

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Atherosclerotic coronary artery disease is one of the main causes of death worldwide. Since the first successful balloon angioplasty for coronary artery stenosis in 1977,1 percutaneous coronary intervention has come a long way in terms of interventional devices and technical aspects. Drug-eluting stents (DESs) reduce the rate of in-stent restenosis compared with bare metal stents (BMSs). However, the apparent increase in late stent thrombosis remains a major concern.2 The polymer used for drug coating onto a metallic alloy is associated with arterial inflammation and late stent thrombosis.345 Furthermore, polymer degradation and consequent fragmentation can cause serious adverse events, including arterial embolism.67
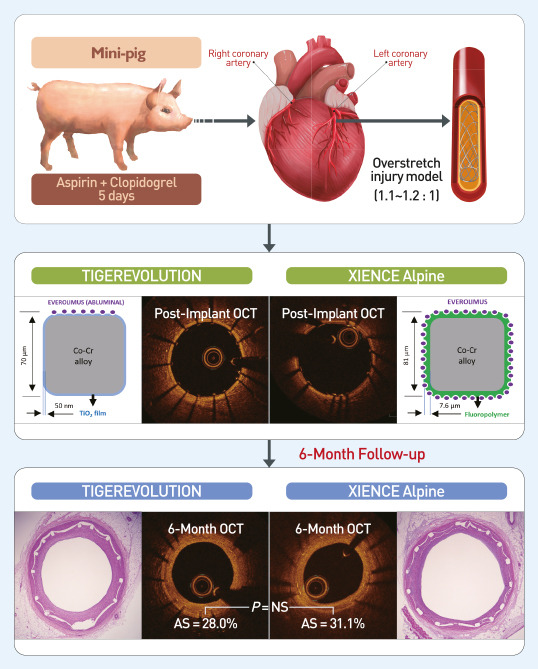
The authors previously developed a novel method to coat a drug onto a titanium dioxide (TiO2) film without a polymer to avoid the problems associated with polymer-based DES.89 Furthermore, a new polymer-free everolimus-eluting stent was developed using this technology, as well as a new BMS (TIGER®; CGBio, Seoul, Korea), named the TIGEREVOLUTION® stent (TIGER EVerOlimus eLUting stent using TIO2 thiN film; CGBio).101112
In this study, we investigated the efficacy and safety of the TIGEREVOLUTION® stent in comparison with a commercial durable polymer-based DES (XIENCE Alpine®; Abbott Vascular, Santa Clara, CA, USA) using 6-month follow-up coronary angiography, quantitative coronary analysis (QCA), optical coherence tomography (OCT), and histopathological analysis in a porcine coronary restenosis model.
Go to : 
METHODS
Preparation of a TiO2 film-coated stent with everolimus (TIGEREVOLUTION®)
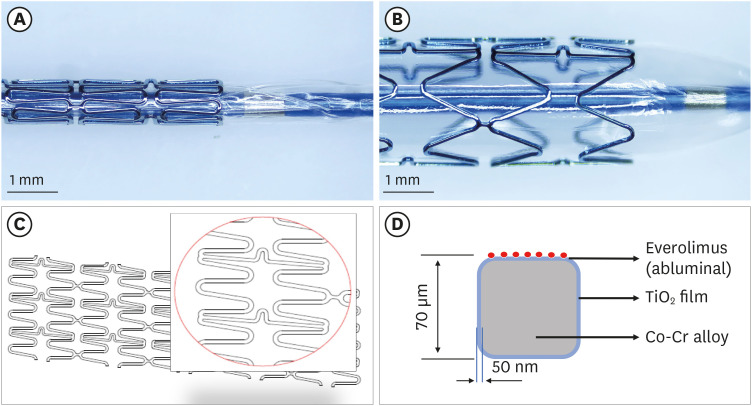
A new BMS with excellent mechanical performance (TIGER®) was designed using a cobalt-chromium-based alloy because it is stronger and more biocompatible than stainless steel.12 The cobalt-chromium tube was cut using a laser cutter (Rofin, Starcut, Hamburg, Germany), followed by ultrasonic cleaning with acetone, ethanol, and distilled water. The tube was then subjected to heat treatment and polishing. The plasma-enhanced chemical vapor deposition process was used to deposit TiO2 thin films onto the BMS. When the TiO2 thin film was deposited at a discharge power of 5 W, it showed a highly smooth surface with a surface roughness of 9.4 nm, mechanical stability, good adhesion, and blood compatibility. The TiO2 film was surface-modified with water plasma to introduce hydroxyl groups onto the TiO2 surface. Subsequently, everolimus (LC Laboratories, Woburn, MA, USA) was grafted to the abluminal surface through the formation of ester bonds between the hydroxyl groups of the modified TiO2 film and the carboxyl groups of everolimus. The “method for manufacturing of drug-releasing stent coated with titanium-oxide thin film” has been granted a United States patent (No. US 8,999,456 B2). The surface morphology of the stent with nitrogen-doped TiO2 film deposition was investigated using scanning electron microscopy, which demonstrated a homogenous coating, with no evidence of cracks after stent expansion.13 The configuration and structure of the stent strut before and after balloon inflation are illustrated in Fig. 1A-C. The stent strut and coating thickness of the TiO2 film were 70 µm and 50 nm, respectively (Fig. 1D).
