

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Kawasaki disease (KD) is an acute inflammatory disease characterized by persistent high-grade fever along with certain mucosal and dermatological changes, and generally presents with varying degrees of multi-organ system manifestations including acute vasculitis, myocarditis, pulmonary infiltrates as well as aseptic meningitis mostly in young children and infants.1)2)3)4)5)6)7)8) This phenomenon was first described in Japan where its annual incidence has been substantially higher compared with other geographical regions (for instance; ≍250/100.000 in those <5 years of age in 2011 and 2012).1) Pathogenetically, a substantial immune response induced by specific antigens including viruses possibly accounts for KD evolution mostly through an acute autoinflammatory reaction characterized by a plenitude of activated circulating neutrophils and augmented proinflammatory pathways including interleukin (IL)-1 and IL-6 cascades.1) The most dreaded clinical manifestation appears to be the ‘coronary arteritis’ potentially complicated by subsequent ‘coronary artery aneurysm (CAA)’ formation.1)5)6)7)8) Morphologically, CAA in the setting of KD is defined as an ‘ectatic coronary segment’ with a diameter of >1.5 times that of the reference segment or an echocardiographic Z score of >2.5.1) In this context, harnessing Z score (that universally signifies standard deviation from the avarage) allows adjustment for certain variables including body surface area.1) Therefore, one should not exclusively rely on numerical values (including aneurysm diameter) to define CAAs in children due to the significant variation in their body sizes (and hence; coronary artery diameters at baseline).1) Importantly, coronary artery involvement, besides being an ominous sign, also confirms the diagnosis of KD in cases with incomplete or ambiguous findings.1)
Temporally, CAA evolution in the setting of KD has been universally regarded as an early-onset phenomenon, and is well known to be associated with the severity of the disease course, and in particular; with the failure to initiate disease-modifying strategies including intravenous immunoglobulin (IVIG), etc.in a timely manner.1)8)9) In particular, classical CAAs in the setting of KD have a male gender predilection with an incidence of 25% (in untreated cases) that has declined to around 4% with the initiation of proper management strategies.1) In this paper, the term ‘ early CAA’ signifies classical aneurysms in patients with KD. However, CAA formation in the setting of KD might occasionally arise as a late-onset phenomenon generally presenting with new-onset CAAs or expansion of long-stable ‘early CAAs,’ and might have diverse implications.1)9)10)11)12)13) On the other hand, the diagnostic criteria for early CAAs (including Z score value)1) possibly apply to the diagnosis of these late-onset aneurysms. Of note, it seems likely that ‘late CAAs’ in the setting of KD might be confused with other vascular pathologies (including atherosclerotic CAAs) on coronary imaging, and are possibly underdiagnosed in clinical practice. The incidence of these aneurysms was demonstrated to be 3% in a previous report.10) Within this context, the present paper aims to highlight pathogenetic and clinical implications late CAA formation largely through a comparison with classical ‘early CAAs’ in the setting of KD.
LATE VERSUS EARLY (CLASSICAL) CORONARY ARTERY ANEURYSMS IN KAWASAKI DISEASE: CLINICAL AND PATHOGENETIC INSIGHTS
Temporal and demographic characteristics
Regarding temporal evolution, classical ‘early CAAs’ invariably arise within the first few weeks and reach their maximum diameter by 6 weeks following the KD onset.1)8) This seems in strict contradistinction to the ‘late CAAs’ that usually emerge after a substantial latent period of years to decades.9)10)11)12)13) In a population of 562 patients with KD, 17 late CAAs (15 new-onset and 2 expanding aneurysms) were previously reported in 15 patients (3%) with a male gender predominance (n=11).10) Time at intial diagnosis of these aneuryms was reported to range from 1.9 to 19 years with a median duration of 11.4 years.10)
In a previous case report, a giant CAA (reaching a diameter of 11 mm) at left main coronary artery (LMCA) was attributed to the late expansion of a stable aneurysm at the same site after a period of 11 years in a male patient.11) Within this context, a previous case series reported late CAA evolution in 2 segments of the right coronary artery (RCA) (each having a diameter of around 8 mm) after 10 years following the index KD episode in a boy.12) In this case series, a ‘late CAA’ at the distal part of a long-stable ‘early CAA’ involving the proximal portion of circumflex artery was reported to arise after 28 years following the index KD episode in another male patient.12) Similarly, in a boy with a history of KD episode (around 2 years of age), ‘late CAAs’ were demonstrated on coronary angiograms (CAGs) performed when he was around 8 years (presenting with a new aneurysm in RCA) and around 17 years of age (presenting with 2 other new aneurysms in RCA and left anterior descending [LAD] artery).13) Based on these reports, ‘late CAAs’ in the setting of KD also have a male gender predilection (similar to classical ‘early CAAs’),1)8) and generally arise several years or even decades after the index KD episode.9)10)11)12)13) Accordingly, late CAA formation might be regarded mostly as a disease of adolescents or adults with a history of KD.10)11)12)13)
