

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Due to the continuing coronavirus pandemic, there is a growing interest in digital healthcare devices.12 From media reports and other available information, it seems that the era of accessible digital healthcare has begun. New and diverse information and communication technologies (ICT) are being utilized in the digital healthcare market every day.34 Digital healthcare devices with sensors that measure various biometric data and a variety of applications that act as platforms to store and analyze measured data have been released.567 Digital healthcare devices are being developed to increase miniaturization and multifunctionality and improve data analysis capabilities.
However, if we look at the success of digital healthcare from the perspective of medical professionals, the story is different. The public expects digital healthcare to solve issues within the medical field, but the reality diverges. Contrary to the high expectations and evidence of its potential, digital healthcare has not been successful in the medical market.
Various issues in digital healthcare devices have been noted, such as lack of improvements in regulations of digital healthcare, lack of data standardization, privacy, and legal liability issues,8910 but even if all of these issues are resolved, it is unclear whether digital healthcare devices will be utilized on a mass scale. For instance, not all diabetic patients actively use digital glucometers because the digital glucometer seems unreliable or difficult to use. If patients check and act according to recommendations from their digital glucometer, they will become more active in managing their own blood glucose by using digital healthcare. Medical staff must approach digital healthcare based on real-world problem perception in the medical market, not a superficial approach. In particular, nurses, pharmacists, and paramedical professionals such as nutritionists and exercise trainers, who have close contact with patients, are the most supportive of the implementation of digital healthcare for patients. We need to further utilize digital healthcare to more clearly understand its limitations.
Go to : 
WHY AREN'T DIGITAL HEALTHCARE DEVICES CONSTANTLY BEING USED?
Most people who claim that having adequate medical data and making good use of health management apps will greatly benefit patients' health management are not those who work in the medical field, but those who work in the industry.11 This is simply an exaggeration based on a simple theory. In digital healthcare, digital healthcare devices are rarely used for more than a year, and their usage continuity is not high.121314 Nurses have reported that even if a hospital distributes digital healthcare devices to patients for free for clinical research purposes, it is often not used fully. Although patients may initially be interested in a new digital healthcare devices to some extent, they feel no need to keep using the device and do not comprehend the true value of the contents provided by the device. However, if the device provides medical value to users, they will use the device even if it is uncomfortable.
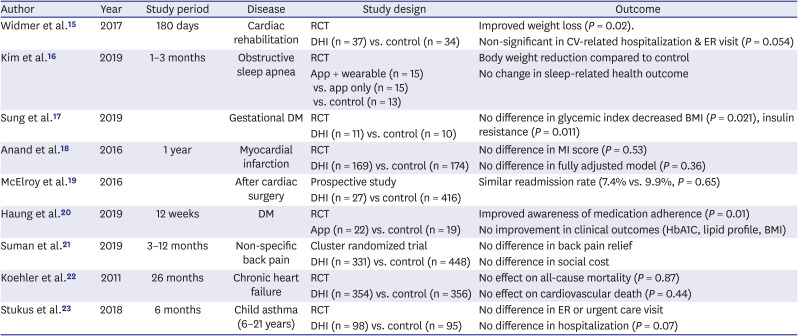
Data cannot be obtained unless the device is used (Fig. 1). When the user stops using the device, data are not created, and the digital healthcare device can no longer provide users with a valuable service based on the data. This is a vicious cycle, and we need to start by examining the possible value of digital healthcare devices. Actually, behavioral correction, weight control, glucose control, blood pressure control, etc., had good results with randomized controlled trial (RCT) using digital health technology in previous studies (Table 1). However, the outcomes of clinical trials for chronic diseases such as heart failure and asthma do not seem to have any meaningful results that reduce mortality, emergency room visits, and hospitalization.
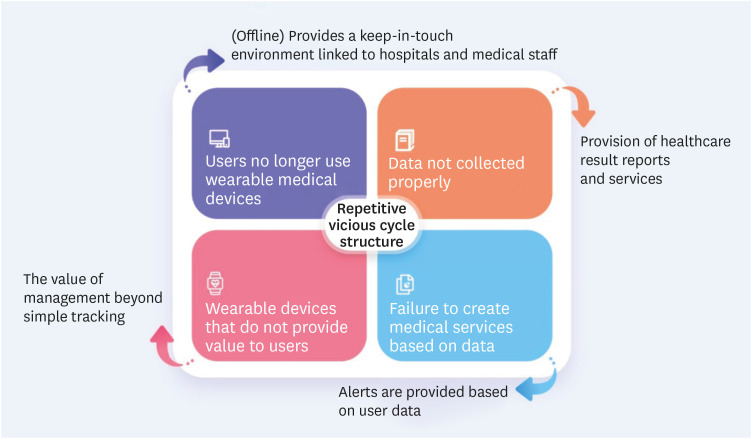 | Fig. 1Repetitive vicious cycle structure of the use of digital healthcare and avoidance alternative.When creating a single digital healthcare devices or app, it must be designed so that each of these steps can be carried out from the beginning. Therefore, collaboration between medical staff and industry professionals and active intervention by medical staff from the beginning is important.
