

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Out-of-hospital cardiac arrest (OHCA) is a leading cause of global mortality.1) Despite rapidly evolving medical care systems for patients with myocardial infarction and stroke, the consequences of OHCA are devastating. The post OHCA survival rate remains under 10%, and often leaves neurological sequelae.2)3)4)5) Its unpredictable occurrence in young people without comorbidities poses a burden to public health as well as their families.
To develop effective interventions for reducing the public health burden, numerous studies have attempted to accurately estimate the number of OHCAs. The most recent studies to investigate OHCAs used multicenter, registry-based data from the European Registry of Cardiac Arrests, Cardiac Arrest Registry to Enhance Survival, Resuscitation Outcomes Consortium Epistry in North America, All-Japan Utstein Registry, and Pan-Asian Resuscitation Outcomes Registry (PAROS), but their reported OHCA incidence rates showed wide disparities—ranging from 40–84 per 100,000 people-owing to regional variations, research time, and inconsistent OHCA definitions.6)7)8)9)10)
The exact OHCA burden is not known since there are numerous episodes which have not been reported in registry studies. Registration can only be performed in hospitals, where voluntary registration by an active physician is possible, but since it was performed by various centers, there could have been errors or selection bias during data collection. In addition, identifying the cause of arrest in those who died was difficult, and follow-up for survivors was often inadequately. To overcome these limitations of registry studies, validation through other research methods is required. We aimed to evaluate the epidemiologic features and outcomes of non-traumatic OHCA on the basis of nationwide population-based data from Korean National Health Insurance System (K-NHIS).
METHODS
Ethical statement
Our study protocol was approved by the K-NHIS and the Korea University Anam Hospital Institutional Review Board (Approval number: 2015AN0362), who waived the requirement of obtaining informed consent since the data were fully anonymized and de-identified.
Data source
This study was conducted using the K-NHIS database. K-NHIS—the sole medical insurer in the Republic of Korea—is managed by the Korean government. While 97% Koreans are the K-NHIS subscribers (~50 million people), the remainder are medical aid subjects. The K-NHIS database includes demographic information, medical claims data, pharmacy dispensing claims, mortality data, and disease diagnoses, as defined by the International Classification of Diseases, 10th Revision (ICD-10). By obtaining participants' disease and medical treatment codes, we were able to retrieve diagnoses related to cardiac arrest. Since ICD-10 codes are classified as primary and secondary diagnoses, the main disease identified by the clinician who actually managed the patients was considered as the primary diagnosis.
Study population and definitions
Our study comprised of data from 2008 to 2017, and included those afflicted by OHCA during this period. In Korea, all OHCA patients are first transported to a hospital's emergency room (ER) by its emergency medical services (EMS) system. Those with cardiac arrest codes (I46.0, I46.1, I46.9, I49.0, R95.0, R96.0, and R96.1) or who had undergone cardiopulmonary resuscitation (CPR) in ERs of nationwide hospitals were enrolled as subjects (Supplementary Table 1). Cardiac arrest or CPR codes assigned in other departments of the hospital were excluded since these were considered as in-hospital cardiac arrest. Those, whose primary diagnosis codes in ER comprised of respiratory arrest (R09.0), gastrointestinal bleeding (K25–29 or K92), cerebral hemorrhage (I60–I62), cerebral infarction (I63–64), septic shock (A40–A41), injury by trauma (S00–S99), and accidents including asphyxiation, anaphylaxis drowning, poisoning, traffic accident, falls, burns, and suicides (T00–T98) were excluded, and classified as having non-cardiac origin arrest. The cause of arrest in those who had died was double-checked by analyzing their death certificates since the main diagnosis related to death needs to be entered in death certificates after the clinician's evaluation during admission or autopsy. The cause of arrest among survivors was analyzed by reviewing their disease, procedures, and surgery codes for the six months following the arrest.
For the validation of the OHCA definition, we screened 215 patients at Korea University Guro Hospital from October 2015 to August 2018 by the aforementioned codes in this research. Among them, 69 patients were excluded as per the non-cardiac origin exclusion criteria. The positive predictive value was 84.9% because the actual OHCAs were 124 cases. Patients' survival discharge rate was 32%.
OHCA caused by coronary artery disease (CAD) was defined based on the myocardial infarction code and a history of coronary intervention or surgical bypass, anytime during the patients' lifetime (Supplementary Table 2). Subjects who were not assigned any CAD codes were categorized as the non-CAD subgroup.
