

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Anaphylaxis is a life-threatening medical emergency, and its prevalence is on the rise worldwide, highlighting the importance of treatment, prevention, and management in communities.123 Food, drug, insect, and bee venom are the typical causes of anaphylaxis, but the incidence of these common causes varies between studies. In children, anaphylaxis is most commonly caused by food intake.456 Patients are given a thorough education about avoiding causative food allergens and contamination risk to prevent anaphylaxis.78 However, there are cases of anaphylaxis caused by inevitable exposure to the allergen through meals from childcare facilities and restaurants.9 In adults, drug and bee venom are common causes of anaphylaxis.4 Pre-hospital treatment is crucial for these cases of anaphylaxis, as anaphylaxis caused by drug allergy often involves a drop in blood pressure and is often fatal, and exposure to bee venom is during outdoor activities.10
Prompt epinephrine intramuscular injection is the most crucial aspect in the treatment of anaphylaxis. Anaphylaxis is marked by systemic skin, respiratory, gastrointestinal, cardiovascular, and neurological symptoms, as the causative antigen activates mast cells, including histamine, leading to a quick release of mediators that cause systemic vasodilation and mucosal swelling. Epinephrine, which can quickly resolve all of these symptoms, is the treatment of choice.7811 Therefore, for early self-treatment, it is important to prescribe one or more epinephrine autoinjectors (EAIs) for patients at potential risk.71213
In South Korea, the 119 emergency medical service team (EMST) is responsible for basic life support and patient transport.14 Healthcare providers, including nurses, and the first- and second-level emergency medical technicians (EMTs) are qualified to become 119 EMST. However, as per Article 33 of the Enforcement Rule of the Emergency Medical Service Act,15 epinephrine intramuscular injection can be given by 119 EMST with the assistance of physicians (e.g., via video calls). However, it has not been authorized for the treatment of anaphylaxis, even in 2021. There have been continuous voices to, at least, partially expand the scope of practice for 119 EMST to include epinephrine intramuscular injection in anaphylaxis pre-hospital management,1617 and the National Fire Agency Korea launched the pilot project of special EMST (SEMST) in July 2019 and expanded the project nationwide in December of the same year. An SEMST comprises the first- and second- level EMTs and nurses. Among them, some first-level EMTs and nurses who completed special education are authorized to administer intramuscular epinephrine for anaphylaxis with assistance of physicians via a video call. Improvements in anaphylaxis pre-hospital management since the launch of this pilot project are yet to be evaluated.
The need for pre-hospital anaphylaxis management has rarely been studied. In this study, we attempted to examine whether establishing 119 SEMST as a pilot project and authorizing them to administer epinephrine indeed improved anaphylaxis treatment and to identify further needs in the field. Further, we administered an education program about anaphylaxis to evaluate the effectiveness in Gangwon-do 119 EMST, which serves in one of the largest rural areas in South Korea. We evaluated the effectiveness of the education through a survey in order to present valuable data for enhancing the quality of pre-hospital anaphylaxis management and community health care.
