This article has been
cited by other articles in ScienceCentral.
A baby was born through emergency C-sec delivery at 28
+3 weeks of gestation, with a birth weight of 1.3 kg, due to fetal ventricular tachycardia, severe ventricular dysfunction, and fetal hydrops (
Figure 1,
Supplementary Videos 1 and
2).
1) Electrocardiogram and Holter monitoring showed intermittent 2:1 atrioventricular blocks (AVB) and prolonged QT interval with a circulatory collapse during bradycardia (
Figure 2). Inotropes including isoproterenol were started, but bradycardia episodes persisted despite decrease in frequency. After a week of unstable clinical conditions, ventricular functions began to improve and the patient began to tolerate bradycardia episodes due to 2:1 AVB. At a month of age, a non-sustained polymorphic ventricular tachycardia (Torsades de Pointes; TdP) developed, 2–3 times a day (
Figure 3). A beta-blocker was applied without an effect, then oral mexiletine was added, resulting in a gradual decrease of QT interval and the AVB episodes, and eventually TdP disappeared (
Figure 4). The patient was discharged home at 87 days after birth, taking propranolol and mexiletine. Currently, the patient is 16 months old and in normal growth without any cardiovascular event. The last electrocardiogram showed 1:1 AV conduction with much decreased QTc (470 ms) (
Figures 4 and
5). Next-generation sequencing revealed a
KCNH2 gene mutation and long QT syndrome (LQTS) type 2 was confirmed.
Ventricular arrhythmia and/or 2:1 AVB associated with LQTS may cause fetal hydrops and intrauterine fetal demise, have been reported to have high mortality rate during infancy, and frequently need device therapy.
2)3) Mexiletine may be a good alternative choice for these patients.
4)5)
The Institutional Review Board of Seoul St. Mary's Hospital approved this study and the informed consent was waived (IRB number: KC21ZISI0437).
Figure 1
Fetal echocardiography images. (A) A transverse scanning with a four-chamber view shows enlarged right atrium, dilated and hypertrophied right ventricle, small amount of pericardial effusion (open arrow), and pleural effusion (closed arrow). (B) An M-mode image shows a ventricular tachycardia (red dots) with a heart rate of 215 beats/min, instead atrial rate (yellow dots) is 120 beats/min. (C) Tricuspid valve inflow Doppler shows a sharp monophasic filling pattern. (D) A ductus venosus flow Doppler shows reverse flows during atrial contractions (arrows). (E) An umbilical venous flow Doppler shows notches during atrial contractions (arrow heads). All of the above findings suggest severe fetal cardiovascular dysfunction and poor general conditions, which demand immediate treatment.1) Image C, D and E were obtained during the time without ventricular tachycardia.
LA = left atrium; LL = left lung; LV = left ventricle; RA = right atrium; RL = right lung; RV = right ventricle.
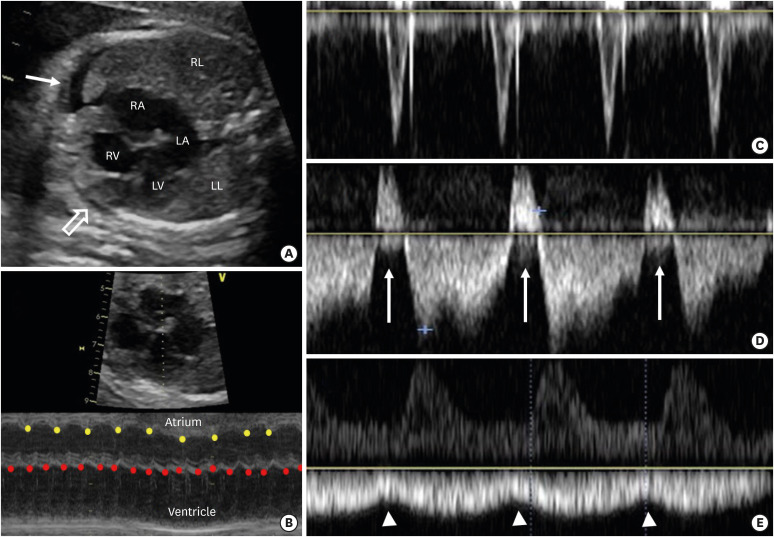
Figure 2
Electrocardiograms after birth showing a sinus rhythm with a heart rate of 166 beats/min and prolonged QT interval (QTc = 530 ms) (A) and frequent 2:1 atrioventricular blocks with a heart rate of 50–60 beats/min (B). Severe sudden heart rate fluctuations (50–130 beats/min) were observed on Holter monitoring (C).
