

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Hypertension (HTN) is a well-known, powerful risk factor of cardiovascular disease (CVD), and its prevalence has been rising worldwide.1)2)3) Previous clinical trials have shown that treating HTN reduced the risk of all-cause mortality and CVD, including stroke, myocardial infarction, and heart failure.4)5)6)7) More importantly, the Systolic Blood Pressure Intervention Trial (SPRINT) demonstrated that intensive blood pressure (BP) control (targeting a systolic BP of less than 120 mmHg), compared with standard control (targeting a systolic BP of less than 140 mmHg), reduced rates of major adverse cardiovascular events in patients at high risk for CVD without diabetes mellitus.8) Based on that result, the current relevant guidelines recommend treatment thresholds for the initiation of antihypertensive drugs and target BP ranges that are lower than those in the previous guidelines as long as patients tolerate the treatment.9)10)11) Nevertheless, in real-world practice, BP control rates are still low, and the prevalence of resistant HTN continues to increase globally.12)13) One of the factors affecting that result is poor adherence to prescribed antihypertensive medications. In fact, previous large observational studies have shown that roughly half of participants stop taking their antihypertensive drugs within a year for various reasons, including poor patient compliance, adverse effects of drug therapy, and socioeconomic factors,14)15) and non-persistence or low adherence to antihypertensive treatment was associated with future adverse outcomes.16)17)18)19) In this regard, patients who cannot take medication or poorly adhere to their prescribed regimen might need additional or alternative treatment options for adequate BP control, and device-based BP-lowering therapy such as renal denervation (RDN) could be a complementary or alternative treatment option for those patients.20)21)22) In this review, we discuss the current evidence, issues, future trials, and potential roles of RDN as an attractive treatment option for HTN.
Go to : 
PATHOPHYSIOLOGICAL RATIONALE
Although the pathophysiology of HTN is complicated, the renal sympathetic nervous system, which contains both afferent and efferent sympathetic nerve fibers, plays an essential role in the development of HTN.23) Concretely, activation of the efferent sympathetic nerves in the renal artery can lead to renal arteriolar vasoconstriction, decreased renal blood flow, increased renin secretion, subsequent activation of the angiotensin-aldosterone system, and increased sodium and water absorption, resulting in increased intravascular volume and the maintenance of systemic HTN.24) On the other hand, activation of renal afferent nerves can lead to increased systemic sympathetic activity and hormone release in the hypothalamus, resulting in increased systemic vascular resistance and HTN.25) Therefore, RDN, which interrupts both efferent and afferent sympathetic sensory nerve pathways in the renal artery, has been developed for the treatment of HTN.
Go to :
EVIDENCE FOR THE FIRST-GENERATION DEVICE
The first-generation radiofrequency (RF) ablation system for performing RDN was a single unipolar electrode on a flexible (4 French) catheter (SYMPLICITY Flex™; Medtronic, Minneapolis, MN, USA). In 2009, Krum et al.26) conducted a proof-of-concept study (SYMPLICITY HTN-1) and demonstrated the feasibility of RDN in patients with resistant HTN. In that study, office BP was decreased by up to 27 mmHg (systolic BP) and 17 mmHg (diastolic BP) 12 months after the RDN procedure without serious procedure-related adverse events. Subsequently, the open-label randomized controlled SYMPLICITY HTN-2 trial also showed that the RDN group was associated with significant BP reduction at the 6-month follow-up, compared with control group (RDN vs. control group, −32/12 mmHg vs. 1/0 mmHg, p<0.001) in patients with treatment-resistant essential HTN (defined as office systolic BP ≥160 mmHg despite the prescription of ≥3 antihypertensive drugs).27) Most observational studies and registries showed similarly promising findings.28)29)30)
