

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Past evidence has revealed the importance of breakfast and its positive effect on health condition and productivity. Breakfast consumption is associated with a lower body fat content and a healthier cardiovascular profile [1]. Moreover, skipping breakfast is related to an increased risk of degenerative diseases, such as type 2 diabetes mellitus [2]. Furthermore, breakfast consumption positively affects children and adolescents' academic performance and behaviors, particularly in mathematics and arithmetic [3]. It has been suggested that breakfast should provide at least 20% of the daily energy intake to enhance cognitive performance [4]. However, many adolescents around the world and within various socioeconomic status (SES) cohorts, reportedly skip breakfast. A recent study in Ghana reported that > 30% of 1,195 teenage students had breakfasts for < 4 days a week, and it appeared that students with a low SES had a lower breakfast frequency than the students from a higher SES [5]. In addition, a study of middle and upper socioeconomic classes in India reported that 37% of 203 adolescents skipped their breakfasts frequently [6]. In Indonesia, skipping breakfast is common among school children and teenagers. Previous research with a small sample size conducted on breakfast from 2002 to 2011 showed that approximately 16.9% - 59% of primary school children in some big cities do not eat breakfast [7]. There are no national data regarding skipping breakfast in adolescents, but many small studies in several major cities in Indonesia show a similar pattern as that observed in children. A study among high-school girls in Surabaya observed 58% breakfast skippers [8], in Bogor city it was 54.4% [9], and in Makassar it was 41.2% [10]. A 2016 study in Makassar reported that 37% of high-school students did not have a daily breakfast [11].
In addition to the high frequency of skipping breakfast among children and adolescents, the quality of breakfast is also a concern since the nutritional quality of their breakfast consumption may not meet the recommended daily allowance (RDA; 15–30% of RDA). Previous research based on secondary data within the Indonesian Basic Health Survey 2010 [12] investigated the types of breakfast food consumed by 35,000 children aged 6–12 years and reported that 44.6% of children consumed a low nutritional quality breakfast. Approximately 44.6%, 35%, 68%, 85%, 89%, and 90.3% of children consumed breakfast with < 15% RDA for energy, protein, vitamin A, iron, calcium, and fiber, respectively [13]. Other research using secondary data from the Southeast Asian Nutrition Study analyzed breakfast consumption among 2,629 Indonesian children aged 2–12.9 years and observed that only 31.6% had an adequate quality breakfast, defined as breakfast-provided energy, protein, vitamin and minerals of > 25% of RDA [14]. Moreover, that research observed that older age and children with a lower SES tend to consume a poor nutritional quality breakfast. Research among 6–12-year-old children in Jakarta observed that the breakfast meal contributed a high proportion of carbohydrate and fat requirements but a low proportion of fiber and micronutrients [15]. The study also showed that the low-medium SES group had low nutrient intakes during breakfast and consumed a low level of several micronutrients. Studies among adolescents indicate average energy and protein intakes from breakfast of approximately 15% and 20% of RDA, respectively [9], but only 10% of adolescents had a high-quality breakfast [8]. Therefore, improvements in breakfast habits and quality of school children and adolescents in Indonesia require serious attention, especially if it is related to the role of breakfast in providing nutrition levels that allow the achievement of optimal academic abilities. Moreover, adolescents experience growth spurts, which require an adequate intake of energy and other nutrients from their daily diet to support optimal growth and development [16].
A national school breakfast program (SBP) has been initiated and implemented in many countries as one approach to promoting the consumption of a healthy breakfast and improving breakfast practices, nutritional status, and school performance among children and adolescent, particularly for low-income families [1718]; however, an SBP has not been available to Indonesian adolescents. Since 2016, Indonesia has piloted a school feeding project to provide a breakfast meal for primary school children in 2 provinces, and the results showed improvements in school attendance and achievement as well as energy, protein, and iron intakes of the children participating in the project [19]. Regardless of the positive effects, low coverage is an issue; hence, increasing the feeding program's coverage to all targeted school children has been suggested. In 2014, the Ministry of Health of the Republic of Indonesia established the Indonesian Dietary Guidelines (Pedoman Gizi Seimbang) [20] that includes breakfast promotion as one of the 10 messages to achieve a balanced nutrition status; however, it has been reported that most Indonesian adolescents do not follow the guidelines [21].