Mechanistic aspects
Classical early coronary artery aneurysms
Mechanistically, acute and substantial vascular destruction due to severe and multi-layer necrotizing vasculitis is well known to be the hallmark of classical ‘early CAAs’.1)8) These aneurysms might fully or partially regress in time or incur further complications including thrombus formation, significant myofibroblastic proliferation leading to coronary stenosis, etc..1)8) Within this context, acute neutrophilic infiltration (that largely accounts for necrotizing arteritis, and is usually complete within 2 weeks) within the vessel wall gradually replaced by subacute/chronic lymphocytic infiltration (commencing within 2 weeks and lasting for weeks to months) and active subacute/chronic luminal myofibroblastic proliferation (LMP) stage (lasting for months to years) generally characterize the consecutive, yet; intersecting pathological findings of coronary arteritis and subsequent early CAA formation in patients with KD.1)8) Of note, timely initiation of specific therapies including IVIG might completely block or interrupt this pathological cascade at an earlier stage with the potential to prevent or mitigate early CAA formation in this setting.1)8) In particular, ‘early CAAs’ generally involve the proximal portions of major epicardial coronary arteries including proximal LAD artery and LMCA.1)8) Proximal coronary involvement might also denote potential roles of certain hemodynamic factors including dP/dt and blood pressure in the evolution and progression of ‘early CAAs’. This mechanistic implication might also suggest a potential analogy to the genesis of proximal aortic aneurysms. Of note, proximal coronary involvement might allow close monitoring of these aneurysms through serial echocardiographic examinations.1)
Late coronary artery aneurysms
Late CAA evolution long after KD onset has been a poorly understood phenomenon with ill-defined pathological characteristics.9)10)11)12)13) Within this context, ‘late CAAs’ were previously suggested to arise as potential recurrences at the sites of previously regressed ‘early CAAs’ possibly as a result of ongoing pathological and hemodynamic abnormalities including coronary stenosis and somatic growth within the related coronary segments.9)10)11)12)13) In other terms, these abnormalities were suggested to be associated with the eventual formation of late-onset aneurysms at the weakest part of associated coronary segments mostly in an asymmetrical manner.9)10)11)12)13) In a large population of patients with KD, 17 late CAAs (with diameters of 2.0 to 6.5 mm) were reported with 15 of them presenting as new-onset pathologies.10) Of note, 14 of these 15 new-onset CAAs were reported to occur at the proximal portion of major coronary arteries (with 8 aneurysms involving LAD) predominantly at the branches or bifurcation points and mostly in the form of post-stenotic dilatations.10) In this context, bifurcation points were suggested to have specific pathological and hemodynamic characteristics that might facilitate aneurysm formation.10) In particular, 10 of these 15 new-onset aneurysms were also demonstrated to emerge at the sites of previously regressed ‘early CAAs’.10) Interestingly, 5 of these aneurysms were not associated with previous ‘early CAAs’ potentially suggesting alternative yet; obscure mechanisms underlying their evolution. In this large KD series,10) only 2 late CAAs were attributed to the expansion of pre-existing stable ‘early CAAs’. This may suggest that late aneurym formation mostly arises as a new-onset phenomenon in patients with KD.10)
Based on the above-mentioned notions, late CAA formation in the setting of KD might manifest as a ‘late new-onset CAA’ or ‘late expanding CAA’.10) The term ‘late new-onset CAA’ usually denotes a late aneurysm formation at the site of a partially or completely regressed early CAA. On the other hand, the term ‘late expanding CAA’ mostly signifies late expansion of a long-stable ‘early CAA’ (with minimal or no changes in size during several years until expansion).10) In this regard, current reports on late CAA formation have been quite rare in the literature to draw firm conclusions on its pathogenesis and description. Interestingly, localized coronary stenoses (mostly at the proximal or distal site of these aneurysms) might possibly have important pathogenetic implications in the evolution of ‘late CAAs’. On the other hand, evolution of localized coronary stenoses is possibly dependent on partial or complete regression of ‘early CAAs’ which might, in turn, recur as ‘ late new-onset CAAs’ partly due to the adverse hemodynamic impact of emerging coronary stenoses on the vessel wall.10) In other terms, magnitude of early CAA regression mostly through the process of LMP seems to correlate with the degree of localized coronary stenoses.