In 2014, to overcome the methodologic shortcomings, particularly the lack of blinding, in the SYMPLCITY HTN-2 trial, an additional multicenter, single-blind, randomized sham-controlled trial (the SYMPLICITY HTN-3 trial) was conducted in patients with resistant HTN (defined as office systolic BP ≥160 mmHg despite the prescription of ≥3 antihypertensive drugs).31) In that study, 535 patients with resistant HTN were randomly assigned in a 2:1 ratio to undergo RDN or a sham procedure. Unexpectedly, the early excitement about RDN ended abruptly when the results of the SYMPLICITY HTN-3 trial failed to demonstrate the superiority of RDN over sham treatment for office BP changes at 6 months. In the SYMPLICITY HTN-3 trial, the mean change in office systolic BP at 6 months was −14.13 ± 23.93 mmHg in the RDN group (p<0.001 for comparisons with baseline) and −11.74 ± 25.94 mmHg in the sham-procedure group (p<0.001 for comparisons with baseline), without a significant between-group difference (difference of −2.39 mmHg; 95% confidence interval [CI], −6.89 to 2.12 mmHg; p for superiority=0.26 with a margin of 5 mmHg), although the safety endpoints did not differ significantly between the two groups either.31) Several possible explanations have been proposed to account for the discrepancy between the results of the SYMPLICITY HTN-3 trial and the results of previous studies and registries, including the SYMPLICITY HTN-1 and -2 trials. First, 39% of patients underwent antihypertensive medication changes during the study period. Furthermore, trial participation might have affected the high degree of adherence to antihypertensive therapy found among the participants because of close follow-up, which might be associated with the unexpectedly large BP reduction in the sham group. Second, patients with isolated systolic HTN were included in the SYMPLICITY HTN-3 trial. Mahfoud et al. reported that changes in isolated systolic HTN following RDN was less pronounced than BP reduction in patients with combined systolic and diastolic HTN.32) Third, due to the limitations of operator experience with RDN, only a few patients in the RDN group received the complete circumferential ablation pattern in the main renal arteries recommended in the protocol. Actually, the number of ablations was associated with the degree of BP reduction in post-hoc analysis of SYMPLICITY HTN-3 trial data.33)
Beyond the SYMPLCITY HTN-1, -2, and -3 trials, several other randomized controlled trials and registries have been published about the first-generation RDN device, and Table 1 summarizes the results of those studies.34)35)36)37)38)39)40)41)42)43) Among them, the issue of adherence, which is one of the weaknesses of the SYMPLICITY HTN-3 trial, was adequately addressed in the well-designed open-label randomized controlled Renal Denervation for Hypertension (DENERHTN) trial. That trial included 106 patients with well-defined and truly resistant HTN, and the patients were randomized 1:1 to receive either RDN plus standardized stepped-care antihypertensive treatment (SSAHT) or SSAHT alone. That study showed that RDN plus SSAHT reduced ambulatory systolic BP significantly better than SSAHT alone (RDN vs. control, −15.8 mmHg vs. −9.9 mmHg; baseline-adjusted difference of −5.9 mmHg; 95% CI, −11.3 to –0.5 mmHg; p=0.033). Of note, although about 50% of the patients in both the RDN and control groups were partially or completely non-adherent to antihypertensive medications, no differences in doses or adherence rates were found between the two randomized groups.44) Interestingly, a post-hoc analysis of the DENERHTN trial demonstrated that antihypertensive medication nonadherence was a major determinant of the difference between office systolic and daytime ambulatory BP.45)
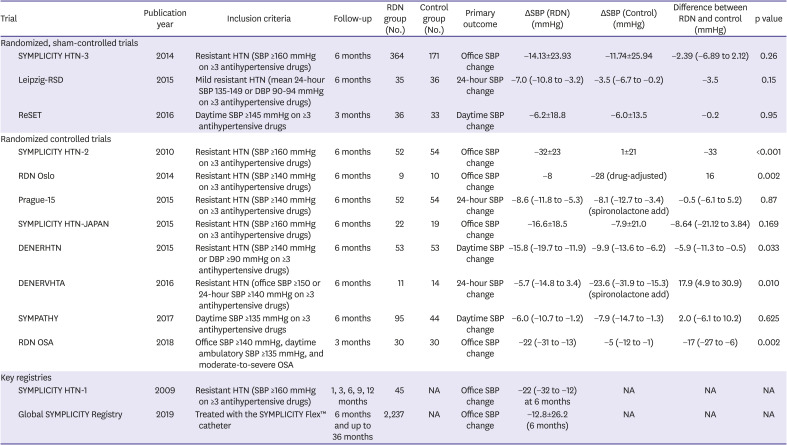
Table 1
Results from trials that used the first-generation RDN device (SYMPLICITY Flex™)
Data are presented as the mean±standard deviation or median (95% confidence interval).