Since it is recognized that a lack of knowledge and awareness is one of the determinants of nutrition-related problems [22], a nutrition education (NE) program can be an additional approach to overcoming unhealthy breakfast behaviors in adolescents. NE can help younger people obtain reliable information that may influence them to make healthier choices, leading to healthier eating habits. NE was reported to effectively influence knowledge, attitude, and practices among school-aged children when applied using a behavior-focused design based on a theoretical framework and delivered in an appropriate manner [23]. Although NE has been included in the national school curriculum in many countries, a NE program specifically aimed at adolescents is not currently a priority in Indonesia, and it has only been integrated into certain school subjects and provided in small doses and few sessions [2425]. Furthermore, these studies indicated many factors that challenge the inclusion of NE in the Indonesian national school curriculum, including lack of teacher capacity, lack of school support in terms of funding and time constraints, and lack of external environmental support, including a lack of parental nutrition awareness. Alternatively, delivering school-based NE outside the classroom or as an extracurricular activity can help adolescents achieve better knowledge, attitude, and related eating habits.
Schools are the most efficient venue for health education targeting dietary changes or other health-related behaviors in adolescents and school-aged children [2627] as they can provide the opportunity to teach young people about food and nutrition and demonstrate the importance of a balanced diet for future health [27]. It has been suggested that an efficient school-based NE program should be comprehensive; that is, it should target not only knowledge and skills but also person-related factors, food preferences, and sensory factors [28]. Moreover, support from parents and teachers and external sources can strongly help achieve a positive outcome [29]. To accommodate these various elements for success, NE should be designed as a multi-strategy intervention.
Multi-strategy NE intervention was reported to have positive effects on changes in adolescent dietary intake and other nutrition-related behaviors in a review of previous studies in European countries, Australia, and the USA [30], but only one of the reviewed studies had the objective of changing breakfast frequency in relation to an obesity prevention program that resulted in no change [31]. Thus, there is limited availability of reports investigating multi-strategy NE approaches to breakfast habit improvement. A study in Tunisia adopted a multi-strategy intervention, a combination of interactive lessons and activities in a school-based NE program, to improve knowledge and motivation toward breakfast consumption among adolescents [32]. The intervention was integrated into the school's curriculum and delivered by pre-trained teachers in collaboration with medical doctors. The study included a large sample of adolescents representing various socioeconomic backgrounds; however, more than half of the sample exhibited good daily breakfast habits during the pre-intervention period. Other studies with a similar design reported improvement in personal influences as well as breakfast frequency and quality in adolescents after the implementation of multi-activity NE sessions that were delivered by teachers and nutritionists [3334]. However, the Elseifi et al. [34] study involved a small convenience sample of female students and covered middle-upper socioeconomic settings [3334]; hence, the generalizability of their results to other SES groups is questionable. Moreover, the long-term effect of the intervention was not assessed.
One of the challenges in youth NE is the difficulty in attracting the attention of the target population. Therefore, it is important to use up-to-date trendy approaches for this purpose. A qualitative report on Indonesian public health workers and experts as informants revealed that technology, such as a mobile phone, is a potential key engagement strategy as there was high cell phone use among Indonesian youth [22]. Furthermore, there is growing evidence of the positive effect of health promotion provided through text messages related to health behavior in clinical care and preventive intervention [35]. Another study has shown that NE delivered through a combination of conventional nutrition lectures, brochures, and text messages has a positive effect on dietary intake and behavior of young adult-university students [36]. A limited number of studies have included the use of social media platforms to deliver health education to adolescents, including those from low-middle income families, and provided modest evidence regarding social media's effectiveness in changing nutrition knowledge and nutrition-related behaviors, but few have included long-term follow-up to examine the sustainability of behavioral changes [3738].
Improving nutrition behavior through multi-strategy NE that combines printed materials with interactive activities, skills development, and motivational text messaging can result in positive breakfast-related personal influences and long-term behavioral changes. To the best of our knowledge, a limited study empirically tested the efficacy of a multi-strategy intervention in a low-middle-income community and only included adolescents with unhealthy breakfast practices as subjects. This study measured the effect of multi-strategy NE on personal influences toward breakfast (i.e., knowledge, attitude, self-efficacy, and motivation), breakfast frequency, and nutrient intake from breakfast. Further, this study assessed whether the intervention changes can be retained over a longer period. The results were expected to determine which NE model applies to adolescents with low-mid SES in Indonesia and potentially prove effective in improving their breakfast habits.
