

 PDF
PDF Citation
Citation Print
Print



Depression has been reported to be a risk factor of coronary artery disease (CAD).1) Another study about depression and CAD is set to be published in this current issue of the Korean Circulation Journal. However, it is somewhat different from previous studies.
Kim et al.2) reported a higher prevalence of depression in women with CAD (22% vs. 6.5% without CAD), but no significant increase was observed in men with CAD (5.5% vs. 3.4% without CAD). Although women have been acknowledged to be more susceptible to depression than men,3)4)5)6) this large sex disparity has not been reported. Interestingly, the prevalence was similar to that reported in previous studies (20–30% in women with CAD or acute myocardial infarction, and 5% in the general population)1) except for men with CAD.
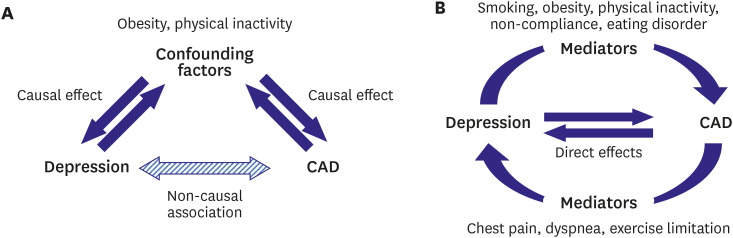
Interpreting the results requires caution as the study is cross-sectional and observational, with misclassification being the most worrisome source of error. The diagnosis of CAD was not medically verified, but based on a survey. People might have thought of chest discomfort and/or dyspnea from psychogenic origins as cardiac problems. In addition, we cannot determine the exact relationship between CAD and depression. From the previous studies, the relationship seems to be bidirectional, and complicated with various mediators and confounding factors such as diabetes mellitus, smoking, physical inactivity, obesity and non-compliance (Figure 1). The relationship and the methods of analysis are interesting issues in epidemiology and biostatistics.
Nevertheless, the high prevalence of depression (up to 30% in women younger than 65 years) has important clinical implication. As the authors have quoted, depression has a significant impact on the prognosis of CAD regardless of the onset.7) Depression itself is a serious disease that needs to be addressed. Hence, even cardiologists should pay attention to the mental health status of their patients, especially young women. It would be worthwhile to include a screening protocol for depression before discharge or at the diagnosis of CAD.
 XML Download
XML Download