DBP = diastolic blood pressure; HTN = hypertension; NA = not applicable; OSA = obstructive sleep apnea; RDN = renal denervation; SBP = systolic blood pressure.
![]()
Go to :
SECOND-GENERATION RENAL DENERVATION TRIALS
Radiofrequency ablation-based treatment
Because the results of trials using a first-generation RDN device for the treatment of HTN were controversial, several subsequent preclinical and clinical studies explored ways to improve the effectiveness of RDN.46)47)48) For example, a second-generation RF ablation device (SYMPLICITY Spyral™; Medtronic), a flexible 4-electrode catheter design used to perform 4 simultaneous ablations with a helical pattern, was developed. This system can perform a comprehensive RDN procedure that includes ablation in the distal main renal artery and arterial branches. Based on the lessons learned from the pitfalls of the SYMPLICITY HTN-3 study, two well-designed, randomized, sham-controlled, pilot trials of the second-generation multielectrode SPYRAL RF ablation device were conducted.49)50) Those trials enrolled patients with mild to moderate combined systolic and diastolic HTN (defined as office systolic BP ≥150 mmHg and <180 mmHg, office diastolic BP ≥90 mmHg, and mean 24-hour ambulatory systolic BP ≥140 mmHg and <170 mmHg) in the absence (SPYRAL HTN-OFF MED trial) or presence (SPYRAL HTN-ON MED trial) of antihypertensive medication. Based on the previous results of a randomized trial comparing the effectiveness of BP reduction between RF ablation at distal renal arterial branches beyond the main renal artery vs. conventional main renal artery treatment,51) all previously experienced RDN operators who participated in these studies were advised to perform RF ablation at all accessible renal arteries, including distal segments and subsequent branches, using a multi-electrode catheter. Furthermore, medication adherence was strictly evaluated by urine or serum assays both before and after the RDN or sham treatment in the SPYRAL HTN-ON MED study to identify the effect that adherence had on the endpoints. In the prospectively planned interim analyses of the first 80 patients enrolled in the SPYRAL HTN-OFF MED study, the RDN group showed a significant reduction in mean 24-hour ambulatory systolic BP from baseline to 3 months (−5.5 mmHg; 95% CI, −9.1 to −2.0 mmHg; p=0.003), but the sham procedure group saw no significant difference (−0.5 mmHg; 95% CI, −3.9 to 2.9 mmHg; p=0.76; difference between groups −5.0 mmHg; 95% CI, −9.9 to −0.2 mmHg; p=0.041). The SPYRAL HTN-ON MED trial of patients taking one to three antihypertensive medications also demonstrated that 24-hour ambulatory systolic BP decreased significantly from baseline to 6 months in the RDN group (−9.0 mmHg; 95% CI, −12.7 to −5.3 mmHg; p<0.001) but not in the sham procedure group (−1.6 mmHg; 95% CI, −5.2 to 2.0 mmHg; p=0.365), with significant between-group differences (−7.4 mmHg; 95% CI, −12.5 to −2.3 mmHg; p=0.005). Interestingly, similar to the DENERHTN trial, the patient adherence rate to the prescribed antihypertensive medications was about 60% and did not differ significantly between the RDN and control groups at 3 or 6 months. Recently, the sham-controlled SPYRAL HTN-OFF MED Pivotal trial was published and was adequately powered for the primary efficacy endpoint.52) A total of 331 patients was recruited using a combination of data from pilot (n=80) and pivotal (n=251) trials. A Bayesian approach was used for the primary analyses. The treatment difference between the RDN and sham control groups for 24-hour systolic BP was −4.0 mm Hg (Bayesian 95% credible interval, −6.2 to −1.8 mmHg; p=0.001), and for office systolic BP, the difference was −6.6 mm Hg (Bayesian 95% credible interval, −9.6 to −3.5 mmHg; p<0.001). There was no difference in major device-related or procedural-related safety events between the two groups for up to 3 months. The prospectively powered sham-controlled SPYRAL HTN-ON MED Expansion trial is currently ongoing (ClinicalTrials.gov, NCT02439775). The results of these trials are expected to consolidate support for RDN as a treatment for HTN. Beyond the SYMPLICITY Flex™ and Spyral™ ablation catheters, other RF ablation systems have been developed and approved for use in Europe (EnligHTN [St. Jude Medical, St. Paul, MN, USA], Vessix [Boston Scientific, Marlborough, Massachusetts, USA], OneShot [Covidien, Dublin, OH, USA], and