

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Breast cancer is the most common malignant tumor among women worldwide, and is the second most common cause of cancer-related death in females after lung cancer in the United States, and after thyroid cancer in Korea.1 The five-year survival rate of breast cancer has been reported to be as high as 89.5%.2 However, without early detection and appropriate treatment, this type of cancer can metastasize via the bloodstream and lymphatic vessels to the entire body, resulting in serious consequences.1
The current National Comprehensive Cancer Network guidelines have identified the estrogen receptor (ER) to be an important prognostic indicator of disease-free survival and overall mortality in individuals with breast cancer.34 Moreover, the presence of ERs and progesterone receptors (PRs) are important factors influencing the design of treatment strategies and patient prognosis. Approximately 3–10% of ER-negative breast cancers respond to anti-hormone therapy, whereas the response rate in ER-positive cancers is as high as 50–60%. In particular, ER- and PR-positive breast cancers demonstrate high improvement rates to anti-hormone treatment (75–80%).56 A 55–66% of primary breast cancers and 45–55% of metastatic breast cancers express hormone receptors by fluoroestradiol (FES) positron emission tomography/computed tomography (PET/CT).6 Hormone receptor-positive breast cancers—even without additional treatment after surgery—demonstrate higher survival rates than hormone receptor-negative breast cancers with small tumor size, and respond well to anti-hormone therapy.78 Approximately 55% of hormone receptor-positive tumors respond well to anti-hormone therapy compared with 3–10% of hormone receptor-negative tumors, which also demonstrate high toxicity to chemotherapy.56 Ductal carcinomas with ER- and PR-positivity rates according to immunohistochemical staining demonstrate high response rates to anti-hormone therapy.5910 In other words, hormone receptor-positive breast cancers exhibit high survival rates and low recurrence rates.811 As such, hormone receptors in breast cancer patients must be tested because they are an important factor(s) influencing prognosis and treatment.5812
To date, the presence of ERs in individuals with breast cancer has been confirmed through immunohistochemical staining of tumor tissues13; however, there is a limitation in that an invasive biopsy must be performed. In addition, about 20% of patients experience recurrence, and 27% have difficulty identifying all areas where tumors have metastasized due to the nature of breast cancer that can cause distant recurrence in the bone, liver, and brain.14 In addition, variations in receptor status among the primary and metastatic sites make it difficult to determine prognosis and plan treatment in patients with recurrent and/or metastatic breast cancers.15
However, F-18 FES PET/CT is a non-invasive test that can be used to evaluate the distribution and binding of estrogen in several sites and can confirm metastasis at the same time.1617 Although several previous studies have predicted treatment response according to the results of F-18 FES PET, we conducted a pooled analysis of the diagnostic accuracy of F-18 FES PET/CT reported to date to confirm its effectiveness.
Go to : 
METHODS
The aim of the present systematic literature review and meta-analysis was to evaluate whether performing F-18 FES PET/CT in patients with recurrent or metastatic breast cancer to diagnose ER expression in the torso region is safe and effective. A systematic literature review was performed according to the reporting guidelines of the Arbitration Act Handbook, as proposed by the Cochrane Union (Cochrane collaboration) and the Preferred Reporting Items for Systematic Reviews and Meta Analyses group.18 All investigators who participated in the present study were recommended by the Korean Medical Association, including a specialist from the Korean Ministry of Health and Welfare, three experts in nuclear medicine, two in hematology-oncology, one in general medicine, and one in evidence-based medicine. Three separate meetings were held for the experts to establish study selection criteria, review studies for eligibility and select those for inclusion, overview data extraction, and refine and validate the conclusions of the study.
Search methods
The terms “((breast cancer.mp. or breast cancer/) OR (Breast Neoplasms.mp. or breast tumor/)) AND ((fluoroestradiol.mp.) OR (FES.mp.)” were combined to search the Ovid-MEDLINE and Ovid-EMBASE databases to identify keywords for the target population and interventions. Accordingly, the keywords “(FES.mp. OR Fluoroestadiol.mp.) AND (breast cancer.mp. OR breast neoplasms/)” were used to search the Ovid-EMBASE, Ovid-MEDLINE, Cochrane Central Register of Controlled Trials, ClinicalTrials. gov, Koreamed, Korean Information Service System, Research Information Service System, Korea Institute of Science and Technology Information, Kmbase, National Library of Korea, and The National Assembly Library of the Republic of Korea and Kolis databases for relevant studies published between January 1980 and May 15, 2020. A total of 512 articles (0 from Korea, 512 studies from overseas) were retrieved. After excluding 158 duplicate articles, those fulfilling the “PICO” (population, intervention, comparison and outcomes) criteria were selected, as follows: Population, patients with recurrent or metastatic breast cancer; Intervention, F-18 FES PET/CT tests; Comparison, immunohistochemistry and immunological tests; and Outcomes, test-related side effects for safety and diagnostic accuracy, correlation, and agreement for effectiveness (Fig. 1).