Go to : 
METHODS
Online questionnaire survey
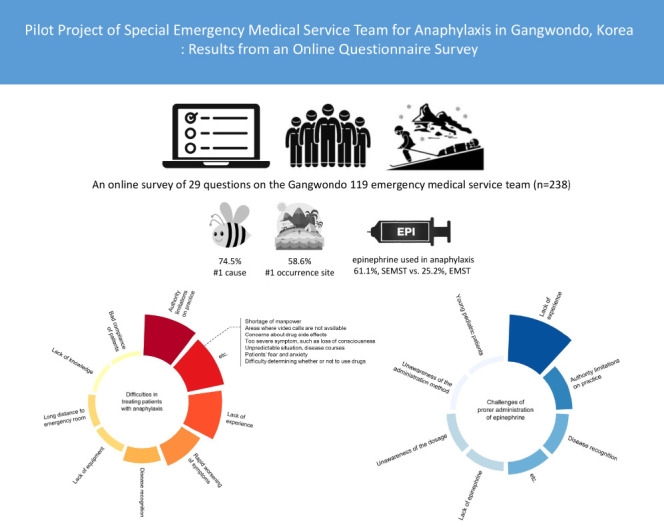
An online questionnaire survey was administered to 119 EMST in Gangwon-do from November 2020 to December 2020. The online survey was developed by allergists, and data were collected via Google Forms on a professional account. The online poll was reached via a hyperlink. The collected data were secured on protected computers with limited access to the members of the Gangwon-do Atopy · Asthma Education Information Center. Participation was anonymous and voluntary. Questions in different categories were asked. The first category was about participants' characteristics, including sex, age, and qualifications; first-level EMT, second-level EMT, and medical personnel (e.g., nurses), work experience, career as SEMST: current, former, never been, experience of anaphylaxis and pediatric anaphylaxis. The second category consisted of questions about participants' knowledge of the diagnosis and treatment of anaphylaxis. The third category was about participants' experiences with anaphylaxis, primarily asking about the cause, place, treatment, including epinephrine injection and patient's possession of EAI. The fourth category consisted of an open question about the difficulties in pre-hospital anaphylaxis management. The total number of questions was 29, with one open-ended, seven close-ended-multiple-choice, and all other close-ended-single-choice questions.
Statistical analysis
All variables were categorical, and therefore, number (%) was presented. For variables with multiple responses, all responses were summed and presented as percentages. Yates' continuity correction was used to adjust for the differences in the probability value by analyzing noncontinuous categorical data with a χ2 test. Statistical analyses were performed using the IBM SPSS Statistics ver. 20.0 (IBM Co., Armonk, NY, USA) and R ver. 4.0.3, and statistical significance was set at P < 0.05.