Study protocol
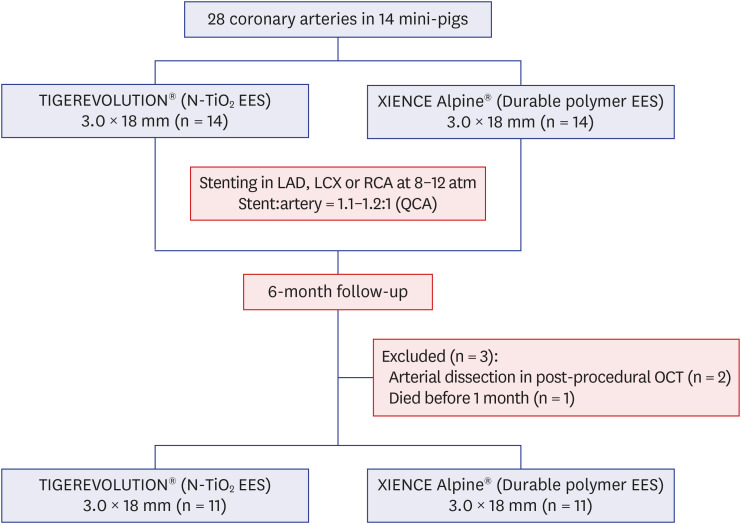
The study animals were mini-pigs (Micropig® T-type male swine; Apures, Pyeongtaek, Korea) weighing between 15 and 20 kg. The exclusion criteria for the analysis included post-procedural complications such as major arterial dissection, which had the potential to affect the outcomes, and other major events that were judged to be relevant to the outcomes. Aspirin (100 mg) and clopidogrel (75 mg) were administered daily for 5 days before the procedure. On the day of the procedure, the pigs were anesthetized with zolazepam and tiletamine (2.5 mg/kg; Zoletil50; Virvac, Caros, France), xylazine (3 mg/kg, Rompun; Bayer AG, Leverkusen, Germany), and azaperone (6 mg/kg, Stresnil; Janssen-Cilag, Neuss, Germany). An oxygen mask was used to supply continuous oxygen. Continuous hemodynamic monitoring, including electrocardiography, was performed during the procedure. Left carotid artery cutdown was performed under local anesthesia, and a 6 French sheath was inserted. An intravenous bolus of 5000 U of heparin was administered, and the coronary artery was engaged using six French guiding catheters. Baseline coronary angiograms were obtained using a nonionic radiocontrast agent in two orthogonal views. Fourteen TIGEREVOLUTION® stents and 14 commercial everolimus-eluting stents (XIENCE Alpine®) were implanted in the coronary arteries of 14 mini-pigs. QCA (Caas Workstation; Pie Medical imaging B.V., Maastricht, the Netherlands) was performed to establish suitable coronary arterial locations amenable to stent implantation. Two different types of stents were implanted in one mini-pig. The stent was deployed by inflating the balloon with an intended stent-to-artery ratio of 1.1–1.2:1. Coronary angiography, QCA, and OCT were performed immediately after stenting. All pigs received aspirin 100 mg and clopidogrel 75 mg orally per day throughout the study period. Follow-up coronary angiography, QCA, OCT, and histopathological studies were performed 6 months after stenting. Pigs that had major arterial dissections on postprocedural OCT or died before 6 months were excluded. Ultimately, 11 mini-pigs were included in the final analysis. The study scheme is illustrated in Fig. 2. Assessments of QCA, OCT, and histopathologic findings were performed based on anatomical naming, and the analyzers were blinded. All stents were implanted at the Animal Laboratory of the Chonnam National University Hospital in the morning (9 AM to 12 AM) from September 2018 to November 2019.
