

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Positive surgical margins (PSMs) were observed in 14–23% of prostate cancer (PCa) patients who underwent a radical prostatectomy (RP) between 2000 and 2011.1 However, over time, the proportion of PSMs has gradually decreased; since 2010, it has been maintained at approximately 10%.2
PSMs can result from inadvertent capsular incisions into otherwise organ-confined tumors or the failure to excise extra-prostatic extensions of PCa, but they can also reflect artifacts induced by tissue processing.345 Nonetheless, PSMs are residual cancer cells on the resected surface, and thus they are adverse pathologic features after RP. They are associated with a higher risk of biochemical recurrence (BCR) in PCa following RP, and they can serve as an independent prognostic factor of BCR.6 Many studies have examined how PSMs affect BCR according to margin location,78 multifocality,910 margin length,11121314 or the Gleason score (GS) at the PSM.1516 However, opinions on whether any of those factors eventually affect cancer-specific mortality (CSM) are controversial.2171819
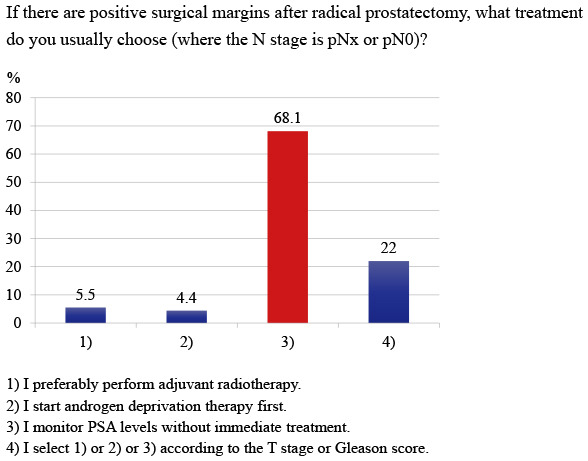
According to the National Comprehensive Cancer Network (NCCN) guidelines, external beam radiation therapy (EBRT) with or without androgen deprivation therapy (ADT) can be applied as adjuvant therapy or a watch-and-wait observation approach can be used for patients with adverse pathologic features such as PSMs, extracapsular extension, or seminal vesicle invasion, so long as no lymph node metastasis is observed in the surgical results.20 EBRT with or without ADT is mentioned as an adjuvant treatment, but in actual clinical situations, there are many cases in which prostate-specific antigen (PSA) does not rise in patients with PSMs, even without any adjuvant therapy.
In randomized controlled trials (RCTs) comparing adjuvant radiotherapy (aRT) and observation in patients with adverse pathologic features, including PSMs, after RP, aRT was found to be beneficial in terms of BCR. However, the results for metastasis and survival were inconsistent.21222324 Also, a meta-analysis of three randomized studies (RADICALS-RT, GETUG-AFU 17, and RAVES) found no evidence that aRT improves event-free survival compared with early salvage radiotherapy (sRT).25
Currently, there is no clear consensus on the optimal treatment with curative intent for patients with PSMs following RP. Therefore, we investigated the perceptions and treatment patterns of Korean urologists regarding resection margin status after RP.
METHODS
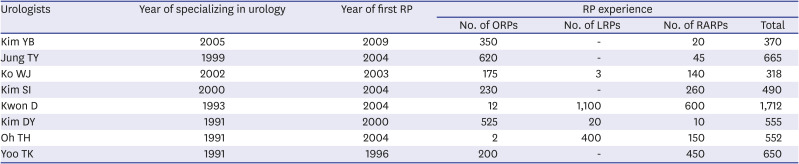
In March 2019, we searched “radical prostatectomy,” “surgical margin(s),” and “resection margin(s)” in PubMed. After classifying the papers by research field and subject matter, we created an initial questionnaire of 14 questions. Eight urologists who had each completed more than 300 RPs modified and deleted questions in the preliminary questionnaire (Table 1 showed detailed characteristics of the eight urologists who participated in creation of the questionnaire). The final questionnaire contained 10 questions about respondents' surgical experience, their usual perception of the surgical margin for RP, and their treatment patterns for patients with PSMs.