Go to : 
SUBJECTS AND METHODS
Study design
This study applied a cluster randomized controlled trial design, treated a school as a study cluster, and randomly assigned the schools to treatment and control groups (CGs). The treatment group received multi-strategy NE containing printed materials, mobile phone text messages, social media activities, cooking demonstrations, and competitions, while the delayed CG received only printed NE materials. Pre- and post-tests and follow-up tests were conducted in both groups.
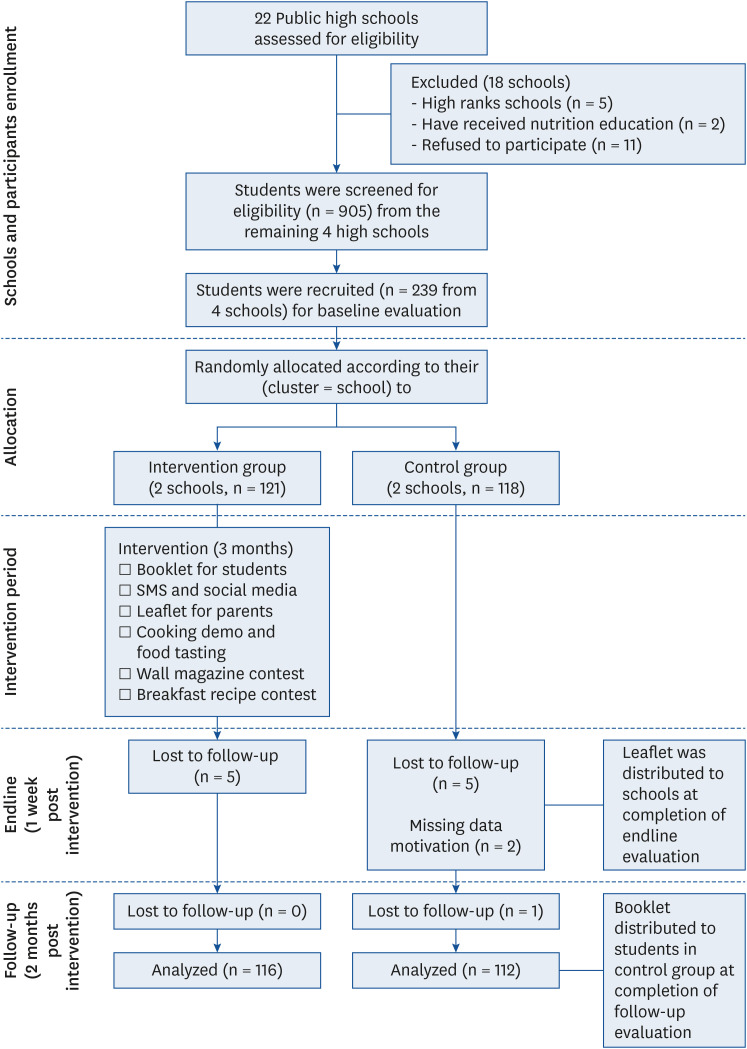
To be included in the study, 22 public schools (as designated by the Department of Education of Makassar City) were screened for eligibility according to the following inclusion criteria: non-high ranking public high schools representing low-to-mid socioeconomic class, never received any previous NE intervention, and the school's principal approved participation in the study. Among 22 schools, 5 schools were categorized as high-rank schools, 2 schools received NE intervention within the past year, and eleven schools refused to participate; thus, only 4 schools were eligible for enrollment in the study.
Participants
Following the initial school screening, students from each eligible school were screened for eligibility as study participants based on the following criteria: 1) registered in grade 10 at the time of data collection, 2) habitually having breakfast ≤ 4 times a week, 3) have access to a cellular phone, and 4) provide consent to participate in the study. In total, 905 students were screened and 346 of them met the inclusion criteria. Overall, 60 eligible students from each school were randomly selected by drawing papers containing the student's name. Finally, 239 students agreed to participate in the baseline data collection procedure and provided consent for participation. After baseline data collection, the principal investigator randomly allocated 2 schools to the intervention group (IG) and 2 schools to the CG. As a result, 121 and 118 students were included in the IG and CG, respectively, at the pre-intervention level. At the end of the intervention, 5 students in the IG and CG withdrew due to moving to another school outside of the study area. Furthermore, one participant in the CG was excluded during the follow-up period because of a similar reason. Finally, 228 participants completed the study (Fig. 1).