|
Table 1
Digital healthcare studies that did not demonstrate significant effects
| Author | Year | Study period | Disease | Study design | Outcome |
|---|---|---|---|---|---|
| Widmer et al.15 | 2017 | 180 days | Cardiac rehabilitation | RCT | Improved weight loss (P = 0.02). |
| DHI (n = 37) vs. control (n = 34) | Non-significant in CV-related hospitalization & ER visit (P = 0.054) | ||||
| Kim et al.16 | 2019 | 1–3 months | Obstructive sleep apnea | RCT | Body weight reduction compared to control |
| App + wearable (n = 15) vs. app only (n = 15) vs. control (n = 13) | No change in sleep-related health outcome | ||||
| Sung et al.17 | 2019 | Gestational DM | RCT | No difference in glycemic index decreased BMI (P = 0.021), insulin resistance (P = 0.011) | |
| DHI (n = 11) vs. control (n = 10) | |||||
| Anand et al.18 | 2016 | 1 year | Myocardial infarction | RCT | No difference in MI score (P = 0.53) |
| DHI (n = 169) vs. control (n = 174) | No difference in fully adjusted model (P = 0.36) | ||||
| McElroy et al.19 | 2016 | After cardiac surgery | Prospective study | Similar readmission rate (7.4% vs. 9.9%, P = 0.65) | |
| DHI (n = 27) vs control (n = 416) | |||||
| Haung et al.20 | 2019 | 12 weeks | DM | RCT | Improved awareness of medication adherence (P = 0.01) |
| App (n = 22) vs. control (n = 19) | No improvement in clinical outcomes (HbA1C, lipid profile, BMI) | ||||
| Suman et al.21 | 2019 | 3–12 months | Non-specific back pain | Cluster randomized trial | No difference in back pain relief |
| DHI (n = 331) vs. control (n = 448) | No difference in social cost | ||||
| Koehler et al.22 | 2011 | 26 months | Chronic heart failure | RCT | No effect on all-cause mortality (P = 0.87) |
| DHI (n = 354) vs. control (n = 356) | No effect on cardiovascular death (P = 0.44) | ||||
| Stukus et al.23 | 2018 | 6 months | Child asthma (6–21 years) | RCT | No difference in ER or urgent care visit |
| DHI (n = 98) vs. control (n = 95) | No difference in hospitalization (P = 0.07) |
RCT = randomized controlled trial, DHI = digital health intervention (such as app or digital healthcare devices and so on), CV = cardiovascular, ER = emergency room, DM = diabetes mellitus, BMI = body mass index.
![]()
Go to :
DO DIGITAL HEALTHCARE DEVICES CONTINUE TO PROVIDE MEDICALLY VALUABLE INFORMATION TO USERS?
In the past, it was important that digital healthcare devices measure values accurately and were comfortable and stable.72425 Using a device or app that is not suitable for the user results in poor healthcare.26 However, while accuracy and comfort are important, these are the minimum requirements for users and do not determine the long-term use of the devices. If the data generated by the digital healthcare devices are not properly analyzed and if the user is not continuously provided with meaningful new information, they have no reason to continue using the device. The question arises: “Will digital healthcare devices really provide something valuable to the user?” Currently, the data measured on devices and the information provided to the user are extremely simple. Today's digital healthcare often only tracks an aspect of health and provides users with simple, rough data.27
When explaining treatment in a hospital, medical staff and paramedical professionals use various medical data, such as glucose levels, medication consumption, or laboratory test results measured in the hospital,2829 to inform patients of their personalized treatment, while digital healthcare devices do not explain treatment solutions in detail to patients.26 If digital healthcare requires patients to check, manage, and track data on their own, they should be able to feel the effects, or else they will not be motivated to use the digital healthcare devices.