Assessment of risk of bias
The quality of the studies was independently assessed by two reviewers according to the Scottish Intercollegiate Guidelines Network methodology checklist.19
Data extraction
Data extraction was performed by two evaluators and repeated several times because eligible studies comprised more than one study type. Selection and categorization of the studies were performed in consultation with other investigators when problem/disagreement resolution was necessary. The data were then categorized according to type, study characteristics, and the reliability of the techniques used. Final extraction of data from validated primary sources was performed by two evaluators.
Statistical analysis
The results of the qualitative analysis of the validity indices of the test were summarized in a table for technical analysis, and a 2*2 table was prepared, and MetaDisc 1.4 used for meta-analysis. Heterogeneity was confirmed using the I2 statistic. When analyzing data, attempts were made to perform a subgroup analysis by classifying intervention tests (i.e., PET/CT), metastasis/recurrence, and metastatic sites. However, because each study did not report medical results according to metastasis/recurrence and metastatic sites, additional results could not be confirmed.
Go to :
RESULTS
Study characteristics
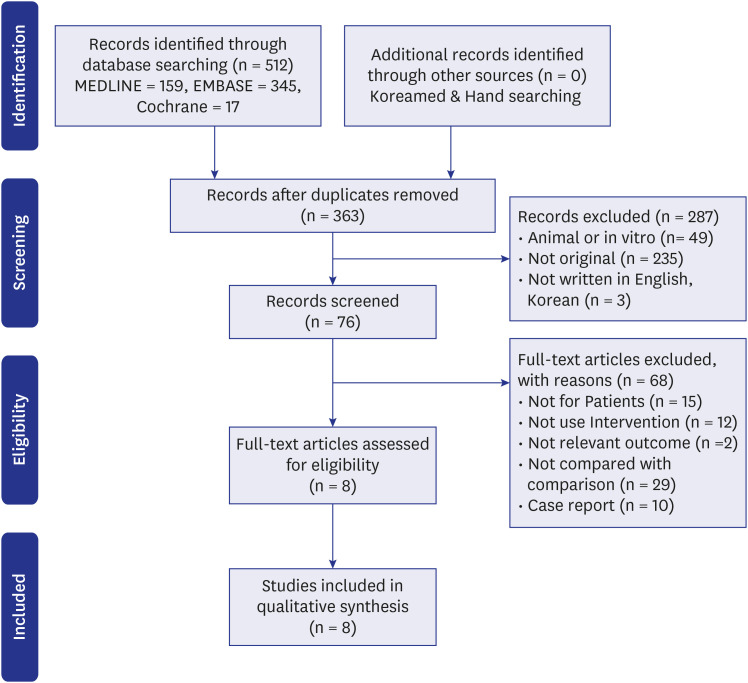
Of the 512 studies retrieved in the literature search, 8 including a total of 284 subjects were ultimately deemed to be eligible.2021222324252627 All selected studies were diagnostic test evaluation studies. Quality assessment yielded three studies with a rating of “2++” and five with a rating of “2+”. In terms of intervention, three studies used PET, and five used PET/CT, all of which reported quantitative results. Immunohistochemistry, a reference standard test, was performed in all studies, in which the cut-off for standard uptake value (i.e., SUV) was ≥ 1.0 in two, ≥ 1.5 in three, and ≥ 2.0 in two (Table 1).