This study was conducted according to the guidelines laid down in the Declaration of Helsinki. All procedures involving human subjects received ethical clearance approval from the Faculty of Medicine Hasanuddin University Health Research Ethic Committee (Reference No: 606/H4.8.4.5.31/PP36-KOMETIK/2017). All participants were informed about the study, and all participants and their guardians provided informed consent.
NE intervention
The developed NE intervention was based on a previous study [39] that applied a NE conceptual model [40] that adapted the theory within the transtheoretical model [41]. The intervention lasted for 3 months, during which the participants received education via illustrated booklets and leaflets, short message services (SMS), and Line/WhatsApp messenger, cooking demonstration, food tasting, wall magazine contests to promote healthy breakfast eating, and breakfast recipe contests. Each student in the IG received a booklet on the importance of breakfast, which included suggestions and motivations to overcome breakfast consumption barriers. The purpose and content of the booklet were directly explained to the participants, and they were encouraged to read the booklet frequently during their leisure times at or out of school. They could further discuss the booklet content or other adolescent nutrition-related issues with the research team through mobile phone communications. Educational and motivational messages were also delivered individually through SMS and Line/WhatsApp messenger for 4 consecutive weeks. A cooking demonstration was conducted in each of the intervention schools and involved researchers and field staff cooking 4 simple but healthy breakfast menus. The cooking demonstration was attended by the school principal, teachers, and participating students and their respective parents. The students' representatives were invited to cook the menus by themselves in front of the audience, and all attendees tasted the cooked food together. A leaflet containing information about the benefits of breakfast and a healthy breakfast recipe was distributed to the parents with the cooking demonstration invitation, which was given to the students 3 days before the event. During the cooking demonstrations, researchers explained the leaflet's content. A wall magazine contest was conducted to promote healthy breakfast consumption for all grade 10 classes in the IG. One team represented one class, and at least one team member was a participant in this study. The study participants were expected to work with, and deliver educational information they have received to, their classmates. The contest to create a healthy and simple breakfast recipe was limited to the study participants, but they were expected to work with their parents or family members. The best 3 wall magazines and recipes were displayed in each school's library, and the winners of these contests received awards. The control schools received leaflets at the completion of endline data collection. Moreover, students in the CG received booklets after the follow-up data collection.
Study instrument and measures
Researchers collected data in 3 periods: baseline (pre-intervention), endline (post-intervention), and follow-up (2 months post-intervention). A validated self-administrated questionnaire, developed in previous research among high-school students in Makassar, with Cronbach's alpha coefficients ranging from 0.792 to 0.832 (indicating good reliability) and item-to-total-item correlations of > 0.40 (indicating good construct validity) [39], was used to measure breakfast-related personal influences during each period. The questionnaire comprised 12 questions with multiple choice answers to assess knowledge, 8 questions to assess breakfast attitudes, and 7 questions to assess self-efficacy. The response scales for the latter variables ranged from strongly agree (score = 4) to strongly disagree (score = 1). Motivational status was assessed via one question regarding the current stage of change of the participant toward changing his/her breakfast habit with 5 responses: no intention to change (pre-contemplation), intend to change but not sure (contemplation), decide to change (decision), start to change (action), and successful in change (maintenance). These responses were relevant to the motivational-to-action phase depicted in the conceptual framework for NE [40] and the stages of changes included in the transtheoretical model [41]. A subject's breakfast habit was measured during the 3 data collection periods by asking about the frequency of breakfast consumption in a week. Nutrient intake (e.g., energy and protein intake from the breakfast meal) levels were based on the food consumption data collected during each collection period. All foods and drinks consumed at breakfast were reported in interviews using an unstructured breakfast recall for 3 consecutive days. Food pictures published by the Indonesian Ministry of Health in 2014 were used to assist portion size estimation during food recall.