Table 1
Detailed characteristics of the eight urologists who participated in creation of the questionnaire
In July 2019, this questionnaire was delivered once via e-mail to 105 urologic oncology specialists in Korea using the Google Forms survey administration app. To increase the reliability of the questionnaire responses, all respondents were asked to provide their names. After the survey was closed, the respondents' names were deleted.
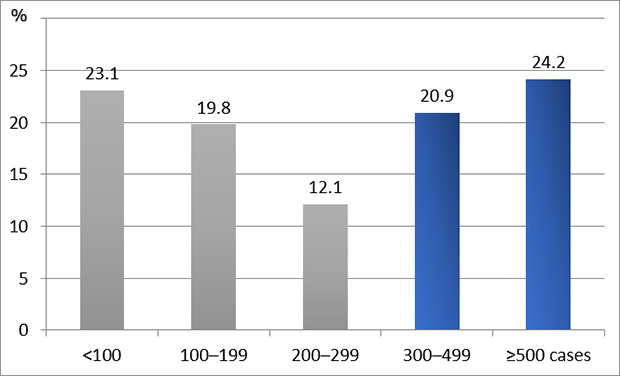
The number of respondents to each question was plotted as a frequency (percentage). For questions 3 and 10, the trend of responses was further analyzed by classifying them into respondents who reported performing 300 or more RPs and those who reported performing fewer than 300 RPs. Frequency analyses and χ2 testing were used. SPSS 18.0 (SPSS Inc, Chicago, IL, USA) was used for statistical analysis, and statistical significance was set at P < 0.05.
The present survey was conducted in accordance with the Helsinki Declaration as revised in 2013.
RESULTS
We received replies from 91 of the 105 (86.7%) urologists we contacted. The survey questionnaires and responses are represented Appendix 1.
Further analysis showed that urologists who had performed 300 or more RPs mainly applied a robot-assisted approach (82.9%), and those less experience used an open retropubic approach (50.0%, P < 0.001) (Table 2).
Table 2
Surgical approach according to doctor experience with RP

| Surgical approach | RP experience < 300 cases | RP experience ≥ 300 cases | P value |
|---|---|---|---|
| Robot-assisted | 18 (36.0%) | 34 (82.9%) | P < 0.001 |
| Laparoscopic | 7 (14.0%) | 3 (7.3%) | |
| Open retropubic | 25 (50.0%) | 4 (9.8%) |
We also found that urologists who had performed 300 or more RPs tended to attempt more nerve-sparing procedures in patients with a high risk of PSMs than less experienced surgeons (36.6% vs. 14.0%; P = 0.012) (Table 3).
Table 3
Preference for nerve-sparing surgery according to doctor experience with RP

DISCUSSION
Survey methodology
E-mail surveys generally have a low response rate (about 30%),26 but the response rate for our survey was 86.7%. A high response rate is both desirable and an important criterion by which the quality of a survey is judged27 because it reflects less-serious potential nonresponse bias.26 We conducted our survey using identified answering. Meade & Craig showed that identified answering of an online survey produced fewer careless responses than anonymous answering.28 Anonymity can afford more accurate reports about sensitive behaviors,29 but because our questionnaire asked for the established professional opinions of individual urologists, there was little concern about acquiring honest answers.