Ethics statement
This study was approved by the Institutional Review Board of Kangwon National University School of Medicine and the requirement for informed consent was waived (IRB No. KNUH-2021-02-019).
Go to :
RESULTS
Characteristics of participants
Of the 960 questionnaires, 428 (44.6%) were retrieved. The participants consisted of 153 first-level EMTs (35.7%), 209 second-level EMTs (48.8%), and 66 medical personnel (15.4%). A total of 251 (58.6%) participants had field experience of three years or more. Ninety-nine (23.1%) currently served in the SEMST, while 37 (8.6%) had served in the SEMST in the past. Among all responders, 55.6% (238/428) had experienced anaphylaxis pre-hospital management, 12.6% of whom (30/238) were dispatched more than five times a year. Only 3.8% (9/238) had experience with pediatric (≤ 12 years) anaphylaxis pre-hospital management (Table 1).
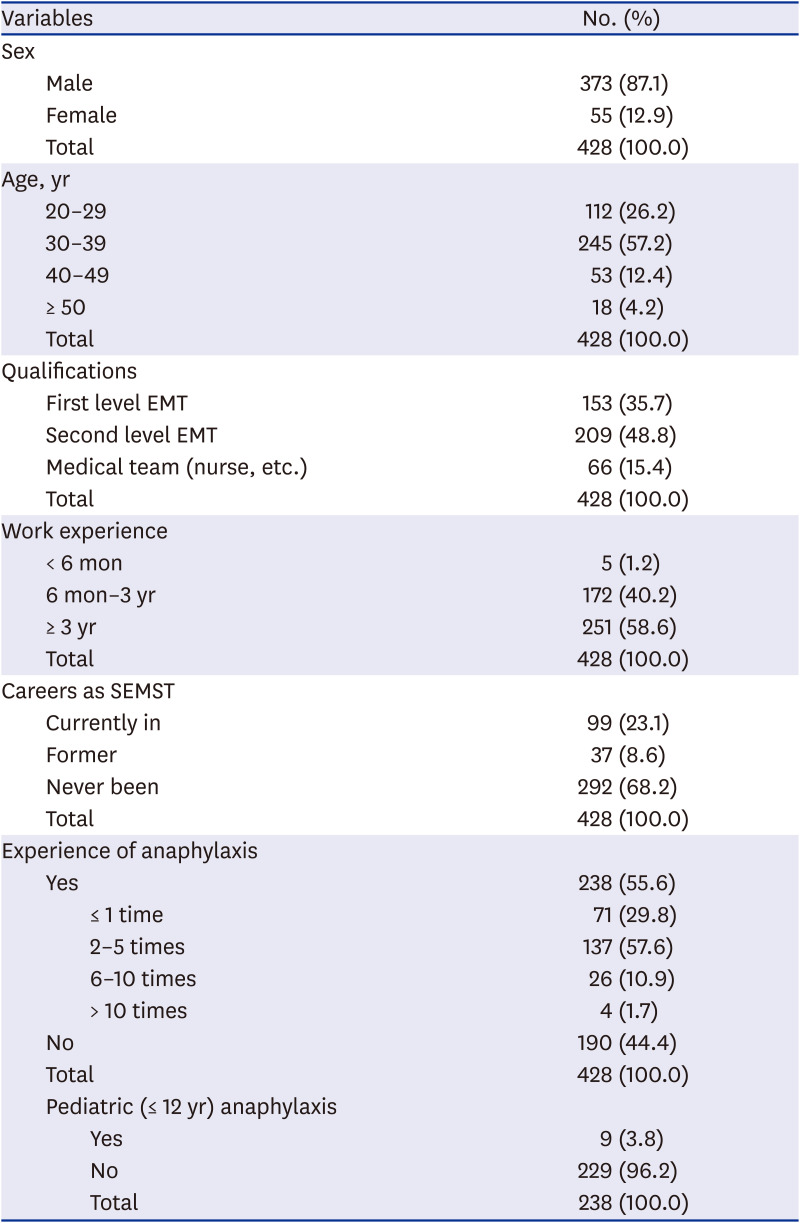
Table 1
General characteristics of responders
![]()
Recall based causes and pre-hospital management of anaphylaxis among participants with experience in anaphylaxis
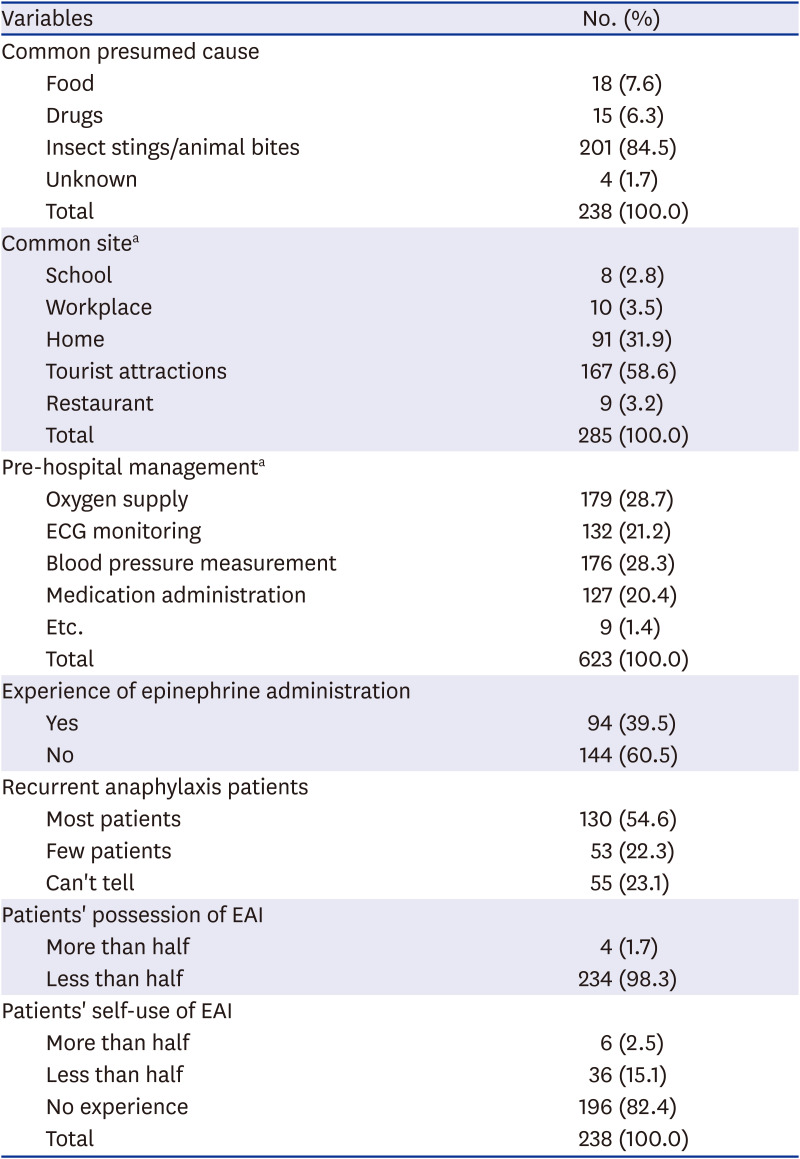
Participants with experience in anaphylaxis pre-hospital management were asked about the suspected cause of anaphylaxis, and 84.5% (201/238) chose insect sting/animal bites, followed by food (7.6%, 18/238) and drug (6.3%, 15/238). Common locations of occurrence (multiple responses, n = 285) included tourist attraction (outdoors) (58.6%, 167/285), home (31.9%, 91/285), workplace (3.5%, 10/285), restaurant (3.2%, 9/285), and school (2.8%, 8/285). Common types of pre-hospital management, also a multiple-response question (n = 623), included oxygen supply (28.7%, 179/623), blood pressure measurement (28.3%, 176/623), electrocardiogram (ECG) monitoring (21.2%, 132/623), and drug administration, including epinephrine (20.4%, 127/623). Ninety-four participants (39.5%) had