Statistical analyses
Continuous variables were described as the mean±standard deviations and compared using the Student's t-test. Categorical variables were presented as percentile values and compared with either a χ2 test or Fisher's exact test, as appropriate. The total population with national medical health insurance was used as the denominator to estimate the annual incidence rate of OHCA, which was calculated as the number of events per 100,000 person-years. The one-year survival rate was estimated using Poisson regression models. Hazard ratios (HRs)—which are an estimate of the ratio of hazard rates in the comparative versus the reference group (mortality rate in 2008)—with 95% confidence intervals (CIs) were calculated. All significance tests were two-tailed, and a p value ≤0.05 was considered as statistically significant. All statistical analyses were performed using the SAS software version 9.2 (SAS Institute Inc., Cary, NC, USA).
RESULTS
The 10-year trend of out-of-hospital cardiac arrest incidence in Korea
From January 2008 to December 2017, 387,665 patients were transferred to the ER for resuscitation. A flowchart of the study population's enrollment is presented in Figure 1. Around 295,070 OHCA patients were enrolled, excluding those whose arrest was mainly due to non-cardiac causes. The study population's baseline characteristics—184,025 (62.4%) males, with a mean age of 66.2 years—are summarized in Table 1. More than half of them had hypertension. Figure 2 and Supplementary Table 3 present the number of annual episodes of OHCA and changes in its incidence. The OHCA incidence rate was 48.2 per 100,000 in 2008, but steadily increased to 53.8, 60.1, and 66.7 in 2011, 2014, and 2017, respectively.
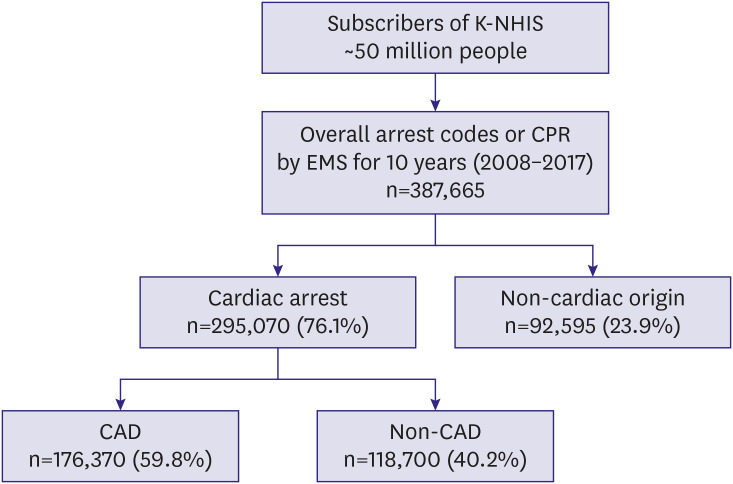
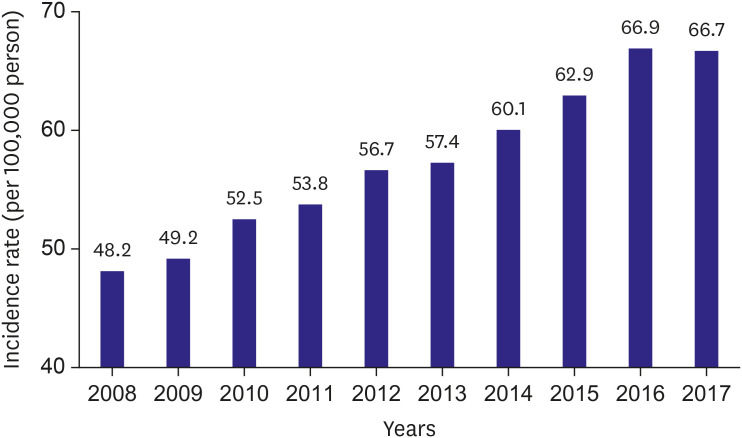
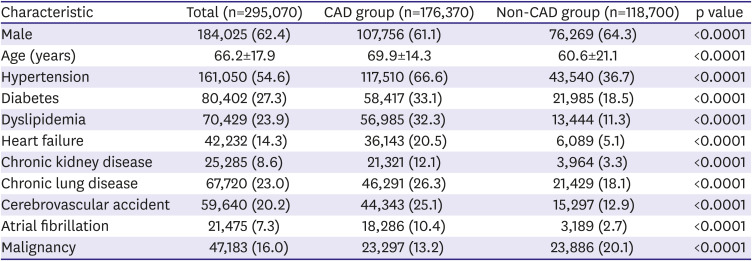
Figure 1
Flowchart of the process used to identify out-of-hospital cardiac arrest and -related etiology.