To do this, users need to know how to manage their own data. Medical staff must teach and encourage users to be able to analyze and manage their patient-generated healthcare data (PGHD).30 Through this process, users should be able to find medical values from the digital devices. In addition, medical staff should motivate users to continue to use digital healthcare devices to collect PGHD. Medical staff should not only focus on providing personalized customized content to users but also help them understand what kind of customized content they need. However, this is not an easy task, because medical staff are often not experienced in the use of digital healthcare. We need to train paramedical professionals about digital healthcare management to communicate with and educate physicians and patients about the devices and their uses. It is difficult for physicians alone to promote the use of digital healthcare, so these trained digital healthcare professionals composed of nurses, pharmacists, nutritionists, and exercise trainers must assist patients to make them understand and utilize digital healthcare devices.
Go to :
ARE MEDICAL VALUES BEING COMMUNICATED TO USERS PROPERLY?
Digital healthcare aims to change the patient's lifestyle, but it is better to abandon the expectation that the use of simple digital healthcare devices and apps can artificially change lifestyles.31 In addition, contrary to the expectations of developers and medical staff, users are unfamiliar with the medical data and charts provided by existing medical apps,26 and they are not sure what their measured data means (Table 2). Users do not specifically know what behavior changes they need to make from looking at medical data and information, and there is not enough content to lead to changes in behavior. Digital healthcare devices cannot make use of human touch for interpretation of reports; therefore, instructions are interpreted by patients as unnecessary spam messages. To overcome this, it is necessary to determine what kind of behavioral changes will be recommended to users by seeing their accumulated tracking data. Educating patients about how to utilize the device and understand its value are important, but the way patient health is measured is more important when they do not recognize it. Digital healthcare devices increasingly require automatic measurement and storage of information and recorded data in a non-invasive, continuous way.42829
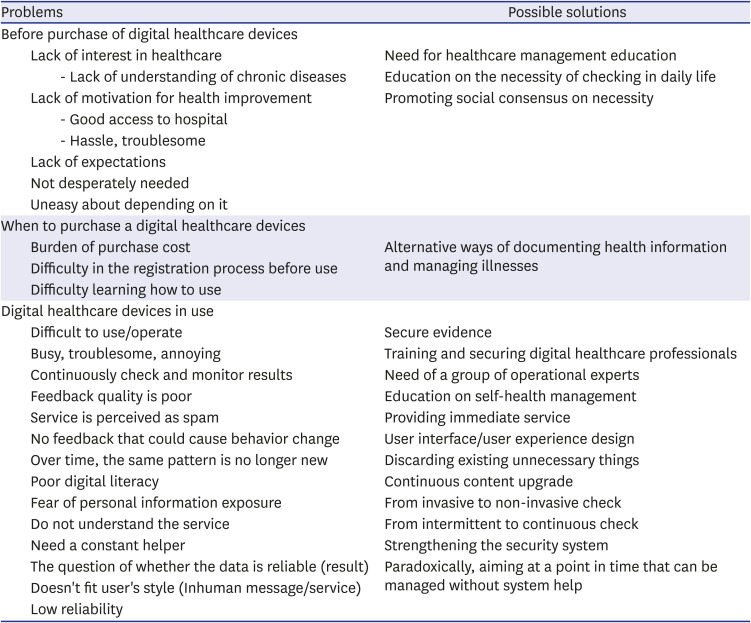
Table 2
Reasons why users do not use digital healthcare constantly
![]()
Further, self-analysis of the data generated from devices is important, but it is more important to create a healthcare service that blends into the patient's daily life, so that they can continuously create data.4 Ensuring that users keep using the device is a top priority. Only then will we be able to determine if the device is working properly.
Various digital healthcare devices, such as continuous glucose monitoring systems (CGMSs) that allow patients to continuously monitor and manage their own blood sugar, are the best examples of digital healthcare devices on the market today.43233 In addition, various efforts have been made to establish a service system for medical staff that actively utilizes medical information. This system uses input information to state the purpose and procedure of the system.434 If some technical part is supplemented, CGMSs will become the most practical example of digital healthcare. However, several studies have emphasized that education on how to use the device is very important.35 Although the importance of digital healthcare devices and platforms is constantly being emphasized in digital healthcare fields, we must not forget that the participation of actual paramedical professionals plays a much more important role. In the digital healthcare field, paramedical professionals cannot just educate users about how to use devices but must also teach users to understand and analyze data from the digital healthcare devices and perform diet or exercise therapy. To do this, paramedical professionals need to comprehensively understand digital healthcare. If such a combination is possible, the utilization of CGMS will be more positive, and it will be a more meaningful example of digital healthcare.