experienced epinephrine administration. In the question asking whether more than half of the patients encountered during dispatch were considered to have recurrent episodes with prior anaphylaxis history, 130 (54.6%) said yes. However, only four (1.7%) participants answered yes to whether more than half of the patients possessed an EAI. Forty (17.6%) participants encountered a patient in possession of an EAI, and 36 (90.0%) of them stated that less than half of these patients used the device on their own (Table 2). Regarding the frequency of epinephrine administration among 238 participants with experience in anaphylaxis pre-hospital management, 61.1% people in the past or current SEMST group (SEMST+, 58/95) and 25.2% in the non-SEMST group (SEMST−, 36/143) had administered epinephrine, showing a significantly higher percentage in the SEMST+ group (Fig. 1).
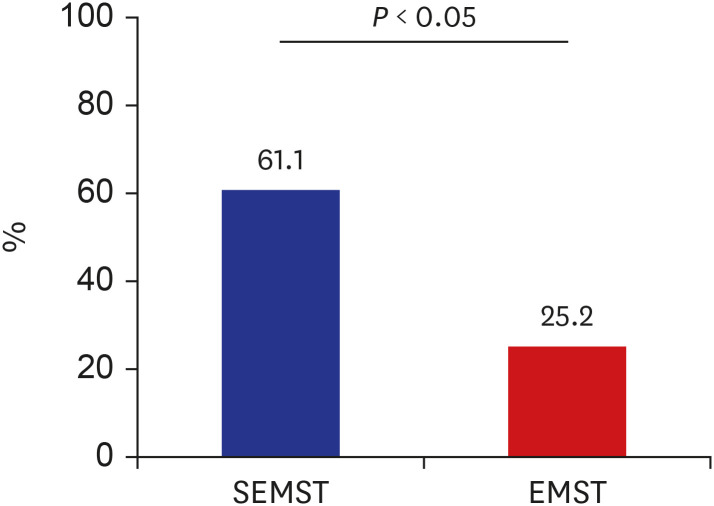 | Fig. 1Rates of epinephrine administration experience. The χ2 test with Yates' continuity correction.SEMST = special emergency medical service team, EMST = emergency medical service team.
|
Table 2
Recall based causes and pre-hospital management of anaphylaxis among participants with anaphylaxis experience
![]()
Effectiveness of education programs and correct response rates for questions about the diagnosis and management of anaphylaxis
A total of 374 (87.4%) participants completed anaphylaxis education programs offered at the Gangwon-do Atopy · Asthma Education Information Center, and 339 (91.6%) of these had completed the education in the past two years. Correct response rates for the question about diagnosis were significantly higher in the educated (24.9%, 93/374) than in the non-educated group (11.1%, 6/54) (Fig. 2A). Answer rates for the question about treatment were also significantly higher (two times) in the educated group (73.5%, 275/374) than in the non-educated group (37.0%, 20/54) (Fig. 2B).