Iberis [Terumo, Ann Arbor, MI, USA]), China (GL-06E15WA ablator and GL-6W ablation catheter [Shanghai Golden Leaf Medtech Company, Shanghai, China]), and Korea (DENEX™ [Handok Kalos Medical, Seoul, Korea]).53)54)55)56)57)58) However, those devices still need their efficacy and safety proven in well-designed, randomized, sham-controlled trials. Among them, the recent randomized, sham-controlled Renal Denervation Using the Vessix Renal Denervation System for the Treatment of Hypertension (REDUCE HTN REINFORCE) trial evaluated the efficacy of balloon-type bipolar RF-based RDN devices (Vessix; Boston Scientific).59) Although enrollment was terminated early for apparent futility before a sample sufficient for powered efficacy comparisons was enrolled, a significant difference in office systolic BP reduction in favor of RDN was reported at 6 and 12 months.
Ultrasound-based treatment
An alternative technology using balloon-type ultrasonic RDN catheters (ReCor Medical, Palo Alto, CA, USA) allows complete circumferential denervation in a more reliable fashion than RF ablation by generating frictional heating through the interaction of high-frequency sound waves that pass through the surrounding fluids.60) The multicenter, randomized, sham-controlled RADIANCE-HTN SOLO (patients with mild to moderate HTN without antihypertensive medications) and TRIO (patients with uncontrolled HTN receiving 3 antihypertensive medications) trials were conducted to evaluate the safety and efficacy of the ultrasound-based RDN procedure. In the RADIANCE HTN Solo trial, 146 patients with combined systolic and diastolic HTN (daytime ambulatory BP ≥135/85 mmHg and <170/105 mmHg) after discontinuing a maximum of two antihypertensive medications for 4 weeks before the ambulatory BP assessment were recruited.61) After 2 months, the reduction in daytime ambulatory systolic BP was significantly greater with RDN (−5.9±9.3 mmHg) than with the sham procedure (−2.2±10.0 mmHg, baseline-adjusted difference between groups: −6.3 mm Hg; 95% CI, −9.4 to −3.1; p<0·001). Between 2 and 6 months after randomization, patients in both groups were restarted on antihypertensive drugs according to a standardized drug titration protocol if their average home BP was ≥135/85 mmHg. At 6 months, greater reduction in daytime ambulatory systolic BP was maintained in the RDN group than in the sham control group (difference adjusted for baseline BP and number of medications −4.3 mmHg; 95% CI, −7.9 to −0.6 mmHg; p=0.024), despite being prescribed fewer antihypertensive medications than in the sham group (RDN vs. sham procedure, 65.2% vs. 84.5%; p=0.008).62) Between 6 and 12 months (unblinded phase), patients received antihypertensive medications at their physicians' preference. The decrease in daytime ambulatory systolic BP from baseline to 12 months in the RDN group was stably maintained, despite taking fewer prescribed medications than the sham procedure group (number of medications for RDN vs. sham, 1.0 vs. 1.4; p=0.015). However, the mean between-group difference in daytime ambulatory systolic BP change adjusted for the number of antihypertensive medications was not significant at 12 months (−2.3 mmHg; 95% CI, −5.9 to 1.3; p=0.201).63) In the recently published RADIANCE HTN TRIO trial, 136 patients with resistant HTN (defined as office BP ≥140/90 mmHg despite the prescription of ≥3 antihypertensive drugs, and daytime ambulatory BP ≥ 135/85 mmHg 4 weeks after switching a single-pill, fixed-dose, daily combination of amlodipine 10 mg, valsartan 160 mg [or Olmesartan 40 mg], and hydrochlorothiazide 25 mg) were finally enrolled.64) Full adherence to the combination medications at 2 months were similar between the two groups (RDN vs. sham, 82% vs. 82%; p=0.99). After 2 months, RDN procedure significantly reduced daytime ambulatory systolic BP more than the sham procedure (RDN vs. sham, −8.0 mmHg [interquartile range from −16.4 to 0.0 mmHg], vs. −3.0 mmHg [interquartile range from −10.3 to 1.8 mmHg]; group difference −4.5 mmHg; 95% CI, −8.5 to −0.3; adjusted p=0.022) without serious procedure-related adverse events. The currently ongoing REQUIRE (Korea and Japan, ClinicalTrials.gov, NCT02918305) trials will be helpful in determining the safety and efficacy of ultrasound-based RDN procedures for Asian patients with drug-resistant HTN taking standard antihypertensive medicines.