Data analysis
A participant's total score was calculated for each knowledge, attitude, and self-efficacy variable. For motivation variable assessment, frequency distribution analysis was performed to examine the distribution of data in each category according to the questionnaire's items. The average intakes of energy and protein from breakfast were analyzed based on output from the NutriSurvey program calculation. To answer the research objectives, data for each variable collected from the pre-, post-intervention, and follow-up periods were paired and compared. Normality testing indicated that the data were not normally distributed; thus, further analyses were conducted using non-parametric tests. To assess the effect of the NE intervention, differences in each variable in each group between the pre- and post-intervention periods were determined using Wilcoxon and McNemar tests. Differences in each variable between the pre-intervention and follow-up periods in IG were assessed to determine the intervention's long-term effect. Differences in each variable between the groups at each data collection period were also tested using Mann-Whitney and χ2 tests. Data are expressed as means and standard deviations as well as percentages, with P < 0.05 was considered significant data.
Go to :
RESULTS
Sample characteristics
Table 1 presents a summary of the characteristics of respondents and their parents. There were no significant differences in baseline characteristics between the study groups, indicating the selected school cluster was relatively homogeneous. Most respondents were female and aged 16–17 years, suggested that skipping breakfast tends to be more common in female and older adolescents. More respondents' fathers had informal jobs (57.3%), such as an owner of a small enterprise or a daily worker, and those who were unemployed (7.1%, data not shown) were also included in this category. Most mothers worked in the informal sector (84.1%), a category that included unemployed mothers (66.1%, data not shown). Most fathers and mothers had an education level of high school and above.

Table 1
Characteristics of respondents and their parents at baseline according to study groups
![]()
Changes in personal influences
Fig. 2 depicts changes in knowledge, attitude, and self-efficacy scores in both study groups during the 3 data collection periods. Mean knowledge score in IG improved (Δ0.15) between the pre- and post-intervention periods, but the difference was not significant (P > 0.05); moreover, knowledge scores did not change (Δ0.0) between the pre-intervention and follow-up periods. In contrast, knowledge score in CG improved between the pre- and post-intervention periods (Δ0.56) and between the pre-intervention and follow-up periods (Δ0.01); however, neither change was significant (P > 0.05). Differences in knowledge scores of the IG and CG were significant at follow-up (Δ0.66, P = 0.01) with the IG achieving a significantly higher mean score than that of CG.
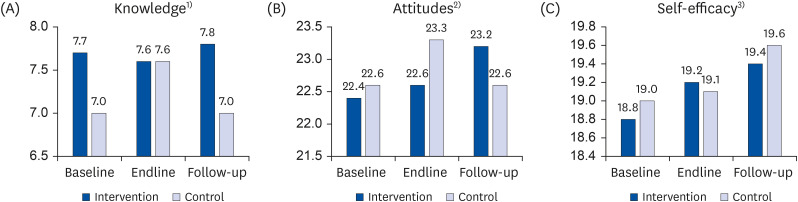 | Fig. 2Comparison of the mean scores of (A) knowledge, (B) attitudes, and (C) self-efficacy toward breakfast consumption between the IG and CG at baseline and endline and baseline and follow-up.CG, control group; IG, intervention group.
1)P-value knowledge score IG vs. CG at baseline and follow-up < 0.05, Wilcoxon test.
2)P-value attitudes score in baseline vs. follow-up in IG < 0.05, Mann-Whitney test.
3)P-value self-efficacy score in baseline vs. follow-up in IG < 0.05 Wilcoxon test.
|
There was no significant change in attitude score in IG between the pre- and post-intervention periods (Δ0.22, P = 0.55), but significant improvement was noted between the pre-intervention and follow-up periods (Δ0.74, P = 0.02). There was no significant change in attitude scores in CG, either at post-intervention or follow-up periods (P > 0.05). Differences between the 2 groups were not significant at post-intervention or follow-up periods (P > 0.05).
A significant difference in self-efficacy score in IG was only observed between the pre-intervention and follow-up periods (Δ0.59, P = 0.05). The change in self-efficacy score between post-intervention and follow-up periods in CG was not significant (P > 0.05). In addition, self-efficacy scores were not significantly different between the groups at intervention and at the 2-month follow-up (P > 0.05).