Conversely, localized coronary stenoses might not be regarded as a characteristic feature of ‘late expanding CAAs’. Consistent with this, a giant aneurysm at LMCA (with a diameter of 11 mm) was reported to arise as a late expanding aneurysm without associated coronary stenosis after 11 years following the angiographic demonstration of a long-stable mild aneurymal dilatation at the same site.11) Nevertheless, localized coronary stenoses might occasionally emerge even in the absence of early CAA regression in the long-term,11) and might contribute to the future evolution of ‘late expanding CAAs’ as well. Accordingly, a 50–75% stenotic lesion at the proximal site of an ever-stable ‘early CAA’ (without significant changes during a period of 17 years) was previously demonstrated on CAG after 17 years following the index ‘early CAA’ evolution.11) In summary, ‘late CAAs’ have been mostly associated with pre-existing ‘early CAAs’ in the setting of KD. However, as described in the next section, evolution of these aneurysms might also arise as a separate entity, and hence; might be quite possible even in the absence of an ‘early CAA’ history in certain patients with KD.
Dysfunctional vascular healing following mild coronary arteritis: an alternative mechanism of late coronary artery aneurysm evolution in patients with Kawasaki disease?
As a novel and reasonable pathological concept, it has been recently suggested that late CAA formation might also arise as a ‘de novo’ and insidious phenomenon (rather than simply manifesting as a recurrence or expansion of ‘early CAAs’ in the long-term) in coronary segments with mild vasculitis at the disease onset.9) Mechanistically, this might be largely attributable to some sort of dysfunctional vascular healing manifesting either as an under-healing or over-healing (excessive vascular remodeling) process in these segments.9)
Vascular under-healing
Reactive inflammation and subsequent fibrotic response are well known to serve as fundamental repair mechanisms usually in a well-balanced manner following tissue injury.14) In the setting of KD, ‘mild coronary arteritis’ is usually characterized by a mild and transient segmental dilatation presenting with a diameter of ≤1.5 times that of the neighboring reference segment or an echocardiographic Z score of 2 to <2.5.1) This form of coronary arteritis is well known to be an early and fully reversible phenomenon encountered in a significant portion of KD cases (up to 50% of cases), and usually resolves within 4 to 8 weeks after disease onset without any acute complications potentially suggesting little or no long-term prognostic relevance.1) Pathologically, this phenomenon might be regarded as a milder form of generalized vascular inflammatory reaction (possibly without severe neutrophilic infiltration) also encountered in other febrile conditions, and might be attributable to certain factors including circulating cytokines.1) Timely initiation of antiinflammatory strategies might possibly prevent, mitigate or terminate mild coronary arteritis (though fully reversible even if left untreated) as analogous to the setting of ‘early CAAs’.
Interestingly, even though ‘mild coronary arteritis’ seems quite innocent at the relatively earlier stages of KD, it might have the potential to elicit long-term pathological consequences. Within this context, permanent functional abnormalities associated with residual vascular damage was previously demonstrated even in apparently normal epicardial coronary arteries (possibly with mild vasculitis) in patients with KD.15) Therefore, residual vascular damage followed by a vascular healing process might be expected to be even more pronounced in the setting of ‘mild coronary vasculitis’ with a transient dilatation. More importantly, vascular healing following ‘mild coronary arteritis’ might occur in a dysfunctional manner characterized by an under-healing process in certain susceptible subjects particularly in the presence of certain risk factors including prolonged and/or excessive steroid use (for refractory KD1)8) or other indications), diabetes mellitus (DM) and severe malnutrition with well-known adverse effects on extracellular matrix (ECM) components.9) This might ultimately lead to vascular frailty and late CAA formation in the long term.9) Conversely, DM was also suggested to have a protective role in the evolution of CAAs and abdominal aortic aneurysms mostly through a reduction in matrix metalloproteinase-2 (MMP-2) and MMP-9 levels leading to the mitigation of excessive vascular remodeling.16)17)18)19)20) Furthermore, significant impact of increased advanced glycation end products on vascular smooth muscle proliferation and ECM expansion might also be of crucial importance in this setting.16)17)18)19)20) However, pivotal impact of DM on the prevention of arterial aneurysms mostly emerge in the setting of atherosclerosis characterized by high inflammatory activity as demonstrated with excessive levels of MMPs and low levels of fibrocellular components.16) Therefore, DM might paradoxically lead to the evolution and progression of CAAs associated with vascular injury as a consequence of incomplete vascular healing. This might be exemplified by the evolution of ‘late CAAs’ in the setting of KD.9)
Systemic steroid use in KD has been mostly warranted in cases unresponsive to IVIG therapy,1)8) and was also demonstrated to decrease the incidence of early CAA formation even when initiated as part of initial management strategies in a previous meta-analysis.21) Conversely, steroid use was also suggested to be independently associated with the evolution of ‘early CAAs’ (also in the form of giant CAAs) in another study.22) These findings may suggest that steroids, as strong antiinflammatory agents, might prevent or mitigate early CAA formation when initiated during the early stages of KD characterized by high inflammatory activity. However, these agents might do more harm than good22) when initiated in the active healing phase of KD characterized by minimal or no inflammation potentially predisposing to the evolution of ‘early CAAs’. In a similar manner, prolonged and excessive steroid use in the healing phase of ‘mild coronary arteritis’ might also be associated with late CAA formation not only as a consequence of dysfunctional tissue healing but also due to steroid-induced hemodynamic changes including elevated blood pressure.