OCT
OCT was performed using a 2.7 C7 Dragonfly Imaging Catheter (LightLab Imaging Inc., Westford, MA, USA). The catheter was placed in the native artery distal to the stented lesion. Automatic pullback at a speed of 20 mm/s was performed during continuous automatic flushing of iodixanol (VisipaqueTM, 320 mg I/L; GE Healthcare, Amersham, UK) at a rate of 2–5 mL/sec, using a Medrad injector (Medrad Inc., Warrendale, PA, USA). Qualitative and quantitative measurements were performed using OCT to assess the stented area immediately after stent implantation and at the 6-month follow-up. OCT images were analyzed at 1-mm longitudinal intervals in a blinded fashion. Volumetric analysis was performed to measure the stent area, lumen area, and neointimal hyperplasia area. Area stenosis was defined as the average area of stenosis in the entire stent.
Histopathologic analysis
The specimens were embedded, and sections of 10–20-µm thickness were obtained at a distance of approximately 1 mm. Then, these were stained using hematoxylin and eosin and Carstairs' method. Histopathologic measurements were performed using a calibrated microscope, digital video imaging system, and microcomputer program (Visus 2000 Visual Image Analysis System, IMT Tech, CA, USA). The measurements were made on five cross-sections from the proximal and distal ends and three midpoints of each stented segment. Scores for injury, inflammation, and fibrin were calculated as previously described.141516 Immunohistochemical analysis was performed to identify cluster of differentiation 31 (CD31)-positive cell expression, a marker of endothelialization. Non-specific reactivity was blocked using 3% fetal bovine serum in phosphate-buffered saline for 60 minutes. Immunohistochemistry was performed using a polyclonal anti-CD31 antibody (1:100; Abcam, Cambridge, MA, USA). Streptavidin Alexa Fluor® 488-conjugated anti-rabbit immunoglobulin G (1:1,000; Invitrogen, St. Louis, MO, USA) was used as the secondary antibody for fluorescence microscopy. Images were captured using a Nikon Eclipse 80i fluorescence microscope (Nikon, Tokyo, Japan).
Statistical analysis
Data were presented as mean ± standard deviation. Unpaired Student's t-test was used to compare the values between the stent groups. Statistical significance was set at P < 0.05. Statistical analysis was performed using R software (version 4.0.3; R Foundation for Statistical Computing, Vienna, Austria).
Ethics statement
The study protocol and procedures for the care of the animals were approved by the Institutional Animal Care and Use Committee of Chonnam National University Hospital (approval no. CNU-IACUC-H-2018-5). The animal study conformed to the Guide for the Care and Use of Laboratory Animals of the US National Institutes of Health (NIH Publication No. 85-23, revised 1996) and the ARRIVE Guidelines for Reporting Animal Research.