Go to :
IS TOTAL CUSTOMIZED MEDICAL SERVICE POSSIBLE WITH JUST ONE DIGITAL HEALTHCARE DEVICE?
There are many digital healthcare devices that offer personalized content or predictive models based on data measured with just one digital healthcare device. However, can we realistically provide personalized and customized content or predictive models with a single digital healthcare device? The data that can be provided by one digital healthcare device is very limited. The creation of individualized treatment plans is possible only when a large variety of medical data are accumulated.
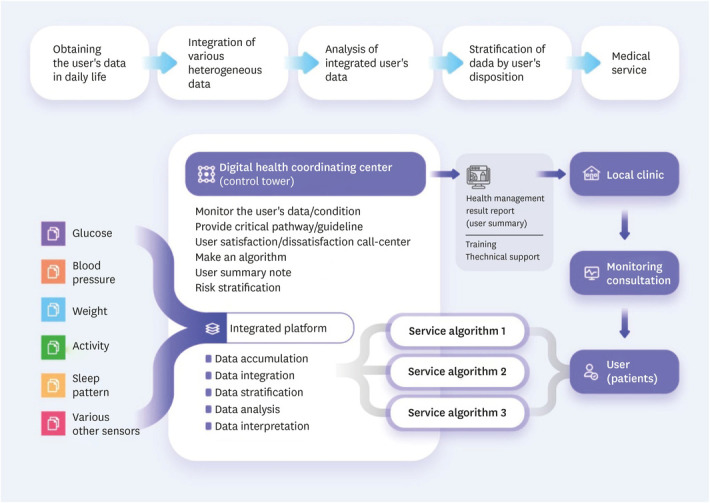
Usually, when a digital healthcare device is purchased, the device manufacturer includes a service app to provide medical services information. If a user buys a blood glucose meter and a pedometer tracker, they have to use two different apps. Of course, the greater the number of devices being used, the more information can be determined about the patient, but the more likely the utilization of some devices will stop. From the user's point of view, it is practically impossible to wear various devices, use numerous apps, and check results separately. Eventually, we will need a single customized service that can comprehensively analyze various medical data (Fig. 2) to provide valuable customized services to users based on the integration of various health data. It is necessary to provide an integrative platform and healthcare service that can be linked to various heterogeneous digital healthcare devices. By building an integrated medical platform, it will be possible to prevent and manage diseases based on customized data. Ultimately, digital healthcare aims to build a patient-centered, not hospital-centered, health ecosystem. Unless it is a single digital healthcare device, various factors such as operating and maintaining interoperability for various data collected from various sources, from data modeling to implemented algorithms and management methods, come into play.
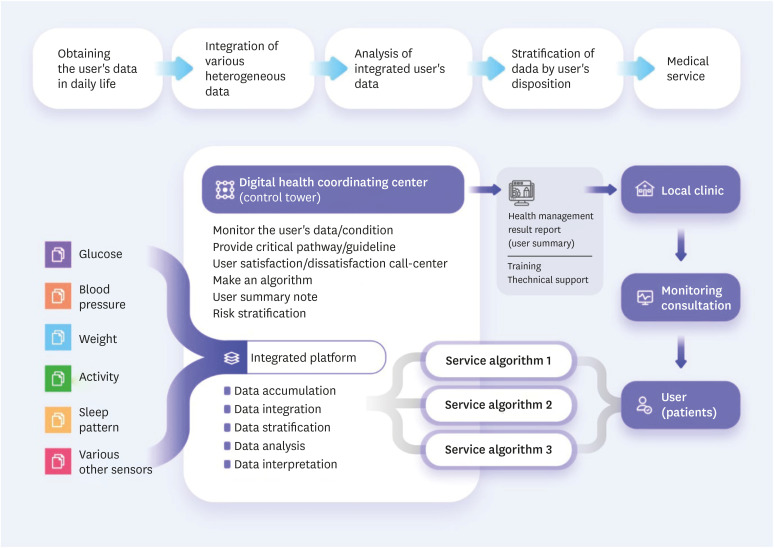 | Fig. 2Integrated digital healthcare devices linkage solution.One type of medical data does not provide adequate information about health conditions. It is necessary to use a variety of digital healthcare devices and to simplify the use of the app. It is also necessary to prepare an integrative system that can properly collect and analyze various data.
|
Go to :
PAY ATTENTION TO DIGITAL HEALTH CENTERS AND PATIENT-GENERATED HEALTH DATA
The concept of digital healthcare has been established,236 but the actual use of ICTs in the medical field is not simple. Data generated and collected from digital healthcare devices must be securely transmitted, stored, managed on a platform,636 and analyzed.