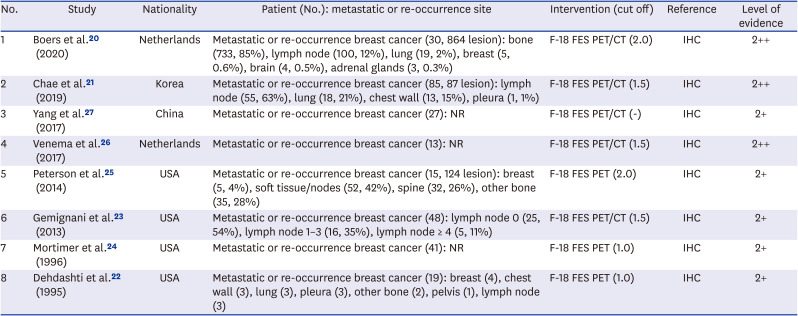
Table 1
Selected studies
| No. | Study | Nationality | Patient (No.): metastatic or re-occurrence site | Intervention (cut off) | Reference | Level of evidence |
|---|---|---|---|---|---|---|
| 1 | Boers et al.20 (2020) | Netherlands | Metastatic or re-occurrence breast cancer (30, 864 lesion): bone (733, 85%), lymph node (100, 12%), lung (19, 2%), breast (5, 0.6%), brain (4, 0.5%), adrenal glands (3, 0.3%) | F-18 FES PET/CT (2.0) | IHC | 2++ |
| 2 | Chae et al.21 (2019) | Korea | Metastatic or re-occurrence breast cancer (85, 87 lesion): lymph node (55, 63%), lung (18, 21%), chest wall (13, 15%), pleura (1, 1%) | F-18 FES PET/CT (1.5) | IHC | 2++ |
| 3 | Yang et al.27 (2017) | China | Metastatic or re-occurrence breast cancer (27): NR | F-18 FES PET/CT (-) | IHC | 2+ |
| 4 | Venema et al.26 (2017) | Netherlands | Metastatic or re-occurrence breast cancer (13): NR | F-18 FES PET/CT (1.5) | IHC | 2++ |
| 5 | Peterson et al.25 (2014) | USA | Metastatic or re-occurrence breast cancer (15, 124 lesion): breast (5, 4%), soft tissue/nodes (52, 42%), spine (32, 26%), other bone (35, 28%) | F-18 FES PET (2.0) | IHC | 2+ |
| 6 | Gemignani et al.23 (2013) | USA | Metastatic or re-occurrence breast cancer (48): lymph node 0 (25, 54%), lymph node 1–3 (16, 35%), lymph node ≥ 4 (5, 11%) | F-18 FES PET/CT (1.5) | IHC | 2+ |
| 7 | Mortimer et al.24 (1996) | USA | Metastatic or re-occurrence breast cancer (41): NR | F-18 FES PET (1.0) | IHC | 2+ |
| 8 | Dehdashti et al.22 (1995) | USA | Metastatic or re-occurrence breast cancer (19): breast (4), chest wall (3), lung (3), pleura (3), other bone (2), pelvis (1), lymph node (3) | F-18 FES PET (1.0) | IHC | 2+ |
NR = not report, F-18 FES = F-18 fluoroestradiol, PET/CT = positron emission tomography-computed tomography, IHC = immunohistochemistry.
![]()
Safety
The safety of the test was evaluated according to test-related side effects, which were reported in two articles: Chae et al.21 reported that nine (10%) patients felt pain with drug injection, with no side effects from the drug; and one reported continuous pain around the injection site. Peterson et al.25 reported no side effects.
Effectiveness
Diagnostic accuracy
Seven articles reported on diagnostic accuracy, in which sensitivity was 0.750–1.000, and specificity was 0.429–1.000.20212223242526 According to intervention tests, the sensitivity of PET (three studies) was 0.750–0.900 and the specificity was 0.429–1.000, whereas the sensitivity and specificity of PET/CT (four studies) were 0.850–1.000 and 0.750–1.000, respectively (Table 2).

Table 2
Sensitivity, specificity, PPV, NPV in each study
| Study | Patient | Intervention | Sensitivity | Specificity | PPV | NPV |
|---|---|---|---|---|---|---|
| Boers et al.20 (2020) | 30 | PET/CT | 0.958 | 1.000 | 1.000 | 0.500 |
| Chae et al.21 (2019) | 85 | PET/CT | 0.851 | 0.789 | 0.833 | 0.811 |
| Venema et al.26 (2017) | 13 | PET/CT | 1.000 | 1.000 | 1.000 | 1.000 |
| Gemignani et al.23 (2013) | 48 | PET/CT | 0.850 | 0.750 | 0.944 | 0.500 |
| Peterson et al.25 (2014) | 15 | PET | 0.750 | 0.429 | 0.692 | 0.500 |
| Mortimer et al.24 (1996) | 41 | PET | 0.762 | 1.000 | 1.000 | 0.800 |
| Dehdashti et al.22 (1995) | 19 | PET | 0.900 | 0.778 | 0.818 | 0.875 |
PPV = positive predictive value, NPV = negative predictive value, PET/CT = positron emission tomography-computed tomography.