Go to :
RESULTS
Drug release kinetics
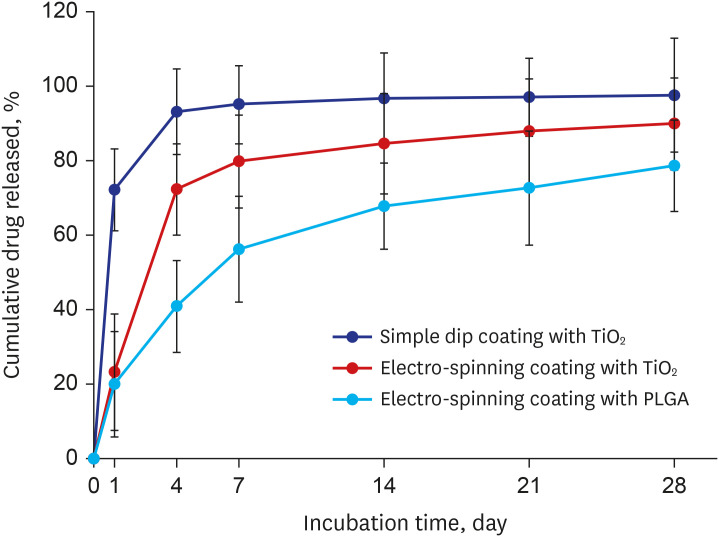
The grafted quantity of everolimus was measured (Supplementary Method). This was followed by an in vivo drug release test as described previously.8913 The release rate of everolimus was lower in the electrospinning coating groups (25.2% ± 11.4% and 19.2% ± 15.0% in the TiO2 and poly(lactic-co-glycolic acid) (PLGA) groups, respectively) on day 1 of incubation compared with the simple dip coating group (75.1% ± 11.4%) (P < 0.001) (Fig. 3). Everolimus was released continuously over a 4-week period, with a higher release rate within the first 7 days in the TiO2 groups (96.4% ± 16.4% and 85.2% ± 14.6% in the simple dip coating and electrospinning group, respectively) than in the PLGA group (58.2% ± 17.6%).
Coronary angiography and QCA
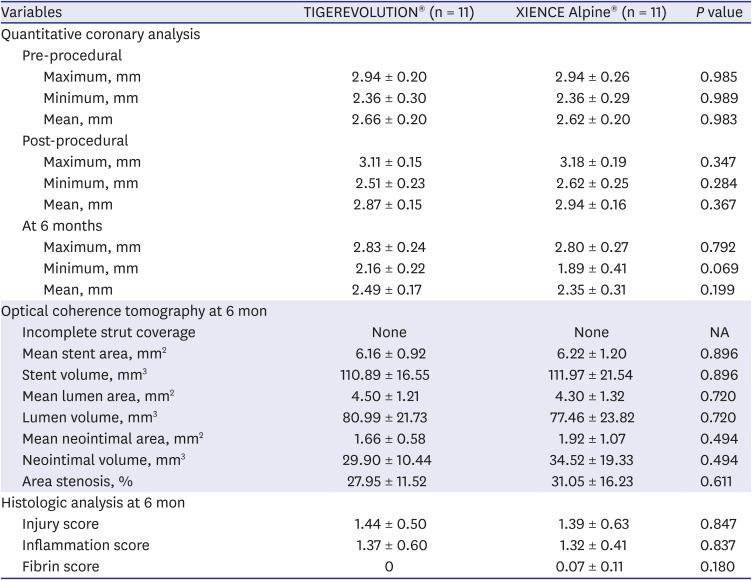
The total number of implanted stents was 28. From these, 22 stents were included in the final analysis (Fig. 2). The stented arteries were patent in both groups immediately after stent implantation and at the 6-month follow-up (Fig. 4A-H). Periprocedural QCA showed no significant difference in the lumen diameter between the groups (preprocedural, 2.66 ± 0.20 mm in the TIGEREVOLUTION® stent vs. 2.62 ± 0.20 mm in the XIENCE Alpine® stent, P = 0.983; postprocedural, 2.87 ± 0.15 vs. 2.94 ± 0.16 mm, respectively; P = 0.367). There was also no significant difference in the lumen diameter at 6 months between the groups (2.49 ± 0.17 mm in the TIGEREVOLUTION® stent vs. 2.35 ± 0.31 mm in the XIENCE Alpine® stent; P = 0.199) (Table 1).