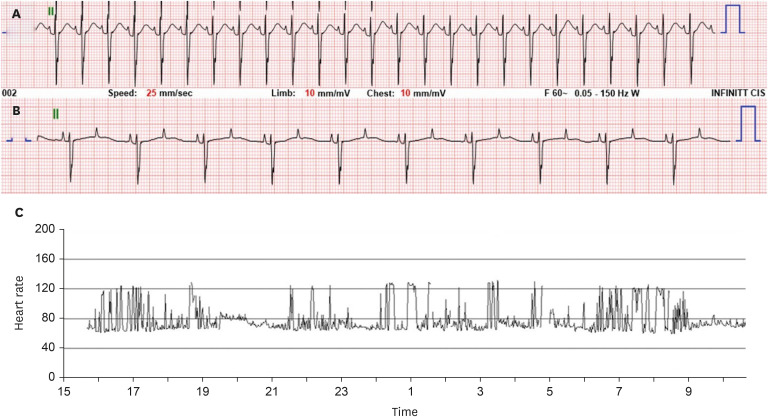
Figure 3
Electrocardiogram at 1 month of age, showing a polymorphic ventricular tachycardia (Torsades de pointes), which occurred 2–3 times a day.
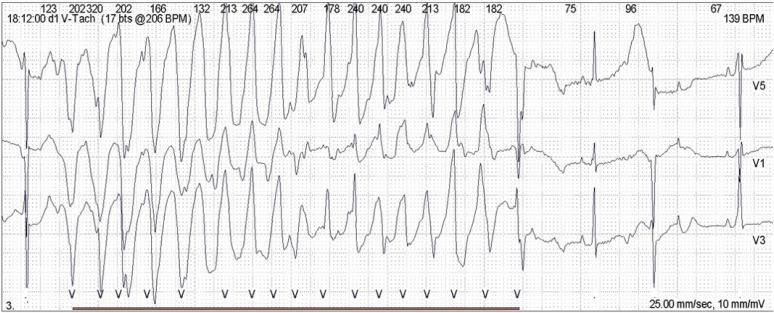
Figure 4
Serial changes of electrocardiogram (lead II and V5) and corrected QT intervals (QTc) over time according to the age of the patient. Electrocardiograms at 1 and 3 months of age showed 2:1 atrioventricular blocks and thereafter, normal sinus rhythms.
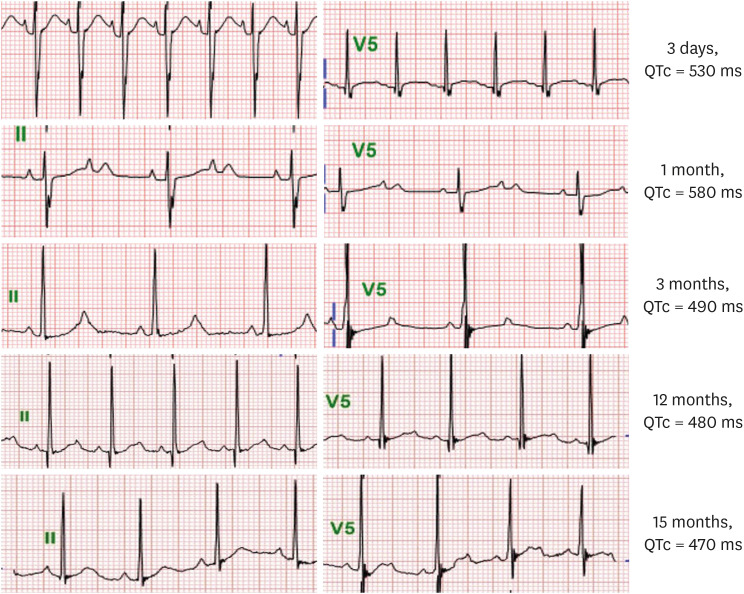
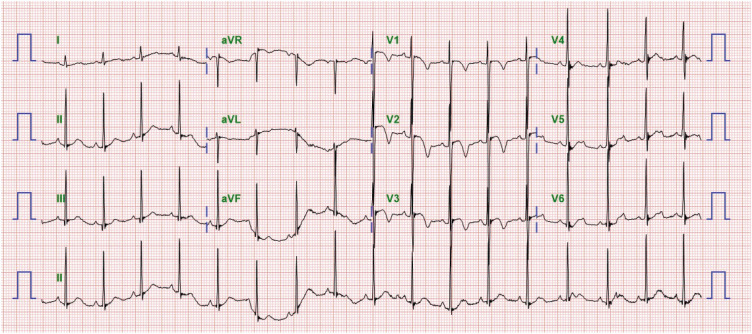
Figure 5
Electrocardiogram at 15 months of age showing a sinus rhythm with a QTc of 470 ms, and notched and asymmetrical T-waves, which are rather typical T-wave morphology in LQT2.


 PDF
PDF Citation
Citation Print
Print




 XML Download
XML Download