Ethanol injection-based treatment
The Peregrine catheter (Ablative Solutions, San Jose, CA, USA) was developed to deliver ethanol directly into the adventitial and periadventitial tissue of renal arteries. The preclinical study in a porcine model identified a linear dose-response between the injected alcohol volume and norepinephrine reduction in the renal artery.65) A prospective, multi-center, open-label trial showed that 6 months after performing the Peregrine catheter procedure, the mean 24-hour ambulatory BP was significantly reduced compared with baseline.66) This device is currently under investigation in a randomized, sham-controlled trial in hypertensive patients taking (TARGET BP I, ClinicalTrials.gov, NCT02910414) and not taking (TARGET BP OFF-MED, ClinicalTrials.gov, NCT03503773) antihypertensive medications.
Go to :
COMPARISON BETWEEN RADIOFREQUENCY ABLATION AND ULTRASOUND BASED RENAL DENERVATION
A recent randomized, single-blind trial was conducted to compare the BP lowering effects of three treatment arms: ultrasound-based (PARADISE catheter) and RF ablation-based (SYMPLICITY Spyral™ catheter) RDN of the main renal artery, and RF ablation-based RDN of the main renal arteries, side branches, and accessories in patients with resistant HTN (office systolic BP >160 mm Hg or diastolic BP >90 mm Hg diastolic despite treatment with ≥3 different classes of antihypertensive drugs, including at least 1 diuretic unless intolerant to diuretics).67) Although daytime ambulatory systolic BP was reduced more in the ultrasound-based treatment group at 3 months than in the group with RF ablation of the main renal artery (−13.2±13.7 vs. −6.5±10.3 mmHg; mean difference, −6.7 mmHg; p=0.038), no significant difference in systolic BP change was observed between the ultrasound-based treatment group and the group with main renal artery and side branch ablation (−8.3±11.7 mmHg for additional side branch ablation; mean difference −1.8 mmHg; adjusted p>0.99). This result might be because ultrasound energy has deeper penetration and offers more complete renal nerve ablation of the main renal artery than the RF ablation of the main renal artery alone. Nevertheless, this result should be interpreted with caution due to the limitations of this study, including the lack of a sham-control, lack of information about drug adherence tracking, and small sample size.