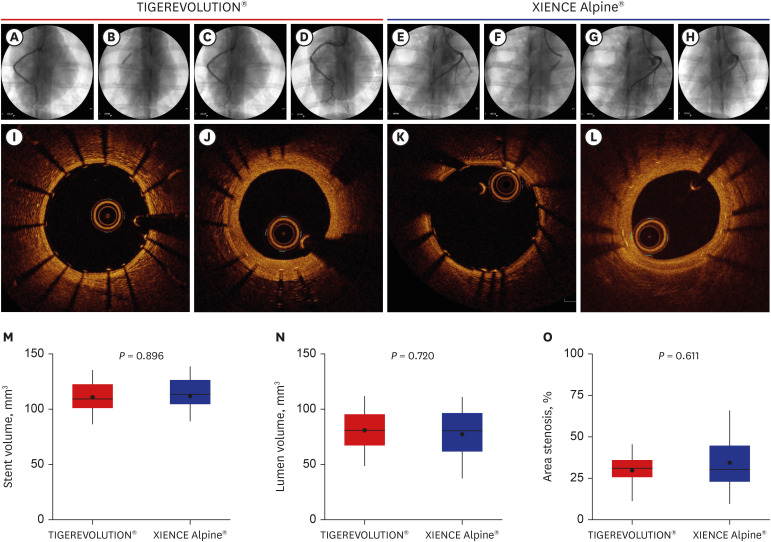 | Fig. 4Efficacy of the TIGEREVOLUTION® stent. Coronary angiographic images of the TIGEREVOLUTION® stent (A) pre-implantation, (B) during implantation, (C) post-implantation, and (D) at the 6-month follow-up. Coronary angiographic images of the XIENCE Alpine® stent (E) pre-implantation, (F) during implantation, (G) post-implantation, and (H) at the 6-month follow-up. OCT images of the TIGEREVOLUTION® stent (I) post-implantation and (J) at the 6-month follow-up. OCT images of the XIENCE Alpine® stent (K) post-implantation and (L) at the 6-month follow-up. Volumetric analysis of the OCT images at the 6-month follow-up: (M) stent volume, (N) lumen volume, and (O) percentage area stenosis. The box displays the median value with an interquartile range. The black points represent mean values.OCT = optical coherence tomographic.
|
Table 1
Quantitative coronary analysis, optical coherence tomography, and histologic analysis between the groups
Values are presented as the mean ± standard deviation.
Area stenosis = (stent volume – lumen volume)/stent volume × 100%.
NA = not applicable.
![]()
OCT
OCT was performed immediately after stent implantation and revealed no significant malappositions or fractures of the stents (Fig. 4I and K). The OCT findings at 6 months demonstrated no dismantling of the stents or thrombi in the stented arteries. The images revealed a homogeneous intra-stent area, suggesting neointimal hyperplasia (Fig. 4J and L). In volumetric analysis of OCT, there was no significant difference in stent volume, lumen volume, and neointimal volume (stent volume, 110.89 ± 16.55 mm3 in the TIGEREVOLUTION® stent vs. 111.97 ± 21.54 mm3 in the XIENCE Alpine® stent, P = 0.896; lumen volume, 80.99 ± 21.73 mm3 vs. 77.46 ± 23.82 mm3, respectively, P = 0.720; and neointimal volume, 29.90 ± 10.44 mm3 vs. 34.52 ± 19.33 mm3, respectively, P = 0.494). Furthermore, the percentage area of stenosis was not significantly different between the groups (27.95% ± 11.52% in the TIGEREVOLUTION® stent vs. 31.05% ± 16.23% in the XIENCE Alpine® stent, P = 0.611) (Table 1 and Fig. 4M-O).
Histopathologic analysis
Representative histological images are shown in Fig. 5A-F. There were no significant differences in the injury score and inflammation score between the groups (injury score, 1.44 ± 0.50 in the TIGEREVOLUTION® stent vs. 1.39 ± 0.63 in the XIENCE Alpine® stent, P = 0.847; inflammation score, 1.37 ± 0.60 vs. 1.32 ± 0.41, respectively, P = 0.837) (Table 1 and Fig. 5G and H). Although the fibrin score was not significantly different between the groups, it was zero in the TIGEREVOLUTION® stent (0 vs. 0.07 ± 0.11, P = 0.180) (Table 1 and Fig. 5I). The expression of CD31 was also not significantly different between the groups (97.8 ± 3.8 in the TIGEREVOLUTION® stent vs. 95.8 ± 5.8 in the XIENCE Alpine® stent, P = 0.282) (Fig. 6).