It is difficult to provide medical values to users with digital healthcare devices alone. It is absolutely necessary to supplement the digital healthcare devices with staff who can actively teach about and encourage the use of digital healthcare devices. Medical information that is useful to patients is successfully extracted only when the digital healthcare devices, platform, and medical service by paramedical professionals are in proper harmony.636 A digital health coordinating center (DHCC) that can support patients using digital healthcare and local clinics that provide medical services is essential.47 A DHCC should play a role in selecting, integrating, analyzing, operating, and continuing upgrades of an integrated medical platform. Multiple and diverse medical services should be managed as a single integrated medical service. For this, interaction between digital healthcare devices (interoperability, mutual authentication), security, gateways with external networks, and remote control are required. A DHCC can also serve as a clinical demonstration platform and test bed based on the interaction between company-hospital-community. It should then extend its role to not only educate patients and other medical staff but also to continuously provide medical services to users. For this, many new healthcare contents are required, and many medical services must be created and provided to users by paramedical professionals, which will help support local clinics that want to engage in digital healthcare. It is a way to clarify the role division and responsibilities of the local clinic and a DHCC and to maximize the cooperation between the two institutions. The foundation of all digital healthcare is the PGHD measured outside the hospital that the user generates.63637 The data measured by visiting a hospital once every few months are not representative of the user's condition. PGHD, which is measured continuously in real time, is the best explanation for an individual's situation and can be the basis for personalized treatment. In a DHCC, it is important to focus on how to use PGHD. Paramedical professionals should take note not only of the digital healthcare devices but of the data generated by it. First, they should be concerned about the quality of the data. To improve the quality of data, attention should be paid to the accuracy and convenience of the digital healthcare devices, and to data privacy, standardization, and quality management of collected data.38394041
Go to :
TRAINING OF PARAMEDICAL PROFESSIONALS FOR DIGITAL HEALTHCARE
Most patients are accustomed to visiting hospitals for healthcare. Therefore, users who may be familiar with digital healthcare in the context of lifestyle management (e.g., diet and exercise), do not have experience or knowledge about using digital healthcare measurement devices for actual healthcare. For most chronic diseases, nurses, pharmacists, nutritionists, and exercise trainers play important roles in patients' diets, exercise, and lifestyle management. This is because they can directly implement doctors' treatment plans and encourage patients. Human touch should be incorporated into digital healthcare with the active participation of paramedical professionals.
Unfortunately, there is no platform that can integrate and interpret data and convey information to patients. For the success of digital healthcare, paramedical professionals must interact directly with patients to educate users about how to use digital healthcare properly.424344 To maximize the medical value of digital healthcare, educating nurses and other paramedical professionals on how to use digital devices is necessary. The most important aspect of digital healthcare is that patients must be able to independently interpret and execute health data to manage their health. Therefore, there is a need to establish an extended role for various digital healthcare professionals, such as nurses, pharmacists, nutritionists, and exercise trainers in digital healthcare.
Go to :
CONCLUSIONS
Although digital healthcare device use has greatly improved, various challenges ensure users have low awareness and high distrust of digital healthcare. Trust issues emerge from lack of privacy protection and responsibility problems. It is important to receive feedback about digital healthcare from medical professionals,345 who must consider how to use the data in developing healthcare treatment plans and encourage active participation of patients. The data can be used to complement data gathered by medical staff. If the patient's PGHD can be collected, analyzed, and organized, artificial intelligence services for personalized healthcare for patients may become a reality.3746
ICT and sensor technology for digital healthcare devices will continue to develop, and the role of digital healthcare in everyday life will increase from simple lifestyle management at present. It will likely be used in the management of chronic diseases where it has significant potential, such as diabetes mellitus, hypertension, hyperlipidemia, and obesity. The field of customized healthcare services using PGHD can also be expanded. To this end, efforts must be made to utilize the true potential of digital healthcare to provide valuable information to both patients and healthcare providers. Digital healthcare devices will inevitably be used to improve treatment, so research from medical professionals about how to use these tools most effectively is necessary.
Go to :
 XML Download
XML Download