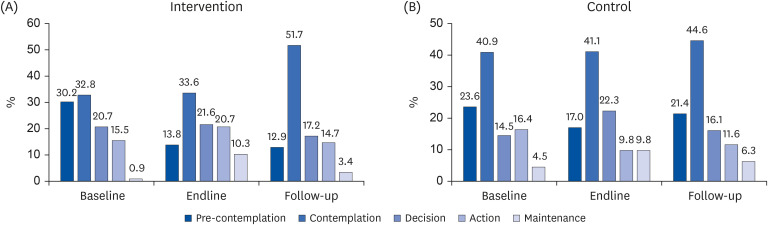
A significant difference was noted in motivation to change breakfast consumption behavior in IG between the pre- and post-intervention periods (P = 0.02) and between the post-intervention and follow-up periods (P = 0.02). In contrast, no significant improvement in motivation to change was observed in CG either at post-intervention (P = 0.20) or at follow-up (P = 0.86) (Fig. 3). Although differences between groups were not significant at any of the 3 periods (P > 0.05), a greater increase in the number of students who changed in each motivational phase to the action phase (contemplation stage until maintenance stage) at post-intervention was noted in IG compared to CG (9.4% vs. 5.3% increase). Moreover, the number of students in the pre-contemplation stage decreased by 16.4% in IG, whereas it decreased only by 6.6% in the CG at post-intervention. The motivation improvement in IG was relatively stable, as shown by the increase in the number of students in the contemplation stage at follow-up (18% increase) compared to 4% increase in CG.
Changes in breakfast-related behaviors
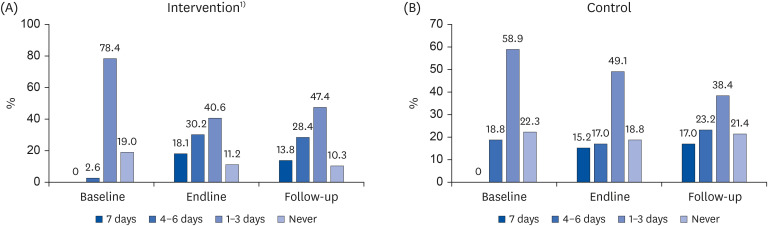
Fig. 4 shows that improvements in breakfast frequency were observed at post-intervention in both IG and CG. At pre-intervention, breakfast frequency significantly differed between the 2 groups (P < 0.01), with more students in IG (97%) than in CG having a poor breakfast habit. At baseline, fewer students in IG had a frequent breakfast (i.e., ≥ 4 days a week) compared to their counterparts in CG (2.6% vs. 18.8%). However, students in IG had a significantly improved breakfast frequency (P = 0.05) at post-intervention. More students in IG than in CG reported having a frequent breakfast at post-intervention (48.3% vs. 32.2%). The improvement of breakfast frequency in IG was retained at follow-up and was greater than that in CG (42.2% vs. 40.2% had a frequent breakfast), and the percentage of adolescents who never had one breakfast a week at follow-up was smaller in IG (10.3%) than in CG (21.4%).
An improvement in breakfast nutrient intake was noted in IG. The mean energy intake of breakfast in IG significantly increased post-intervention (Δ73.09 kcal, P = 0.01) and at follow-up (Δ49.15 kcal, P = 0.02). In addition, breakfast protein intake in IG increased post-intervention (Δ2.29 g, P = 0.08) and at follow-up (Δ1.5 g, P > 0.05), but the changes were not significant. In contrast, the increase in energy (Δ72.83 kcal, P < 0.01) and protein (Δ1.96 g, P < 0.01) were significant in CG, but only at follow-up. Moreover, mean energy and protein intakes were significantly higher in IG than in CG at post-intervention (Δ116.64 kcal and Δ3.23 g, respectively, P = 0.01) (Fig. 5).
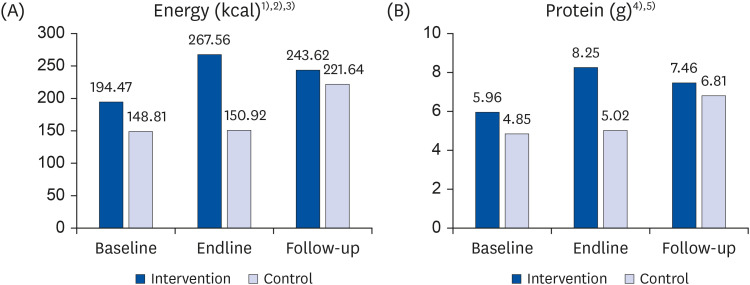 | Fig. 5Comparison of the mean (A) energy and (B) protein intakes from breakfast consumption between the intervention and control groups at baseline and endline and baseline and follow-up.