Preoperative considerations
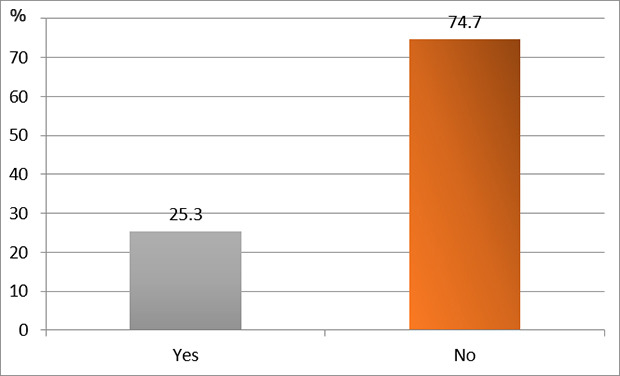
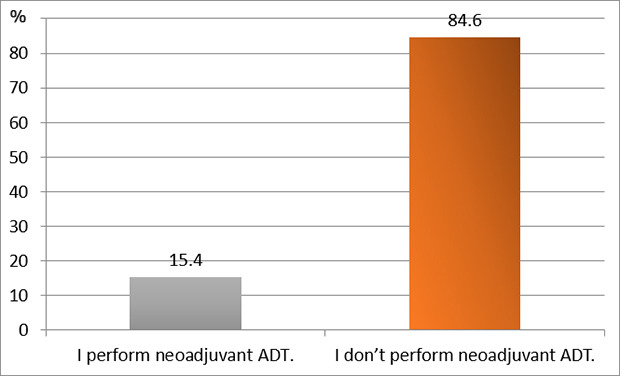
Neoadjuvant ADT (question 9)
Although neoadjuvant ADT might improve oncological outcomes, such as pathological stage and surgical margin status, most randomized studies have failed to show that it improves BCR-free survival or overall survival (OS) after RP.303132 The NCCN guidelines still strongly discourage neoadjuvant ADT for RP outside of a clinical trial.20 In our study, 84.6% of the respondents said that they did not perform neoadjuvant ADT even in high-risk patients. The small effect of neoadjuvant ADT on BCR could result partially from the delay it impinges on surgical intervention, which could allow cancer progression during ADT treatment in the subgroup of patients that is insensitive to ADT. Therefore, identifying the subgroup sensitive to neoadjuvant ADT could be useful. Akitake et al.33 suggested that neoadjuvant ADT had potentially deleterious effects on BCR in patients > 65 years old and patients with low serum testosterone levels (≤ 450 ng/dL), whereas it could improve the prognosis of patients with high serum testosterone levels. McClintock et al.34 reported a consistent decreasing trend in the use of neoadjuvant ADT over time, with the nadir observed in 2011; since then, a modest increasing trend has appeared. They found an association between neoadjuvant ADT and a decreased risk of PSMs, but only among low- and intermediate-risk patients. In high-risk disease, neoadjuvant ADT before RP did not lower the possibility of PSMs and was even associated with worse OS. Appropriate research is needed to determine whether neoadjuvant ADT can be selectively applied according to patient condition or PCa status.
Perioperative considerations
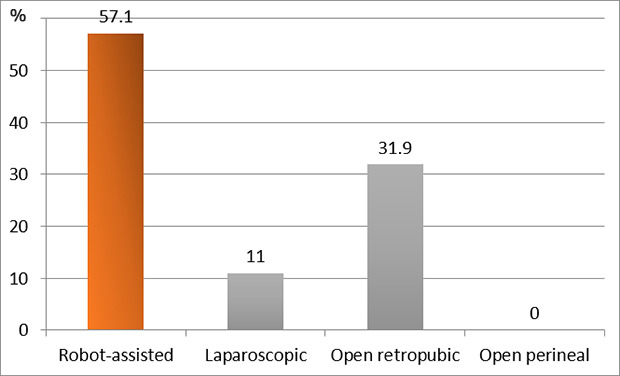
Surgical site approach (robot-assisted vs. laparoscopic vs. open) (question 3)
In a meta-analysis published in 2012, the unadjusted PSM rates were 24.2% in open RP (ORP), 20.4% in laparoscopic RP (LRP), and 16.2% in robot-assisted RP (RARP). After propensity adjustment, the LRP group had higher PSM rates than the RARP group but similar rates to the ORP group.35 In a meta-analysis published in 2018, ORP had a significantly higher rate of PSMs than RARP (odds ratio [OR], 1.18; 95% confidence interval [CI], 1.05–1.32; P = 0.004), but the rate of PSMs did not differ significantly between ORP and LRP (OR, 1.37; 95% CI, 0.88–2.14; P = 0.17) or between RARP and LRP (OR, 0.83; 95% CI, 0.40–1.72; P = 0.62).36 Most of the studies included in those meta-analyses were conducted retrospectively, though some RCTs were included. Guazzoni et al.37 reported that the PSM rates of ORP and LRP were 21.6% and 26%, respectively, which was an insignificant difference (P = 0.28). Yaxley et al.38 compared ORP and RARP and found that the PSM rates (10% and 15%, respectively) did not differ significantly (P = 0.21).