Go to :
SAFETY OF RENAL DENERVATION
In contrast to antihypertensive medications, the safety of device-based therapies for HTN focuses on procedural complications. Renal artery injury, vascular access site complications, and deterioration in kidney function were the most anticipated complications after the RDN procedure. However, the safety profile of RDN in several registries and clinical trials appears to be excellent. A recent meta-analysis of 50 published RDN trials reported on procedural safety.68) Among 5,769 subjects with 10,249 patient-years of follow-up, only 26 patients were found to have renal artery stenosis or dissection (0.45%). The 3-year safety data from the largest database, the prospective, open-label Global SYMPLICITY registry, also demonstrated an extremely low incidence of peri-procedural complications and adverse events.43)
Go to :
ETHNIC DIFFERENCES FOR ASIANS
It is well-known that there are significant ethnic differences in the determinants of HTN and the risk of HTN-related CVD.69)70)71) In general, the prevalence of HTN in Asia is similar to that in other countries, despite a lower prevalence of metabolic syndrome. In addition, the association between BP and CVD, especially for hemorrhagic stroke and non-ischemic heart failure, is stronger in Asian patients than in white patients.71)72)73) Masked HTN (defined as normal office BP and elevated out-of-office BP), which is associated with increased sympathetic activity, is more prevalent in Asians than in Westerners.74)75)76) East Asian populations in particular have at least a 2-fold higher sensitivity to the β-blocking effects of propranolol than white populations.77) Taken together, these ethnic differences indicate that Asian populations might be particularly sensitive to sympathetic modulation, thereby making the RDN procedure an attractive BP-lowering strategy for Asian patients.78)
The SYMPLICITY HTN-Japan randomized trial using the first-generation RDN device (SYMPLICITY Flex™; Medtronic) was the first published information specifically about the efficacy of RDN in an Asian population with resistant HTN.38) Although this trial did not provide conclusive information about the effects of RDN due to its small sample size and early discontinuation, the magnitude of office systolic BP reduction 6 months after the RDN procedure (−16.6±18.5 mmHg) was numerically greater than that in the SYMPLICITY HTN-3 trial (−14.13±23.93 mm Hg), in which the study population was mainly white and Black people. In Korea, the first successful percutaneous RDN using the first-generation device was used to treat a hypertensive patient with congestive heart failure in 2013.79) After that, a sub-analysis of the Global SYMPLICITY Registry evaluated the outcomes of the RDN procedure among patients from Korea.80) Compared with Caucasians with uncontrolled HTN, the Korean patients were younger, had a lower body mass index, a lower baseline systolic BP, and a higher prevalence of CVD, such as stroke, myocardial infarction, or angina. After propensity score matching, the Koreans had a systolic BP change similar to that of Caucasians at 6 months (−19.4±17.2 mmHg vs. −20.9±21.4 mmHg; adjusted p=0.998), whereas the change in BP reduction was significantly higher in Koreans than in Caucasians (−27.2±18.1 mmHg vs. −20.1±23.9 mmHg; adjusted p=0.002) at 12 months. The RDN procedural characteristics did not differ significantly between the two ethnic groups. Thus, the responsiveness of Asian patients to the RDN procedure appears to be at least equivalent to that of Westerners for the reduction of BP. Nevertheless, more evidence using the current generation of RDN devices is needed to confirm these findings.
Go to :
FUTURE DIRECTIONS OF RENAL DENERVATION BEYOND HYPERTENSION
The randomized, sham-controlled trial results for multipolar RF- and ultrasound-based second-generation RDN devices are summarized in Figure 1. Although these trials and several meta-analyses have shown that RDN was associated with reduced BP without serious complications, several problems with those results, including small sample sizes, highly selected patients, and short-term follow-up results, still limit its application in clinical practice.81)82)83) Thus, future trials should include large samples, less-selected patients, and longer follow-up times. Furthermore, clinical outcomes should be assessed following the RDN procedure to identify the benefits of RDN as a potential game-changer.
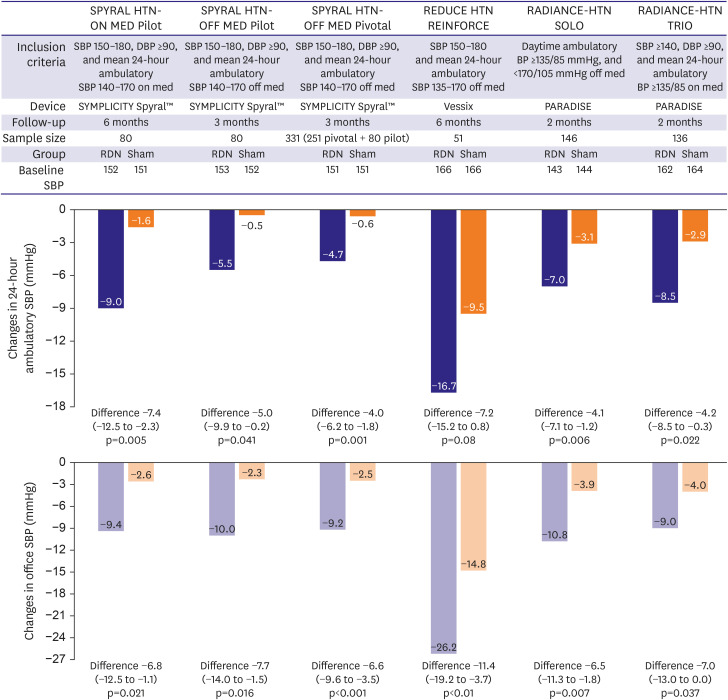 | Figure 1BP Changes with second-generation RDN devices in recently published randomized, sham-controlled trials.Changes in 24-hour ambulatory systolic BP and office SBP in the landmark randomized, sham-controlled trials using second-generation RDN devices are presented.