Vascular over-healing (excessive vascular remodeling)
Alternatively, dysfunctional vascular healing in the setting of ‘mild coronary arteritis’ might also manifest as an over-healing process primarily characterized by an excessive positive (outward) remodeling orchestrated by well-known fibrogenic substances including transforming growth factor-beta (TGF-β).9)11)23) On the other hand, tissue over-healing following injury was previously suggested to harbor a substantial genetic basis, and hence; individual variation largely attributable to various gene polymorphisms associated with proinflammatory mediators and/or growth factors.14) In particular, certain fibrogenic mediators including TGF-β (and associated SMAD3 signaling accounting for myofibroblast activation, fibrogenesis) and vascular endothelial growth factor were previously suggested to be significantly associated with classical early CAA formation in patients with KD.1)16) Pathogenetic roles of these mediators in genetically susceptible KD patients might be even more susbstantial in the genesis of ‘late CAAs’ due to the purely fibroproliferative nature of these aneurysms.9)
As an interesting speculation on the evolution of excessive vascular remodeling, certain viral triggers associated with KD evolution (possibly through autoinflammatory mechanisms) might have the potential to uncover vascular manifestations of genetically inherited connective tissue diseases with an incomplete genetic penetrance and mild phenotypical presentation. One such disease Marfan syndrome presents with abnormalities in fibrillin-1 (an essential ECM glycoprotein) potentially interfering its interaction with TGF-β binding protein with eventually diminished TGF-β sequestration and enhanced TGF-β signaling.24)25) However, it is well known that mild abnormalities in these specific proteins or mediators, due to incomplete genetic penetrance, might be relatively frequent generally leading to mild or no phenotypical presentation of the associated connective tisue disease (including normal aortic diameter and subtle musculo-skeletal abnormalities). Within this context, it seems quite possible that a ‘second hit‘ triggered by the viral agent (potentially associated with the evolution of index KD episode)1) might induce significant genetic mutations with consequent overexpression of subclinical connective tissue disease. This might elicit progressive coronary arterial remodeling particularly in the presence of ‘mild coronary arteritis’ ultimately leading to late CAA formation in the long-term. This virally induced mutations might also result in late-onset aneurysms in other vascular structures including aortic root. However, the above-mentioned notions are speculative, and should be tested with experimental and clinical studies.
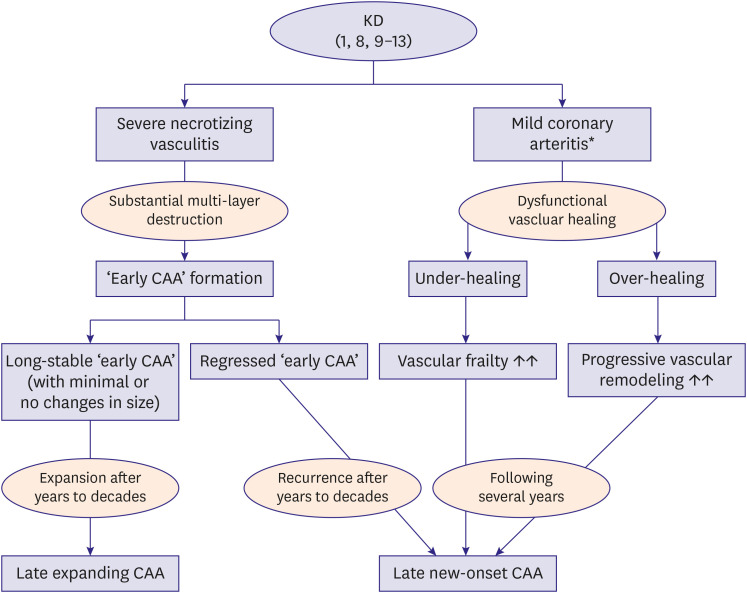
Taken together, it might be suggested that ‘dysfunctional vascular healing’ involving mildly affected coronary segments without necrotizing vasculitis might possibly serve as an alternative mechanism of late CAA formation in the setting of KD.9) Therefore, this mechanism might be suggested as a potential explanation to the evolution of ‘late CAAs’ in a portion of previous KD case series in whom late aneurysms emerged at coronary sites unaffected by previous ‘early CAAs’.10) It seems reasonable that dysfunctional vascular healing associated with late CAA formation might exclusively occur in a subset of KD patients with certain risk-factors. On the other hand, factors including failure to initiate certain specific antiinflammatory strategies (including IVIG) in a timely manner or being a non-responder to this strategies might also serve as potential risk factors for late CAA formation associated with dysfunctional vascular healing. Lastly, a significant portion of idiopathic coronary aneurysms (without a history of ‘early CAA’) detected incidentally on coronary imaging modalities might causally be attributable to this insidious phenomenon.9) Potential mechanisms of late CAA evolution are summarized in Figure 1.