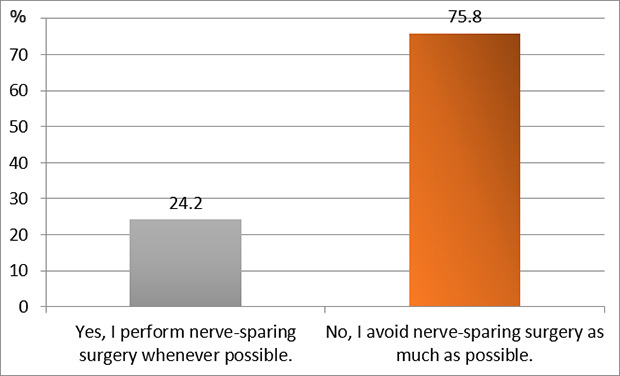
Nerve-sparing surgery (question 10)
1. Nerve-sparing in the high-risk group
In D'Amico high-risk PCa patients (PSA > 20 ng/mL, biopsy GS ≥ 8, or clinical stage ≥ T2c),39 nerve sparing is not traditionally advocated due to the high risk of PSMs, which leave residual disease in situ during RP.4041 However, some authors reported that nerve-sparing was not associated with higher rates of PSM or BCR in patients with preoperatively high-risk PCa who underwent RARP, compared with non-nerve sparing surgery.404142
2. Bilateral vs. unilateral vs. no nerve-sparing
Greco announced that bilateral laparoscopic intrafascial nerve-sparing RP produced better functional outcomes with regard to urinary continence and sexual potency than the unilateral technique, with similar oncological outcomes.43 Kim et al.44 found that the continence return rate was significantly higher in patients with bilateral (93.0%) nerve-sparing RARP than in patients with unilateral (78.1%) or no (76.7%) nerve-sparing RARP, and bilateral nerve-sparing surgery was independently associated with continence return 12 months after surgery in multivariate analysis (OR, 3.67).
The D'Amico high-risk group has a very heterogeneous patient distribution according to three criteria (preoperative PSA, biopsy GS, and clinical T stage), and the selection and application of the nerve-sparing technique also varies by urologist. Although taking the aforementioned findings as a definitive theory has some limitations, sacrificing the neurovascular bundle might not be an essential approach in high-risk patients.
Surgical experience (question 2)
Several studies have reported that PSMs tend to decrease as surgeons gain experience. Although there is variation across studies, the learning curve for surgical margins after RP plateaus at approximately 250 cases, regardless of the approach method.454647 In ORP, the probability of PSMs was 40% for a surgeon with 10 prior cases, which decreased to 25% for a surgeon with 250 prior cases (absolute difference 15%).45 In LRP, there was an apparent improvement in surgical margin rates up to a plateau at 200–250 surgeries, with an absolute risk difference for 10 vs. 250 prior surgeries of 4.8%.46 In RARP, the risk of positive margins decreased from 16.7% to 9.6% in patients treated by a surgeon with 10 and 250 prior procedures, respectively (risk difference 7.1%). In patients with non-organ confined disease, the predicted probability of positive margins was 38.4% in those treated by surgeons with 10 prior operations and 24.9% in those treated by surgeons with 250 prior operations.47
In our study, 82.9% of urologists who had performed 300 or more RPs used a robot-assisted approach. On the other hand, among surgeons with fewer than 300 previous surgeries, 36.0% used a robot-assisted approach, and 50.0% used the open retropubic approach (P < 0.001) (Table 2). Interestingly, urologists who reported performing ≥ 300 RPs tended to attempt more nerve-sparing procedures in patients with a high risk of PSMs than less experienced surgeons (36.6% vs. 14.0%; P = 0.012) (Table 3).