 | Fig. 5Histopathologic analysis at the 6-month follow-up. Representative photomicrographs of hematoxylin and eosin staining of the TIGEREVOLUTION® stent (A: magnitude × 20) and XIENCE Alpine® stent (D: magnitude × 20), and high-power images (B and E: magnitude × 200). Carstairs' fibrin stain of the TIGEREVOLUTION® stent (C) and the XIENCE Alpine® stent (F) (magnitude × 20). Injury score (G), inflammation score (H), and intimal fibrin score (I). The box displays the median value with an interquartile range. The black points represent the mean values.
|
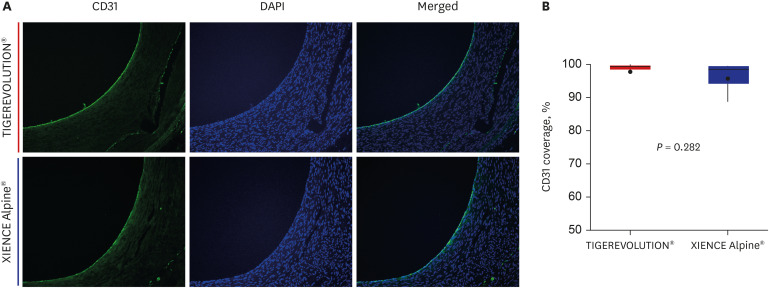 | Fig. 6Endothelialization evaluation of the TIGEREVOLUTION® stent and the XIENCE Alpine® stent at the 6-month follow-up. (A) Immunohistochemical staining of CD31 (bright green positive cells) and DAPI (magnitude x 100). (B) Percentage of CD31 coverage of the TIGEREVOLUTION® stent and the XIENCE Alpine® stent. The box displays the median value with the interquartile range. The black point displays the mean value.CD31 = cluster of differentiation; DAPI = 4′,6 diamidino-2-phenylindole.
|
Go to :
DISCUSSION
In the present study, we used a porcine coronary restenosis model to investigate the efficacy and safety of the TIGEREVOLUTION® stent in comparison with a commercial durable polymer-based DES (XIENCE Alpine®; Abbott Vascular). Using optical coherence tomographic and pathologic analysis, the TIGEREVOLUTION® stent showed comparable results with the XIENCE Alpine® stent at the 6-month follow-up. Although the fibrin score was not significantly different between the groups, it was zero in the TIGEREVOLUTION® stent group. Moreover, immunohistochemical staining revealed that the expression of CD31 was not significantly different between the groups.
DES significantly reduces the rates of in-stent restenosis by inhibiting neointimal tissue proliferation compared with BMS.1718 However, higher rates of late and very late stent thrombosis in DES remain the major disadvantages in practical use compared with BMS.19202122 Therefore, prolonged dual antiplatelet therapy is recommended to prevent stent thrombosis in patients receiving DES implantation unless there are contraindications such as excessive risk of bleeding.23 The polymer used for drug coating onto a metallic alloy provides controlled drug release, but it is also associated with hypersensitivity reactions and late stent thrombosis.3456 Polymer-free DES may be a promising device-based strategy in a complex growing population of patients with a combined high bleeding risk and high thrombosis risk, owing to the possible shortened duration of dual antiplatelet therapy.24 Urban et al.25 recruited 2466 patients with high bleeding risk and randomized them to BMS or polymer-free DES (BioFreedom®, Biosensors Europe, Morges, Switzerland) groups under a dual antiplatelet duration of 1 month. At 390 days, the composite of cardiac death, myocardial infarction, or stent thrombosis occurred in 112 patients (9.4%) in the polymer-free DES group and in 154 patients (12.9%) in the BMS group (risk difference, 3.6 percentage points; 95% confidence interval, −6.1 to −1.0; hazard ratio, 0.71; 95% confidence interval, 0.56 to 0.91; P < 0.001 for non-inferiority and P = 0.005 for superiority). Furthermore, a polymer-free DES was superior to a BMS with respect to the clinically driven target revascularization (risk difference, −4.8 percentage points; 95% confidence interval, −6.9 to −2.6%; hazard ratio, 0.50; 95% confidence interval, 0.37 to 0.69; P < 0.001).