1)P-value mean energy intake between IG and CG at endline < 0.05, Mann-Whitney test.
2)P-value mean energy intake in IG, baseline vs. endline and baseline vs. follow-up < 0.05, Wilcoxon test.
3)P-value mean energy in CG baseline vs. follow-up < 0.05, Wilcoxon test.
4)P-value mean protein intake between IG and CG at endline < 0.05, Mann-Whitney test.
5)P-value mean protein intake in CG, baseline vs. follow-up < 0.05, Wilcoxon test.
|
Go to :
DISCUSSION
This study assessed whether a multi-strategy NE intervention could effectively improve adolescents' knowledge, attitude, self-efficacy, motivation, and behaviors related to breakfast in a low-mid SES setting of Indonesia. The results showed that the intervention had relatively no effect on adolescents' knowledge but positive effects on adolescents' attitude, self-efficacy, motivation, breakfast frequency, and breakfast nutrient intake (energy and protein), thereby demonstrating that the NE model applied in this study was effective in promoting healthy breakfast habits in adolescents with a low-mid socioeconomic background. This study also assessed whether changes resulting from the NE intervention can be sustained over a longer interval. The results showed that, at 2 months after the intervention had ended, attitude, self-efficacy, and motivation changes were retained in adolescents exposed to the NE intervention. Changes in breakfast frequency and breakfast energy intake level were retained at 2 months after the intervention, but the protein intake change was not maintained.
This study supports the results in a previous study [5], which showed that breakfast skipping is common in adolescent girls and those with a low-mid SES. Breakfast nutrient intakes were low in the present study and contributed less than 15% of the relevant RDA, which confirms observations in other studies [1542] revealing that adolescents with a low-mid socioeconomic background tend to consume low nutrient quality breakfasts. These findings suggest that breakfast habit improvements are critical in this portion of the population, and substantial interventions are needed to overcome this tendency.
This study shows that an NE intervention can promote positive changes in breakfast-related personal influence indicators, as well as breakfast quality and consumption frequency in adolescents with a low-mid SES. The results of an analysis using the Mann-Whitney test on outcome variables according to socioeconomic indicators (such as parental occupation in the formal and non-formal sector and the level of parental education) showed that there were no significant differences in those indicators between the intervention and CGs at post-intervention, except for knowledge. The knowledge score in IG was greater than that in CG (Δ0.82–0.98, P < 0.05) for adolescents who had parents working in the informal sector or with a higher educational level. Moreover, the knowledge score in IG was significantly higher than in CG at baseline, suggesting that adolescents' knowledge was potentially influenced by parental occupation and educational status. This finding is inconsistent with that in previous studies showing that an NE intervention can significantly improve study participants' breakfast-related knowledge [324344].
Significant improvement of attitude and self-efficacy in IG at follow-up indicates that the multi-strategy NE intervention had a long-term effect on breakfast-related personal influences. These findings are consistent with those of previous studies showing that multi-strategy NE has positive effects on adolescents' self-efficacy [32] and attitudes toward breakfast [43]. Moreover, the results of the present study demonstrate that a multi-strategy NE intervention has a positive effect on the subjects' motivation toward breakfast. The implementation of cooking demonstrations, contests, and motivational text messaging in this study possibly created emotional experiences [40], thereby contributing to the observed increase in participants' motivation.
The results of this study indicate that a multi-strategy NE intervention can have a positive effect on adolescents' breakfast behavior. This finding is consistent with those in previous studies showing that NE interventions can alter adolescents' breakfast consumption frequency [3233344345]. The improvement in breakfast frequency observed in this study was consistent with the improvements in adolescents' attitude, self-efficacy, and motivation, possibly the key for the observed positive effect of the NE intervention. A recent study among adolescent girls showed that self-efficacy improvement was associated with improvements in eating behavior, including breakfast consumption [46].