Intraoperative frozen section (IFS) (question 4)
In IFS-related studies, a further resection is performed when PSMs are reported, and various results have been shown according to the site of the IFS. When the IFS sites were determined at the discretion of the operating surgeon, changes in the PSM rate ranged from −12.2% to +11%, compared with the non-IFS control condition.4849505152 Studies applying IFS at the posterolateral margins showed a decrease in the rate of PSMs of 6.5–14.1% compared with non-IFS procedures.535455 Öbek et al.56 investigated IFS at the entire prostate margin and reported that the conversion of a positive margin to a negative one was achieved in 85% of cases, and overall PSMs decreased from 22.5% to 7.5%.
Prognosis according to margin positivity
1. BCR (questions 5 and 8)
Due to the long-life expectancies of men with PCa treated by RP, intermediate markers of postoperative oncologic success are generally used, the most common being BCR.11 PSMs are associated with a higher risk of BCR in PCa following RP and could serve as an independent prognostic factor for BCR.6
1) Margin location (e.g., apex, posterolateral, bladder neck, or anterior)
The overall effect of PSM location on oncological outcomes remains highly controversial, with inconsistent results reported for different RP approaches. In a review of mainly ORP procedures, posterolateral PSMs appear to confer the greatest risk of recurrence, whereas the prognostic significance of positive apical margins was unclear.7 On the contrary, posterolateral margins following RARP carry a smaller risk of BCR than apical margins.8
2) Margin multifocality
A narrative review of studies between 2005 and 2011 noted that whether multifocality confers a greater risk of BCR than unifocality is controversial.9 Wu et al.10 concluded that the presence of multifocal PSMs and multilocal PSMs, and especially the combination of the two, significantly affected BCR prognosis.
3) Margin length
The relationship between PSM length and BCR is somewhat controversial,11 but the risk of BCR seems to increase as the margin length increases.121314 Shikanov et al.12 found that a PSM ≤ 1 mm conferred a BCR probability twice as high as a negative margin (hazard ratio [HR], 2.2; 95% CI, 1.6–3.1), and the BCR probability in patients with a PSM > 1 mm was almost fourfold higher (HR 3.7; 95% CI, 2.6–5.3). Lee et al.,13 on the other hand, reported that a PSM ≤ 3 mm did not significantly affect BCR-free survival (HR 1.2; P = 0.686) compared with a negative margin. They also found that a PSM > 3 mm was significantly associated with BCR-free survival (HR > 2; P < 0.001). Cao et al.14 argued that the accuracy of the BCR prediction was higher when the linear length of a PSM was analyzed as a continuous variable than when it was analyzed as a binary variable, with longer PSM lengths correlating with worse BCR prognoses.
5) pT2R1 vs. pT3aR0
Several studies showed that patients with pT2R1 had a BCR risk similar to that of patients with pT3aR0.575859 Even if the postoperative result shows pT2, when PSMs are present, the prognosis is clearly worse than a pT2 result with a negative margin; in fact, it is close to that of pT3 with a negative margin.
2. CSM
Four large-scale studies have analyzed the relationship between PSM and CSM with long-term follow-up. Two of those studies demonstrated that PSM had a significant effect on CSM (HR 1.45; 95% CI, 1.25–1.68)2 and (HR 1.4; 95% CI, 1.0–1.9).17 However, the other two studies found no significant relationship between PSM and CSM.1819 Mithal et al.19 found that PSMs were associated only with an increased risk of BCR (HR 1.98; 95% CI, 1.75–2.23), and not castration-resistant PCa, metastases, CSM, or OS. Those differences could result from the wide range of time to mortality and other risk modifiers that compete with PSMs and obscure their direct effect on PCa mortality.60
Postoperative considerations
Follow-up strategies (question 7)
The NCCN guidelines recommend that PSA be checked every 6–12 months for 5 years and then every year thereafter, with a digital rectal examination (DRE) every year (which can be omitted if PSA is undetectable) after initial definitive therapy.20
1. Regular check of PSA level
Most postoperative patients who develop distant metastasis and die due to PCa develop BCR in advance, so early detection of BCR is the key in PSA follow-up after RP. Yanai et al.61 created an optimal PSA follow-up schedule after RP on the premise that the ideal PSA range for detection of BCR was 0.2–0.4 ng/mL (Table 4). They suggested that this PSA follow-up schedule could reduce the frequency of PSA measurement while limiting the risk of overlooking BCR. Because BCR occurs more frequently in patients with PSMs, it might be necessary to follow-up more often than the usual examination interval for those patients.