Several years ago, we developed a new BMS (TIGER®), which has high flexibility and a thin stent strut (70 µm).101226 We have evaluated the safety and efficacy of various DESs in both human and animal studies for a long time.272829 More recently, a novel drug-combining method on a stent surface using nitrogen-doped TiO2 film deposition was developed. Titanium exhibits good biocompatibility and mechanical properties. It is commonly used in dental and orthopedic devices. Nan et al.30 fabricated a non-stoichiometric TiO2 film using ion-beam-enhanced deposition. They reported that the blood compatibility of the heat valve materials was improved by TiO2 film coating. Windecker et al.31 reported that titanium-nitride-oxide-coated stents had superior biocompatibility to stainless steel stents in terms of platelet adhesion and fibrinogen binding. In the present study, the TiO2 film was deposited onto the BMS via a plasma-enhanced chemical vapor deposition process. Its applicability as a drug-coating matrix was demonstrated to be a promising alternative to the polymers of DESs.89 Moreover, the release rate of everolimus was faster with the use of a polymer-free TiO2 film than with the conventional PLGA polymer, despite the fact that it was attenuated via the electrospinning coating method. Furthermore, the TIGEREVOLUTION® stent showed comparable results with a commercial durable-polymer everolimus-eluting stent (XIENCE Prime®, Abbott Vascular) with regard to the drug release rate.1332
We initially assessed the efficacy of a polymer-free DES coated with everolimus using nitrogen-doped TiO2 film deposition in a porcine coronary restenosis model with a 4-week follow-up.13 This preliminary study included four stent groups, including BMS (group I; TIGER®), BMS (TIGER®) with nitrogen-doped TiO2 film deposition (group II), commercial everolimus-eluting stent (group III; XIENCE Prime®), and polymer-free everolimus-eluting stent using nitrogen-doped TiO2 film deposition (group IV: TIGEREVOLUTION®). The results showed that the percentage area of stenosis was lower in groups III and IV than in group I (30.2% ± 11.7% vs. 29.2% ± 8.9% vs. 46.4% ± 13.8%, respectively, P = 0.005). However, the fibrin score was higher in groups III and IV compared to groups I and II (2.27 ± 0.24 vs. 1.75 ± 0.31 vs. 0.87 ± 0.67 vs. 0.76 ± 0.61, respectively, P < 0.001). Injury and inflammation scores were not significantly different among the four groups. In the present study, we performed OCT 6 months after stent implantation to accurately compare the percentage area of stenosis between the TIGEREVOLUTION® stent and the XIENCE Alpine® stent in a mini-pig model. The results demonstrated no significant difference in the percentage area of stenosis between the groups, as assessed by OCT. Recently, an investigational new drug application for the TIGEREVOLUTION® stent was approved by the Korean Food and Drug Administration on July 31, 2020. Furthermore, a pilot study of the TIGEREVOLUTION® stent involving 20 humans is being performed in 2021 with the support of the Korea Medical Device Development Fund.
The present study has some limitations. First, an inherent limitation is that the stent was implanted in the normal porcine coronary artery in an oversized manner, which is a scenario different from atherosclerotic coronary restenosis in humans. Second, the selection of the artery to be stented was chosen not based on web-based randomization but on the suitability for implanting the stent by QCA results. Moreover, the limited resources of the animal study were considered. Third, although OCT assessment was performed by two analysts and blinded using anatomical naming, differences in stent platform might affect the results of the analysis.33 Furthermore, information on intra- or interobserver variability was not included. Fourth, we did not consider potential confounders such as cholesterol levels, although we controlled for the order of procedures and measurements. Finally, we were unable to verify the cause of death in one pig.
In our preclinical study, the novel polymer-free everolimus-eluting stent using nitrogen-doped TiO2 film deposition, the TIGEREVOLUTION® stent, had results comparable with those of a commercial durable polymer everolimus-eluting stent, the XIENCE Alpine® stent, in 6-month OCT and histological findings in a mini-pig model.
Go to :
 XML Download
XML Download