Clinical outcomes and prognosis
Long-term or acute complications including LMP with coronary stenosis, thrombus formation within the aneurysmal sac with or without coronary ischemic syndromes, progressive aneurysmal dilatation and aneurysm rupture might be encountered during the course of classical ‘early CAAs’ mostly requiring urgent interventional or surgical management strategies.1)5)6)7)8) Of note, these complications mostly emerge in the setting of giant CAAs generally defined as aneurysms with a diameter of >4 times that of the reference segment or >8 mm or with a Z score of >10).1)5)6)7)8) It seems noteworthy that small-medium CAAs (<8 mm in diameter) that constitute the overwhelming majority of ‘early CAAs’ generally regress26) or remain morphologically stable with a trivial risk for late expansion. Therefore, giant ‘early CAAs’ (>8 mm) particularly warrants close follow-up, and in certain instances, prophylactic interventional strategies that all have been discussed in details in the recent guidelines on KD and other reports.1)5)6)7)8) On the other hand, since the body size significantly varies in children according to their age groups and constitutional factors, exclusive use of numerical threshold values (including aneurysm diameter) to define giant ‘early CAAs’ is generally discouraged.1) Therefore, other strategies including Z score and comparison with the reference coronary segment1)5)6)7)8) should also be incorporated into the evaluation particularly when decision-making for subsequent management strategies is of critical importance.
Conversely, ‘late CAAs’ have been mostly diagnosed incidentally on CAG performed as part of long-term KD surveillance strategies.10)11)12) Clinically, these aneurysms were previously reported to pursue a lenient course with no significant risk for coronary adverse events.10)11)12) In this context, it seems quite likely that aneurysm size also serves as the potential determinant of prognosis in the setting of ‘late CAAs’. In a large series of KD, no patients with ‘late CAAs’ incurred any adverse events on follow-up largely attributable to the small-medium size of these aneurysms (median 4.1 mm).10) Therefore, complications including thrombus formation, progressive aneurysmal dilatation, aneurysm rupture might be quite unusual in the setting of ‘late CAAs’. However, there might be exceptional cases of progressive aneurysmal dilatation in patients with ‘late CAAs’ as well.26) Accordingly, progressive expansion of a ‘late CAA’ involving RCA (from an initial diameter of 6 mm to a final diameter of 86 mm during a period of 17 years) was previously reported to be managed with aneurysmectomy and aorto-coronary bypass due to the imminent risk of rupture.26) Therefore, even though giant ‘late CAAs’ are rarely encountered compared with giant ‘early CAAs,’ they might potentially lead to complications as well.26) Moreover, as opposed to the general consensus on the definition of giant ‘early CAAs’ during childhood,1)27)28) there exists a significant variation in the definition of giant CAAs in adults.27)29)30) This diagnostic confusion might also apply to the setting of giant ‘late CAAs’ in the setting of KD. Aneurysm diameters of >20 mm and >50 mm were previously used to define giant CAAs in adults.27)29)30) However, these aneurysms were mostly congenital pathologies associated with fistulas draining into cardiac chambers, and were reported to present with severe symptoms mostly requring surgical correction.27)29)30) On the other hand, inherent characteristics of congenital coronary aneurysms (initial size, pattern of progression and definition of giant aneurysm, etc.) in adults appear to be quite different compared with those of ‘late CAAs’. Taken together, due to the lack of consensus on the threshold aneurysm diameter for the definition of giant CAAs, harnessing the criterion ‘an aneurysm diameter of >4 times that of the reference segment’ seems more reasonable as an initial and practical strategy. However, we strongly suggest that this strategy should also be substantiated with the calculation of ‘Z score’ particularly in patients with a borderline value (for instance; an aneurysm/reference segment diameter ratio of 3.7) or in those with a neighboring reference segment that is not amenable to comparison due to an existing diffuse ectasia or vasospasm. We also suggest that Z score should also be calculated unconditionally in the setting of critical decision-making for prophylactic radical operations including elective aneurysmectomy.