CAD = coronary artery disease; CPR = cardiopulmonary resuscitation; EMS = emergency medical services; K-NHIS = Korean National Health Insurance System.
![]()
Figure 2
Annual trends in age- and sex-adjusted incidence of out-of-hospital cardiac arrest per 100,000 person-years.
![]()
Table 1
Clinical characteristics of people with out-of-hospital cardiac arrest
![]()
An assessment of 1-year mortality after out-of-hospital cardiac arrest
Around 270,783 people died within 1-year from 295,070 OHCA episodes. Thus, Korea's 1-year OHCA survival rate was 8.2%. To assess the prognosis of OHCA patients, the HR of 1-year mortality was calculated (Table 2), using the 2008 rate as the reference value. Age- and sex-adjusted mortality rates tended to decrease. It was 1.0015 in 2009 (95% CI, 0.9831–1.0203), 0.9865 (95% CI, 0.969–1.0043) in 2012, 0.9769 (95% CI, 0.96–0.9941) in 2015, and 0.9629 in 2017 (95% CI, 0.9831–1.0203) (p value for trend <0.0001).
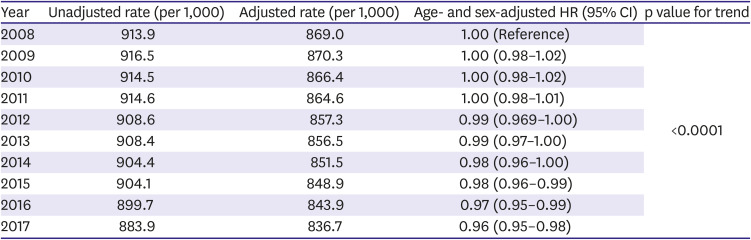
Table 2
One-year mortality rate after out-of-hospital cardiac arrest
![]()
Coronary artery disease as the cause of out-of-hospital cardiac arrest
The baseline demographics of patients with and without CAD as the cause of OHCA are presented in Table 1. While CAD caused OHCA in 176,370 (59.8%) of the overall population, non-CAD OHCA was observed in 118,700 (40.2%) of the population. Patients in the CAD group were more likely to be older with a higher prevalence of hypertension, diabetes mellitus, dyslipidemia, heart failure, chronic kidney disease, chronic lung disease, cerebrovascular accident, and atrial fibrillation; in contrast, those in the non-CAD OHCA group were more likely to be younger, and with a higher prevalence of malignancy.
DISCUSSION
We uncovered a recent 10-year trend of OHCA in Korea using a complete nationwide survey. This study revealed three main findings: 1) the incidence of OHCA has increased steadily over the last 10 years; 2) although the 1-year mortality rate has been gradually decreasing, it was still high; and 3) CAD was the main cause of OHCA and accounted for 60% of OHCA cases.
Most previous studies that evaluated the incidence of OHCA were based on registry data, but their main disadvantage was that patients were mostly registered in large hospitals, while some cases that had occurred in non-participating hospitals were excluded. If a survey is performed within a specific area, the result is affected by regional geographical characteristics or local climate variations.8)11)12) Furthermore, in a registry study, it is difficult to find the cause for the visit to the hospital, especially when patients are brought in dead or there is inadequate time for sufficient examination. To compensate for these weaknesses, a complete nationwide survey was conducted using the K-NHIS database. Since 97% of all Koreans are NHIS subscribers, all OHCAs in the ERs of all hospitals were included in this study. An EMS data-based study by Ro et al. revealed that the per 100,000 person-years OHCA incidence in Korea was 37.5 in 2006, 39.8 in 2007, 42.5 in 2008, 45.6 in 2009, and 46.8 in 2010.13) Our results showed a similar increase in trends but slightly higher incidence. The overall incidence of sudden arrest was 48.7 per 100,000 person-years in a previous study by our group using a sample cohort from K-NHIS.14) The OHCA at institutions which were not included in the EMS data-based registry was a cause for higher incidence in the K-NHIS data-based studies. Although all studies found the OHCA incidence to have increased annually, the causes were uncertain. Additionally, incidence of OHCA steadily increased in other Asian nationwide studies.15)16) We hypothesized that some risk factors for OHCA might have been aggravated. An improved EMS system could increase the number of people who were revivable by resuscitation, given that our definition of OHCA included CPR codes in ER. However, further research into this is warranted.