The improvements in breakfast-related personal influences and behavior in IG were larger than those in CG, suggesting that combining a conventional NE method, which relies on printed materials, with more interactive activities and the inclusion of technological advances hold promise for encouraging an eating behavior change in adolescents. Printed educational materials provided in this study might facilitate enhancements in the consciousness factor [40] of the participants who intend to increase their motivation and breakfast frequency. The addition of text messaging, group discussions through social media apps, and active methods such as cooking demonstrations, food tasting, and contests as intervention-induced reinforcement of printed materials could have contributed to the better results in IG. This study supports the usefulness of the recommendation to deliver NE through school-based and technology-based platforms as an intervention aimed at improving adolescent nutrition in Indonesia [47]. The use of technological advances should be considered a particularly useful strategy for the delivery of NE since such technology is important in the lifestyle of Indonesian adolescents.
Although parental involvement level was not measured, the inclusion of parents of the participants in this study, in terms of supporting the receipt of breakfast-related information through leaflets, cooking demonstrations, and recipe-based contests, could have contributed to the positive effect of the study intervention. It is recognized that parental involvement is a crucial component that can significantly impact multi-strategy NE programs in adolescents [30].
The recognition of intervention intensity as an important characteristic of a successful school-based intervention [48] is supported by the observations in the present study. The NE intervention in this study was delivered at a medium intensity according to evaluation criteria [48] such as intervention duration, contact frequency, personalization level, and reach of strategy influence. The authors suggest that a higher intensity intervention in which more time and resources were invested (i.e., intervention lasting for 6 weeks to 5 months) can result in greater positive dietary changes [48]. The present study's NE intervention was conducted over 3 months with weekly intervention visits, environmental and group level contacts, and the inclusion of students and their respective parents.
Although NE can increase an adolescent's breakfast consumption frequency and reduce breakfast skipping, the observed improvement in breakfast quality in this study was not satisfactory because at post-intervention and follow-up, the breakfast nutrient intake levels were still below 15% of RDA. This finding suggests that this NE initiative should be complemented with other interventions to stimulate larger changes in breakfast quality among this socioeconomic group. One possible supplement would be the provision of a good quality breakfast at school as there is evidence showing that school breakfast initiatives can broaden the types of foods and drinks that students consume during breakfast and improve the associated nutrient intake [49505152]. This approach can be implemented by expanding the current Indonesian school meal policy and pilot a school feeding program for middle and high-school students.
This study's findings provide unique results from a study population of adolescents with a low-mid socioeconomic background, a cohort that is currently understudied. Moreover, this study adds to the available literature on the role of multi-strategy NE as a school-based intervention to improve breakfast-related behaviors in adolescents that have been limitedly investigated in developing countries; for example, Indonesia. The studies also support increasing the use of technology-based platforms and their potential positive contribution to NE, particularly adolescent NE interventions. This study can provide input useful in developing future effective NE programs aimed at addressing nutritional problems among adolescents, but further study is required before implementing such programs in the community. Such research should be directed toward a more intensive use of social media or other technology-based interventions in delivering NE to adolescents. Moreover, the scope of NE research should be broadened to reach out-of-school adolescents. Also, more active involvement of parents, rather than just as voluntary participants, should be considered a means to changing breakfast behaviors.
A strength of this study is its limiting the inclusion of adolescents to those with a low-mid SES and poor breakfast habits. The intervention aimed at promoting healthier breakfast consumption and specifically targeted this vulnerable sub-group in Indonesia. Contamination of information in either of the groups was unlikely during the intervention; however, there is a possible presence of a social desirability bias during the endline, and follow-up data collection as this study applied self-administered questionnaires. The researchers and data collectors were not blinded, and that may have influenced breakfast food recall efficiency. Therefore, the findings from this study should be interpreted cautiously.
In conclusion, this research provides evidence that an infrequent, low-quality breakfast is a major problem in Indonesian adolescents and requires considerable attention. This study identified that school-based NE, particularly when delivered through a multi-strategy intervention, can facilitate the promotion of healthy breakfast consumption and encourage positive and long-term changes in breakfast-related attitude, self-efficacy, motivation, and behaviors of adolescents with a low-mid SES. The NE strategy in this study is applicable and promising for addressing the unhealthy breakfast habits of this particular group of adolescents. The NE approach in this study could be implemented as an extracurricular activity when its integration into the school curriculum is considered a challenge. Regardless, NE should be prioritized as a critical strategy to improve adolescents' healthy eating behavior and can lead to improvement of their nutritional status and performance. NE should be considered a crucial part of adolescent nutrition programs in Indonesia.
Go to :
 XML Download
XML Download