More importantly, associated coronary stenoses, on top of their pathogenetic implications, might also exert a substantial impact on the prognosis of ‘late CAAs’. In a previous KD series,10) variable degrees of coronary stenoses (ranging from 25% to 90%) were reported in all cases with ‘late new-onset CAAs’ either serving as a bystander phenomenon or a potential contributory factor in CAA evolution. In this context, ‘late CAAs’ mostly arise as post-stenotic pathologies along the coronary arteries.10) More importantly, a significant portion of cases with ‘ late CAAs’ might require coronary artery bypass grafting (CABG) or percutaneous coronary intervention (PCI) due to the severity of associated coronary stenoses.10) More rarely, coronary stenoses in the setting of ‘late new-onset CAAs’ might end up with coronary occlusion31) that might mandate urgent revascularisation strategies. Taken together, associated coronary stenoses, that are more likely encountered in patients with ‘late new-onset CAAs,’10)31) might serve as the fundamental risk-stratifier in these patients.
Interestingly, a portion of ‘late CAAs’ (particularly those arising in segments with mild coronary arteritis due to dysfunctional vascular healing) might also have a potential proclivity for specific coronary complications including spontaneous coronary artery dissection possibly as a result of ongoing pathological remodeling involving intima and media layers.9) In contrast, a multi-layer vascular destruction with extreme wall thinning possibly with higher degrees of dystrophic calcification32) might potentially preclude this challenging complication in the setting of early ‘CAAs’ or ‘late CAAs’ arising due to recurrence or late expansion of ‘early CAAs’.9) However, these notions should be tested using specific imaging modalities including intravascular ultrasound (IVUS), etc.
Management
In the acute setting of KD, timely initiation of conventional agents including IVIG and high dose acetyl salicylic acid (ASA) appears to be mandatory for the prevention or mitigation of life-threatening consequences including early CAA formation.1) Furthermore, certain bail-out regimens including steroids, etanercept (tumor necrosis factor-alpha [TNF-α] inhibitor), infliximab (monoclonal antibody against TNF-α), cyclosporine have been used in refractory cases unresponsive to IVIG (10–20% of KD population).1)33) Details of these antiinflammatory strategies may be found elsewhere,1)8) and are beyond the scope of this paper. More specifically, IL-1 and associated caspase-1 were experimentally demonstrated to have particular implications in the evolution of coronary damage and myocarditis in patients with KD.33)34)35) Therefore, IL-1 antagonism with the use of certain agents including anakinra (IL-1 β receptor antagonist) and canakinumab (IL-1 monoclonal antibody) has risen as a promising therapeutic option as a second-line or even first-line strategy in severe cases.33)34)35) Taken together, the above-mentioned antiinflammatory agents mostly target prevention or mitigation of ‘early CAAs’.33)34)35) Accordingly, only 13 out of 325 (4%) IVIG responders with KD were reported to develop ‘early CAAs’ at 4 weeks in a recent retrospective analysis.36) Importantly, a pretreatment Zmax value (the highest Z score in coronary branches) of >2.5 was suggested as the sole clinical variable to predict the evolution of ‘early CAAs’ with a specificity of 91% and a sensitivity of 50%.36) This might potentially warrant more aggressive antiinflammatory regimens in KD patients who already have a pattern of significant coronary dilatation at diagnosis.36) Interestingly, 4 out of 13 patients having CAAs at 4 weeks had a pretreatment Z max value of <2.0.36) Unfortunately, this might imply that KD patients, who have apparently unaffected coronary arteries at the time of diagnosis, might occasionally develop ‘early CAAs’ even after succesful IVIG therapy.36) It seems noteworthy that some authors raised the possibility of long-term use of certain agents including anakinra in an effort to prevent fibroproliferative complications including luminal stenosis.34) Therefore, IL-1 antagonism might also have a potential therapeutic benefit in the setting of established ‘late CAAs’ particularly with regard to prevention of further aneurysm progression.