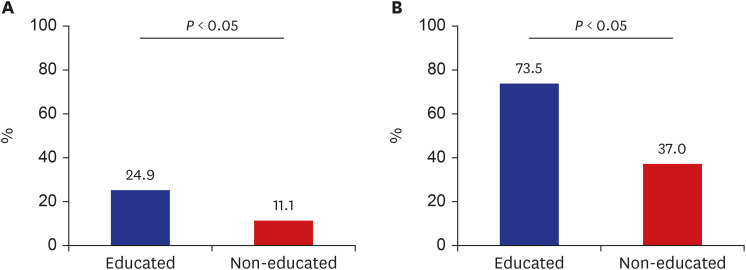 | Fig. 2Participants' knowledge of the diagnosis and treatment of anaphylaxis. (A) Correct response rates for the question about diagnosis of anaphylaxis (educated group: n = 375; non-educated group: n = 54). (B) Correct response rates for the question about treatment of anaphylaxis (educated group: n = 375; non-educated group: n = 54).
|
Difficulties in pre-hospital anaphylaxis management
Difficulties in treating patients with anaphylaxis were surveyed using an open-ended question, and 94 (22.0%) answered the question. The most common challenge was authority limitations on practice, as mentioned by 22 participants (23.4%). Other difficulties included lack of experience (n = 18, 19.1%), rapid worsening of symptoms (n = 12, 12.8%), and disease recognition (n = 8, 8.5%) (Fig. 3A). For the multiple-response question about difficulties in treating children with anaphylaxis, 75.9% (368/485) chose lack of experience, followed by management (12.0%, 58/485) and disease recognition (6.8%, 33/485) (Fig. 3B). For the multiple-response question about the challenges of proper administration of epinephrine, 72.9% (342/469) chose lack of experience, followed by authority limitations on practice (13.9%, 65/469) and disease recognition (5.1%, 24/469) (Fig. 3C).

Go to :
DISCUSSION
Prompt epinephrine intramuscular injection is the treatment of choice for anaphylaxis, and epinephrine administration during pre-hospital management not only significantly lowers disease severity but also reduces mortality. As a result, delayed administration of epinephrine in anaphylaxis is a major risk factor for mortality.1819 The time of epinephrine administration based on arrival at the emergency department (ED) for anaphylaxis in rural areas in South Korea is 32 minutes, which is longer than 21 minutes in urban areas.20 This means that pre-hospital management, including epinephrine administration, is particularly necessary. The results of this study showed that SEMST had significantly more experience (more than two-fold) with epinephrine administration than non-SEMST rescue teams, suggesting that the pilot project of SEMST for anaphylaxis, which emphasizes enhanced authority, is effective in improving pre-hospital management. Therefore, it should be expanded and established in South Korea. A notable 25.2% of the participants not in the SEMST also specified to have administered epinephrine, suggesting that its administration by unauthorized providers is inevitably done with physicians' assistance. This rate ranged from 8.3% to 33.3% in previous studies,2122 and the higher rate observed in this study is presumably attributable to the features of Gangwon-do, characterized by large mountainous areas and a long time from dispatch to arrival at the ED. Still, many participants specified experience and limited authority as the major difficulties with pre-hospital management, and treatments such as oxygen supply, blood pressure measurement, and ECG monitoring were performed prior to medication administration in pre-hospital anaphylaxis management, raising concerns for undertreatment risk. Enhancing authority is crucial for proper treatment, and this need was especially high in rural areas. This highlights the need to consider expanding authority in rescue teams.