BP = blood pressure; DBP = diastolic blood pressure; RDN = renal denervation; SBP = systolic blood pressure.
|
Heart failure
Theoretically, excessive and prolonged activation of the sympathetic nervous system plays a key role in the pathological remodeling of the cardiac structure in patients with heart failure,84) and the use of a beta-blocker or renin-angiotensin system blockade, which affects the regulation of the sympathetic signaling pathway, has been associated with a reduced risk of morbidity in heart failure patients with reduced ejection fraction.85)86)87)88)89)90) Furthermore, Brandt et al.91) previously documented that RDN significantly reduced the left ventricular mass index, improved diastolic function, reduced interventricular septum thickness, decreased end-systolic volume, and improved ejection fraction. Therefore, the REACH-Pilot study was conducted to evaluate the efficacy and safety of the RDN procedure for patients with chronic systolic heart failure. Patients showed improvements in both symptoms and exercise capacity without peri-procedural complications 6 months after the RDN.92) However, the Renal Denervation in Heart Failure with Preserved Ejection Fraction (RDT-PEF) trial was terminated early because of difficulties in recruitment, leaving it underpowered to detect whether RDN improved the endpoints of quality of life, exercise function, biomarkers, and left heart remodeling in patients with heart failure with preserved ejection fraction.93) Therefore, future randomized, adequately powered, blinded, sham-controlled clinical trials are required to determine the effects of RDN on the morbidity of heart failure patients with reduced or preserved ejection fraction.
Atrial fibrillation
Sympathetic activation, particularly in association with para-sympathetic withdrawal, produces arrhythmias such as atrial fibrillation (AF).94) A randomized trial to evaluate the adjunctive effects of RDN on pulmonary vein isolation (PVI) for the treatment of refractory AF and drug-resistant HTN demonstrated that RDN reduces systolic and diastolic BP in patients with drug-resistant HTN and reduces AF recurrence.95) In addition, the larger Evaluate Renal Artery Denervation In Addition To Eliminate Atrial Fibrillation (ERADICATE-AF) trial also showed that adding RDN to PVI, compared with PVI alone, significantly increased the likelihood of freedom from AF 12 months later among patients with paroxysmal AF and HTN.96) These results suggest that RDN could be an attractive new treatment addition to PVI for patients with AF.
Chronic kidney disease
Patients with chronic kidney disease (CKD) are often refractory to drug treatment, even with the combination of several antihypertensive medications.97) Therefore, RDN might be a potentially beneficial intervention to treat the sympathetic activation associated with both HTN and CKD. However, most previous randomized trials of RDN have excluded patients with advanced CKD or end-stage renal disease due to concerns about renal safety. Observational studies have consistently shown that RDN was associated with significant BP-lowering effects without deteriorating the glomerular filtration rates of patients with CKD98)99)100) or end-stage renal disease.101) Future well-designed randomized outcomes studies in patients with CKD treated with and without RDN would provide interesting evidence about risk reduction in those patients.
Go to :
CONCLUSION
Based on the lessons learned from the pitfalls of the SYMPLICITY HTN-3 trial, improvements in device design (spiral type or ultrasound-mediated), technique (main renal artery and distal branch ablation), and trial design (control for adherence) have made RDN an attractive treatment option for HTN. Future trials need to focus on cardiovascular outcomes as well as BP reduction, adequate patient selection to show the greatest benefit, completeness of ablation without significant peri-procedural complications, and potential roles in treating other morbidities characterized by sympathetic overactivity. Furthermore, evidence is needed for the benefits of second-generation RDN devices in Asian patients.
Go to :
 XML Download
XML Download