In general, management strategies of established CAAs (whether early or late) largely depend on the aneurysm size, history of cardiovascular events and acute complications. In this context, certain strategies including life-style modification, statin use constitute preventive approaches against secondary atherogenesis associated with residual endothelial dysfunction.1)8) Moreover, β-blockers and antiplatelet (and/or anticoagulant) therapy might be indicated indefinitely to prevent coronary ischemic complications.1)8) Based on previous reports,9)37) certain agents including renin-angiotensin system (RAS) inhibitors including captopril might also be of significant clinical benefit due to their potential inhibitory impact on MMP-9 synthesis that might possibly contribute to aneurysm formation and progression. However, RAS inhibition seems to be particularly more efficient in a subgroup of KD patients possibly with a genetically-determined and excessive levels of culprit mediators including TGF-β, MMP-9.9)
Effective antiplatelet and/or anticoagulant strategies have been the mainstay of therapy in the setting early and late CAAs associated with KD.1)8)10)38) Type and intensity of blood-thinning regimens mostly depend on the aneurysm size.1)38) In particular, ASA starting from the initial stages usually in combination with systemic anticoagulation (warfarin or heparin) might be indicated particularly in patients with giant early and late CAAs.1)5)8)11)38) In relatively larger, yet; not giant aneurysms, dual antiplatelet therapy including ASA plus clopidogrel may be the preferred strategy.38) However, since ‘late CAAs’ appear to be relatively smaller9)10) possibly leading to less pronounced blood stasis and endothelial injury, it seems more proper to initiate and continue single antiplatelet therapy indefinitely for primary thromboprophylaxis. Potential consideration of adding a second antiplatelet agent in high-risk conditions including relatively larger aneurysms or history of coronary ischemic events might be necessary in the setting of ‘late CAAs’ (as currently recommended also in the setting of ‘early CAAs’).1) However, anticoagulant therapy was deemed as the first-line strategy in patients with ‘late CAAs’ with a median aneurysm size of 4.1 mm in a previous report.10) On the other hand, low dose anticoagulant therapy particularly with novel agents including rivaroxaban (2×2.5 mg) (largely due to its significant adjunctive benefit on top of ASA therapy in the setting of high-risk chronic vascular disease)39) together with an antiplatelet agent might also serve as a plausible alternative to dual antiplatelet regimens or routine anticoagulant therapy in high-risk situations. However, safety and efficacy of low dose anticoagulation with novel agents should be tested particularly in early38) and ‘late CAAs’ associated with KD . Since the size of CAAs might change dynamically in time, dose of antiplatelet/anticoagulant regimens need to be adjusted according to the aneurysm size on imaging modalities during follow-up.1)8)
Importantly, surgical or percutaneous management of CAAs might be necessary in a portion of cases with KD.1)37)40)41)42) In the setting of mechanical complications including CAA rupture, fistulisation, compression or concomitant cardiac conditions including severe valvulopathy, surgical resection might arise as a viable option.40) In the general context of CAAs, progressive dilatation, recurrent coronary ischemic events or persistently huge aneurysm size might also indicate PCI with covered stents or coil embolization as an alternative to surgery.1)40)42) However, it should be borne in mind that CAG might potentially underestimate CAA diameter largely due to thrombus formation in the aneurysmal sac potentially warranting further imaging modalities including IVUS and multi-slice computed tomography (CT) to determine subsequent strategies.1)38)40) Surgical options including aneurysmectomy, though mostly indicated in KD patients with challenging ‘early CAAs,’1)40)41)42) might also be necessary in the setting of ‘late CAAs’ with high risk features including progressive expansion.26) Since the incidence of associated coronary stenoses appears to be higher in patients with ‘late CAAs,’ PCI or CABG might be indicated in a substantial portion of these patients.10) However, management of associated coronary stenoses with PCI may be quite challenging due to their fibroproliferative and calcific nature potentially requiring further strategies including rotational atherectomy.38) Taken together, the size of CAAs, existing complications as well as concomitant cardiac conditions mostly determine the type and intensity of management strategies (medical alone vs. PCI vs. surgery) in the setting of CAAs associated with KD.40) In rare instances, cardiac transplantation may be necessary in KD patients with refractory myocardial failure and/or coronary pathologies that are not amenable to PCI or surgery.1)
Long-term surveillance
A strict surveillance has been highly recommended in the setting of classical ‘early CAAs,’ and may be found in the recent KD guidelines and other reports in details.1)7)8)38) As a basic rule, the larger CAAs at 6 weeks mandate more frequent follow-up.1)38) For instance, evaluation of giant ‘early CAAs’ is recommended at 3, 6, 9,12 months in the first year, and biannually thereafter.38) Regular evaluation of atherosclerotic risk factors along with coronary imaging modalities including echocardiogram, CT) and, where necessary, stress testing modalities, constitute the fundamental aspects of surveillance programme in patients with KD.1)7)8)
Similarly, long-term surveillance, possibly with a less frequent follow-up usually at the discretion of the treating clinician, might also be warranted for established ‘late CAAs’ potentially exhibiting a lower propensity for dynamic morphological changes in time as compared with the classical early counterpart. Importantly, KD patients without ‘early CAAs’ yet; with a significant risk for late CAA evolution (including those with higher levels of profibrotic mediators at baseline, long-term steroid users) should also be under close supervision in an effort to timely detect and manage emerging ‘late CAAs’.9)12)
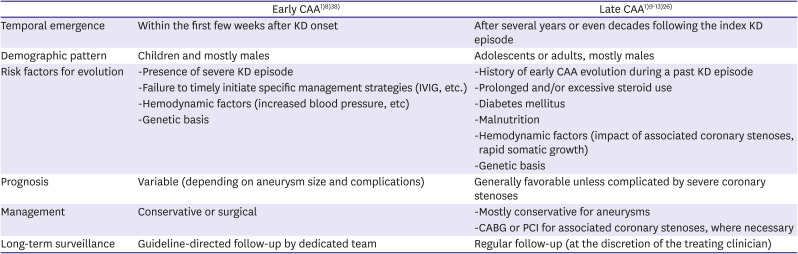
Table 1 summarizes a general comparison between early and late CAAs in the setting of KD.