We analyzed 1-year mortality, unlike other registry studies that only calculated survival discharge rates. OHCA survivors often die from unrestored heart problems or other organ complications, not long after discharge. If neurological sequelae persists, complications such as pneumonia are common. The K-NHIS database reflects the level of the overall health care system in Korea through calculation of mortality rates after one year. In our study the survival discharge rate could be higher since the rate of survival was 8.2% during the 1-year period. The survival rates have gradually improved, despite several studies having shown poor survival rates of less than 10%. The survival discharge rates in Europe North America, Asia, and Australia were 7.6%, 6.8%, 3.0%, and 9.7%, respectively.17)18) Our outcome did not focus on survival discharge rate but on 1-year survival rate, which was higher than that of previous studies. The PAROS study presented finding from seven Asian countries from 2009 to 2012. Korean and Japanese bystander CPR rates were more than 40% and it was 31.4% in Taiwan. These were higher than that of other Asian countries. The survival discharge rate in Korea was highest (8.5%) among all seven countries. The research period of the PAROS study comprises the initial part of our study, during which the bystander CPR rate in Korea had been increasing. A coordinated effort to optimize the effectiveness of the local “chain of survival” leads to a hopeful message. It is necessary to identify and improve additional weak points in the local resuscitation link.19)20)
The survival discharge rates of previous Korean registry data are improving. Ahn et al.21) showed that it was 3.5% in 2005–2006, but Yang et al.22) reported that it was at 9.6% during 2008–2009. In the past 10 years, the bystander CPR rate has increased dramatically owing to the EMS system improvement in Korea. The active expansion of CPR education to the general population and propagation of automated external defibrillator have increased the bystander CPR rate. In addition, extra-corporeal membrane oxygenator becoming more accessible improved survival discharge and long-term outcome. The development of percutaneous coronary intervention and implantable cardioverter-defibrillator implantation can also affect long-term outcome. The successful resuscitation rates after OHCA led to an increase in implantable cardioverter-defibrillator implantation for secondary prevention.23)
In many cases, it is difficult to determine the causes of OHCA. The cause is undefined if resuscitation is unsuccessful, or sometimes it is complex in elderly patients. Thus, our study is beneficial as it identifies the cause of OHCA by reviewing the lifetime of patients in relation to the registry studies. This helped to estimate the cause even if resuscitation had failed. In our study, 59.8% of the OHCA patients were estimated to have CAD, which is lower than that reported by Western data, but higher than that reported in other Asian countries such as Japan.24)25)26) Patients with CAD-related OHCA were relatively older and were exposed to more risk factors than the non-CAD OHCA patients. The prevalence of malignancy was higher in the non-CAD group, which is believed to independently affect OHCA incidence.
Several limitations of our study should be considered when interpreting the results. The main limitation is the general inaccuracy of the definition of OHCA. A disadvantage of claims data-based research is that it relies on ICD codes for diagnosis, and thus validation is difficult. Although OHCA was confirmed by EMS personnel or during hospitalization, the possibility that some OHCA episodes were missed or overestimated cannot be overlooked. ER cardiac arrest cases are not actually OHCA by definition; nonetheless, they may have been included in this study. Non-CAD OHCA, such as sepsis or trauma, was common in these cases. Non-cardiac origin arrest might have been included if the exclusion disease code was not entered in the ER. Second, since database research only collects essential data elements, there is no access to detailed clinical information to assess other factors (e.g., rhythm status or EMS response time) that could influence survival rates. Although the OHCA incidence rate and survival rate were higher than that in previous registry studies, it is possible that several OHCA cases were missed in registry studies; both are complementary information for identifying the epidemiology of OHCA. Third, all patients who had prior CAD diagnosis were classified into the CAD group, even if non-CAD causes had decisively culminated in OHCA; thus, the proportion of CAD-related OHCA could have been overestimated.
In conclusion, this study showed that the incidence of OHCA has increased during the last decade based on a nationwide population-based study. Although the 1-year mortality rate after OHCA is still high, it is gradually decreasing.
 XML Download
XML Download