Table 4
Optimal PSA follow-up schedule after RP61

The first column values are PSA at any timing after surgery, and each box indicates the optimal interval for the next PSA measurement according to the timing after surgery.
PSA = prostate-specific antigen, RP = radical prostatectomy.
aPSA monitoring was stopped for patients who had continuously undetectable PSA levels (< 0.01 ng/mL) for 5 years.
2. Radiologic examination for the early detection of recurrence
A palpable abnormality via DRE is not a reliable finding in detecting local recurrences because postoperative fibrosis often mimics recurrent malignancy.62 Computed tomography (CT) and bone scintigraphy are not sufficiently sensitive in the early recurrence setting with low PSA values. Transrectal ultrasonography with biopsy or multiparametric prostate magnetic resonance imaging (MRI) are valuable imaging modalities for the detection of local recurrence, but few data are available at the lowest PSA levels after RP, and those few show a wide range of positivity. Whole-body MRI has high detection rates for pathological lymph nodes, and especially has higher sensitivity than bone scintigraphy for the detection of bone metastases.63 Combined whole-body and multiparametric prostate MRI as a single-step approach is feasible for the simultaneous assessment of local recurrence and metastatic disease after RP.64 The detection rates of the different imaging techniques depend on the PSA level at the time of imaging. Recent advanced imaging techniques can detect the location of the recurrence, even when PSA levels are still very low. At recurrent PSA levels of < 0.5 ng/mL, detection rates up to 31.3% were reported using 11C choline positron emission tomography (PET)-CT and up to 65.0% using 68Ga prostate-specific membrane antigen (PSMA)-11 PET-CT. At recurrent PSA levels < 0.2 ng/mL, the detection rates of 68Ga PSMA-11 PET-CT ranged from 11.3% to as high as 58.3%.63 Given the continuing lack of guidelines for postoperative radiological examination in patients with adverse pathologic features, consensus on a standard approach to the early detection of recurrence is needed.
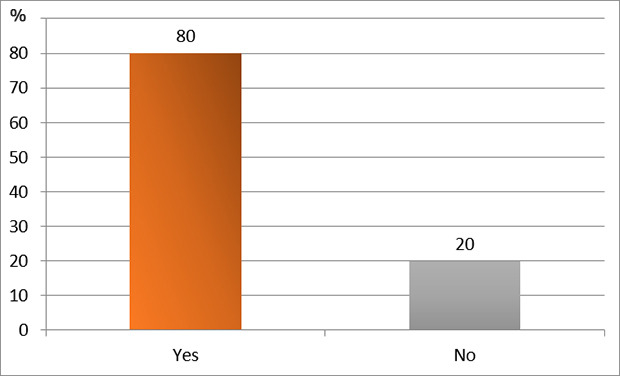
Postoperative treatment: Adjuvant treatment vs. observation (question 6)
The details of postprostatectomy treatment differ slightly in each guideline. The NCCN guidelines recommend that either EBRT or observation be applied for patients with PSMs, extracapsular extension, or seminal vesicle invasion.20 The American Society for Radiation Oncology/American Urological Association guidelines suggest that physicians offer aRT to patients with adverse pathologic findings at RP (Standard; Evidence Strength: Grade A) and offer sRT to patients with PSA elevation or local recurrence after RP (Recommendation; Evidence Strength: Grade C).65 The European Association of Urology-European Association of Nuclear Medicine-European Society for Radiotherapy & Oncology-European Society of Urogenital Radiology-International Society of Urological Pathology-International Society of Geriatric Oncology guidelines were updated as follows in 2021: Do not wait for a PSA threshold before starting treatment. Once the decision for sRT has been made, sRT should be given as soon as possible (strength rating: strong).66
A study analyzing adjuvant treatment trends from 1990 to 2017 for patients with adverse features at RP showed that adjuvant therapy has gradually decreased over time.67 In our study, more surgeons said that monitoring PSA without offering immediate treatment was appropriate for men with PSMs than said that aRT or ADT should be applied.