Table 1
Summary of general comparison between early and late CAAs in patients with KD
| Early CAA1)8)38) | Late CAA1)9)10)11)12)13)26) | |
|---|---|---|
| Temporal emergence | Within the first few weeks after KD onset | After several years or even decades following the index KD episode |
| Demographic pattern | Children and mostly males | Adolescents or adults, mostly males |
| Risk factors for evolution | -Presence of severe KD episode | -History of early CAA evolution during a past KD episode |
| -Failure to timely initiate specific management strategies (IVIG, etc.) | -Prolonged and/or excessive steroid use | |
| -Hemodynamic factors (increased blood pressure, etc) | -Diabetes mellitus | |
| -Genetic basis | -Malnutrition | |
| -Hemodynamic factors (impact of associated coronary stenoses, rapid somatic growth) | ||
| -Genetic basis | ||
| Prognosis | Variable (depending on aneurysm size and complications) | Generally favorable unless complicated by severe coronary stenoses |
| Management | Conservative or surgical | -Mostly conservative for aneurysms |
| -CABG or PCI for associated coronary stenoses, where necessary | ||
| Long-term surveillance | Guideline-directed follow-up by dedicated team | Regular follow-up (at the discretion of the treating clinician) |
CONCLUSION
‘Late CAAs’ in the setting of KD have particular mechanistic and clinical aspects. Mechanistically, evolution of ‘late CAAs’ have been mostly associated with pre-existing ‘early CAAs’. In other terms, recurrence of completely (or partially) regressed ‘early CAAs’ or late expansion of these aneurysms might possibly account for late CAA evolution in patients with KD largely due to the impact of certain hemodynamic and pathological factors. Interestingly, dysfunctional vascular healing following ‘mild coronary arteritis’ (in the absence of necrotizing vasculitis and ‘early CAAs’) might also serve as an obsure mechanism of late CAA evolution particularly in the presence of certain risk factors.
Importantly, antiinflammatory agents including IVIG might also have important therapeutic implications in the setting of late CAA formation. In this context, timely initiation of these agents might not only have a pivotal role in the prevention of ‘early CAAs’ (that potentially recur as ‘late CAAs’ in the long term), but might also lead to the mitigation of ‘mild coronary arteritis’ at its earlier stages. Conversely, steroids, when used in an excessive and prolonged manner, might elicit dysfunctional vascular healing with consequent evolution and progression of ‘late CAAs’ in coronary segments with ‘mild coronary arteritis’. On the other hand, medical management of established ‘late CAAs,’ as analogous to the classical early counterpart, primarily constitute antiplatelet and /or anticoagulant regimens along with certain antiatherogenic agents including statins. Furthermore, RAS inhibition and posssibly IL-1 antagonism might potentially prevent further aneurysm expansion largely through mitigation or inhibition of excessive vascular remodeling in this particular context. However, favorable impact of these strategies on aneurysm progression currently remains at a speculative level, and needs to be confirmed in the clinical setting.
In the general context of CAAs, aneurysm size and potential complications serve as the primary determinants of overall prognosis. Accordingly, elective or urgent interventions might be necessary in certain clinical scenarios (progressive CAA expansion, existing giant CAAs and mechanical complications including fistula formation, etc.). However, clinical outcomes and prognosis of ‘late CAAs’ have been mostly favorable with exceptional cases of rapid expansion or severe coronary stenoses requiring urgent surgery. Of note, relatively high incidence of associated coronary stenoses might arise as a significant therapeutic challenge in the setting of ‘late CAAs’. However, further studies are strictly warranted to establish absolute mechanisms, clinical implications and management strategies of ‘late CAAs’ in patients with KD.
 XML Download
XML Download