The side effects of intramuscular epinephrine injection include paleness, tremor, palpitations, and headache, but most are temporary.2324 However, administering a high dose may lead to emergencies, such as ventricular tachycardia and elevation of blood pressure, and incorrect administration may also lead to tissue necrosis.25 Therefore, lack of experience may be a barrier to epinephrine administration despite continuous education. Thus, it is necessary to increase the stability of administration by equipping teams with EAI or prefilled syringes by body weight and providing continuous and periodic education, along with simulation-based programs that resemble real-life situations.
According to Korean study data, food is the major cause of anaphylaxis, and drugs are also common causes.426 However, in this study, 84.5% of the participants chose insect sting/animal bites as the cause of anaphylaxis, with only 7.6% choosing food as the cause. In addition to recall bias, the difference in these data may be attributable to the fact that past studies were chart reviews or registry analyses of patients who presented to the ED using their own vehicles or other routes and hospitalized, while our study was a survey of anaphylaxis cases reported to the 119 EMST. However, we believe that the major reason for this gap is pertinent to the features of Gangwon-do, the region of this study. Gangwon-do is a rural area located on the eastern side of the Korean peninsula, featuring large mountainous areas, the lowest population density, and high dependence on tourism and agricultural industries.27 Regarding commonplaces of occurrence, 58.6% chose tourist attraction sites, which is different from the results of a previous Korean study25 and a European study,28 where the most common place of occurrence was home. Cases of anaphylaxis in rural areas differ from those in urban areas, and one such difference is high prevalence.29 The fact that more than half of our survey had experience with pre-hospital anaphylaxis management supports this result. Moreover, the common causes and places of anaphylaxis occurrence differed from those reported in previous studies, suggesting the need to reflect regional features in the general care of rural area anaphylaxis. However, the format of the questionnaire that requires answers to its categorized questions to be made between Yes or No made it unable to distinguish between insect stings and animal bites. This caused the study to be limited in its inability to identify the specific problematic antigen and characteristics of symptoms, which warrants future research.
About 87.4% of the participants completed an education program about anaphylaxis, which is a marked improvement from the 119 EMST anaphylaxis educated rate (16.0%) in the Gangwon-do Atopy · Asthma Education Information Center surveyed and reported in 2017.30 In addition, disease knowledge also significantly differed according to prior education, with a nearly two-fold higher correct answer rate for the method of epinephrine administration among educated EMTs. In the 2017 disease knowledge evaluation, there were issues regarding the low correct answer rate for items pertaining to disease recognition and treatment administration, even among those who had been educated, which seems to be an outcome of ameliorating the education project to include theory and practical training led by allergy specialists. This has contributed to the improved awareness observed in this study. However, participants still reported difficulties in disease recognition and treatment for pediatric anaphylaxis cases due to lack of experience or vague or caregiver-described symptoms, which should be resolved through the use of simulation training. In addition, the continuously low rate of correct answers regarding disease awareness demonstrates that by assigning SEMST the responsibility to determine whether EAI administration is required may hinder appropriate treatment. Thus, it is advisable to expand their authority to enable prompt administration on treating the disease, while systemizing physicians' assistance such as video calls.
The fact that many patients did not have an EAI despite having recurrent episodes of anaphylaxis and the low self-use rate among those who had one is an issue to be addressed by physicians. Physicians should prescribe EAI for anaphylaxis prevention and strive to eliminate the barriers to self-use by utilizing different education tools.
One limitation of this study is that it is a survey relying on participant recall and that the response rate was low. In addition, the questionnaire used in this study has never been previously used; therefore, its validity and reliability have not been established. Nevertheless, this study is significant as the first effectiveness evaluation of the pilot project of SEMST for anaphylaxis, assessing the entire rescue team in the rural region of study using the same tool, and enrolling a large sample. Moreover, our findings serve as grounds for supporting the effectiveness of the SEMST project, which has begun the restructuring of authority.
In conclusion, proper administration of epinephrine is particularly important for pre-hospital anaphylaxis management in rural areas. Expanding SEMST with the authority to administer epinephrine and conducting periodic education using virtual experiences is necessary. Implementing prefilled syringes by body weight and utilizing video-based assistance materials to further expand SEMST would enable safer and more appropriate epinephrine administration in anaphylaxis pre-hospital management.
Go to :
 XML Download
XML Download