A meta-analysis of three RCTs (EORTC22911, SWOG8794, and ARO96-02/AUO-AP09/95) compared aRT to a wait-and-see strategy in patients with pT3 or margin-positive PCa.68 The aRT resulted in greater BCR-free survival (HR 0.48) and 10-year metastasis-free survival (OR 0.77). However, there was no survival benefit overall. Compared with the wait-and-see strategy, aRT carried significantly increased toxicity of any grade (50.0% vs. 38.6%), grade 2 or greater genitourinary toxicity (17.1% vs. 10.3%), grade 2 or greater gastrointestinal toxicity (2.5% vs. 1.1%), urinary stricture rates (11.1% vs. 5.7%), and urinary incontinence (6.9% vs. 2.7%). The EORTC and SWOG studies reported on the rate of sRT used in the wait-and-see arm, which was an average of 32.8% in the 2 studies. However, the median PSA concentration at the start of any salvage treatment was 0.75–1.0 ng/mL in SWOG and 1.7 ng/mL in EORTC, and thus those numbers do not represent early salvage but can be seen as late sRT.
In 2020, the results of a meta-analysis of three RCTs (RADICALS-RT, GETUG-AFU 17, and RAVES) comparing aRT and observation (policy of early sRT) in men with localized or locally advanced PCa (including PSMs in the eligibility criteria) were finally released.25 In the observation group, 39.1% had commenced early sRT at the time of analysis. Investigators used a harmonized definition of event-free survival as the time from randomization until the first evidence of either biochemical progression, clinical or radiological progression, the initiation of a non-trial treatment, death from PCa, or a PSA level of at least 2.0 ng/mL. The analysis showed no evidence that event-free survival was improved with aRT compared with early sRT (HR 0.95; P = 0.70). All three trials reported increases in specific side-effects with aRT, including increased urinary morbidity (RADICALS-RT), grade 2 or greater genitourinary toxicity (RAVES), and grade 2 or greater late genitourinary toxicity and erectile dysfunction (GETUG-AFU 17). This systematic review suggests that early sRT would be the preferable treatment policy because it can spare many men RT and its associated side-effects. Our survey was conducted before the results of that meta-analysis were released, and the practice patterns of urologists who participated in our survey are expected to be further supported by those research results.
Although the two reviews just discussed were not conducted solely on patients with PSMs, more than 60% of patients (100% in GETUG-AFU 17) in all six studies included in the reviews had PSMs. It is thought that those data can be sufficiently referenced in policies for postoperative management of PSMs after RP.
Limitations
The most important limitation of our study is that our results do not represent the opinions of all urologists. Only 105 urology specialists in Korea were asked to respond to the questionnaire, which is clearly an insufficient number. However, considering that Korea has only 73 hospitals in which urology residency training is possible and 42 hospitals in which residents were actually trained in Korea in 2019, 105 is not a small number of urologists, proportionally speaking. Furthermore, because each country has different medical infrastructure systems, healthcare systems, and insurance coverage, the application of treatment or testing for PSMs can differ by country. However, most clinicians provide patient care in accordance with common practice guidelines, and therefore, our results have a high possibility of sharing certain global trends in the management of PSMs.
In conclusion, the most common response of Korean urologists was that they monitor PSA levels without providing any adjuvant treatment when PSMs are found after RP. We interpret that response to indicate that they attempt to detect recurrences early through close observation rather than immediately treating PSMs. Through our questionnaire, we found considerable differences in the perceptions and treatment patterns of Korean urologists according to RP resection margin status. Refined research and standardized practice guidelines for PSMs are needed.
 XML Download
XML Download