![]()
A meta-analysis investigating diagnostic accuracy revealed a pooled sensitivity of 0.86 (95% confidence interval [CI], 0.80–0.91; I2, 29.7%), a pooled specificity of 0.85 (95% CI, 0.76–0.92; I2, 41.8%), and a pooled area under the receiver operating characteristic curve (AUC) of 0.9100. According to intervention, three studies that used PET reported a pooled sensitivity of 0.79 (95% CI, 0.64–0.90; I2, 0.0%), a pooled specificity of 0.94 (95% CI, 0.79–0.99; I2, 63.2%), and a pooled AUC of 0.9190, while four studies that used PET/CT reported a pooled sensitivity of 0.89 (95% CI, 0.81–0.94; I2, 42.9%), a pooled specificity of 0.80 (95% CI, 0.66–0.90; I2, 0.0%), and an AUC of 0.8523 (Fig. 2).
Correlation and agreement
Correlation with a reference standard test was reported in two articles,2627 with r values of 0.627 and 0.883. In terms of agreement, one article21 reported a positive agreement of 76.6% and a negative agreement of 100.0% (Tables 3 and 4).


Table 3
Correlation
| Study | Patient | Intervention | r | P value |
|---|---|---|---|---|
| Yang et al.27 (2017) | 27 | PET/CT | 0.627 | < 0.001 |
| Venema et al.26 (2017) | 13 | PET/CT | 0.883 | < 0.001 |
![]()
Table 4
Agreement
| Study | Patient | Intervention | Positive | Negative |
|---|---|---|---|---|
| Chae et al.21 (2019) | 85 | PET/CT | 76.6% (62.0–87.7) | 100.0% (90.8–100.0) |
![]()
Go to :
DISCUSSION
Breast cancer is the most common malignant tumor among women worldwide, and has a high incidence of recurrence through metastasis via the bloodstream and lymphatic vessels. Although invasive biopsy in bone, liver, and brain is often difficult, metastasis is among prognostic factors of the disease. In addition, the presence of ERs in breast cancer patients is known to affect treatment and prognosis. Accordingly, this systematic literature review and meta-analysis investigated the effectiveness of F-18 FES PET/CT, which can noninvasively confirm ER expression.
Safety was evaluated according to test-related side effects. Although nine (10%) subjects reported pain during drug injection, no side effects from the drug were experienced. Pain is reported in approximately 10% of injections involving radioactive materials, and is a generally expected response. However, no side effects due to F-18 FES occurred in this study. Radiation dose of nuclear medicine imaging is generally minuscule, since extremely small amount of radiopharmaceutical is used for the purpose of diagnosis. No case has been reported about radiation related side effects from diagnostic nuclear medicine scan for over the last half a century. In very rare cases there can be an allergic reaction to the chemical to which the radioactive isotope is attached to. Patients who reported pain in the injection site in the analyzed articles are most likely to be caused by mechanical injury from needle injection not by administration of radioactive materials. Safety was considered to be acceptable.
Regarding effectiveness, diagnostic accuracy was evaluated first, with a sensitivity of 0.750–1.000, a specificity of 0.429–1.000, a pooled sensitivity of 0.86 (95% CI, 0.80–0.91), a pooled specificity of 0.85 (95% CI, 0.76–0.92), and a pooled AUC of 0.9100.
Magnetic resonance imaging (MRI) and ultrasound are widely used noninvasive modalities to confirm metastasis. However, the sensitivity of ultrasound is only 50–86%,28293031 and the sensitivity, specificity, positive predictive value, and negative predictive value of MRI is 67–85.7%, 54–89%, 43–92.3%, and 75–80.9%, respectively.2829303132 Compared with noninvasive tests, the heterogeneity of this test, with invasive biopsy as the reference standard, was < 50%, the pooled sensitivity was 0.86 (95% CI, 0.80–0.91), and pooled specificity was 0.85 (95% CI, 0.76–0.92), thus demonstrating high diagnostic accuracy. As an alternative to overcoming inherent error(s) of subjective interpretation due to differences in diagnostic accuracy in areas reported as limitation(s) of ultrasound and morphological characteristics based on subjective judgment, the test can be more useful than the reported diagnostic accuracy in clinical practice.30 However, because the anatomical test site reported in the literature to date is the torso region, it will be necessary to further analyze studies investigating tests performed at other sites.
F-18 FES PET/CT demonstrated high diagnostic accuracy compared with standard biopsy-based tests. As such, it is anticipated to be useful in informing treatment planning and prognosis of breast cancer patients in the future.
Go to :
 XML Download
XML Download