

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Childhood obesity is a substantial threat to public health and is associated with numerous health problems, including diabetes, hypertension, hyperlipidemia, sleep disturbance, and asthma [1234]. Moreover, childhood obesity is also correlated with a high risk of metabolic diseases, cardiovascular disease, and excessive weight in adults [5678]. According to the World Health Organization (WHO), the number of obese children and adolescents worldwide has increased tenfold over the past 40 years [9]. In Korea, the prevalence of overweight and obese children has continued to increase over the past several decades [10]. In particular, the prevalence of obesity in Korean male students in 2013 was 26.4%, which was 2.1% higher than the Organization for Economic Co-operation and Development (OECD) average of 24.3% [11]. Altogether, the rising prevalence of childhood obesity and the resulting present and future health concerns clearly establishes that prevention and correction of childhood obesity is urgently needed.
Although childhood obesity is arguably more serious, being underweight in middle and high school is also of concern. For example, a study of 11–17 years old Korean students found that underweight students accounted for 29.4% of middle school males, 14.7% of high school males, 10.9% of middle school females, and 16.0% of high school females [12]. Similar to being obese, being underweight also causes health problems, such as depression and sleep disorders [131415]. In addition, previous studies have reported that underweight adolescent females are more likely to use extreme weight management methods if they have misperceptions about weight [16]. It is therefore necessary to impart proper education to students for the prevention of obesity, as well as proper weight management and perception.
Many factors contribute to childhood obesity, including unhealthy dietary behaviors and lack of physical activity [17181920]. An analysis of the Korea Youth Risk Behavior Web-based Survey from 2014 indicated that 28.2% males and 28.9% females skipped breakfast for more than 5 days during the past week, and 41.7% males and 34.4% females drank sweetened beverages more than three times in the past week [21]. To combat these and other unhealthy dietary behaviors in youth, school-based weight-control programs have been implemented in many schools, educating the students about weight control, weight perception, and nutrition. The effectiveness of school-based weight-control programs has been ably demonstrated in previous studies [222324]. These programs help to reduce the body mass index (BMI), fat mass, body dissatisfaction, and high-risk eating attitudes and behaviors, as well as increase self-esteem among students [2526]. However, studies examining the effects of school-based weight-control programs across multiple institutions are rare.
Based on previous studies, the present study was designed to identify the difference in inappropriate weight control efforts and health status according to BMI. This study aimed to investigate the association between participation in the school-based weight-control programs and inappropriate weight control efforts, dietary habits, and behavior of students at multiple institutions. Our results add to evidence supporting the results of school-based weight-control programs, and provide relevant data for future efforts to combat childhood obesity.
Go to : 
SUBJECTS AND METHODS
Participants
The study population comprised 1,742 students from 15 high schools and 15 middle schools in Korea. To collect a representative group of Korean students, we recruited schools to participate in collaboration with the Korean Association of Secondary Education Principals, and participants were evenly sampled nationwide. Special education schools were excluded from this study. The purpose and process of the study were explained to all students of the selected 30 schools; 2,569 students agreed to participate, and finally 1,742 students completed the survey. This study was approved by the Institutional Review Board of Seoul National University Hospital (IRB No.1407-127-597).
Instruments and procedure
The survey was conducted from August 2014 to January 2015. A skilled research assistant and school nurse administered the printed self-reported questionnaire to students, and facilitated them to respond to the questions. Baseline demographic variables included sex, age, and school year of the participant. Geographical information and name of the school were also collected. The individual BMI of all participating students was calculated by dividing weight in kilograms by height in meters squared. According to the clinical practice guideline for diagnosis of pediatric obesity, ‘Overweight’ is defined as a BMI at or above the 85th percentile and below the 95th percentile of the same age and sex, ‘obesity’ is defined as a BMI at or above the 95th percentile, and ‘Underweight’ is defined as a BMI at or below the 5th percentile [27].
Health status
Questions regarding the physical, mental, social, spiritual, and overall health status of students were included in the survey [2829]. These five dimensions of health were measured by the following questions: 1) “Physical health is the condition of having normal strength, without illnesses and injuries. How do you rate your current physical health status?”; 2) “Mental health is the condition of being mentally stable, capable of overcoming stress. How do you rate your current mental health status?”; 3) “Social health is the condition of maintaining good social relationships, functioning one's role properly. How do you rate your current social health status?”; 4) “Spiritual health is the condition of finding a value in life through volunteering, religious experience, and meditation. How do you rate your current spiritual health status?”; and 5) “Considering your physical, mental, social, and spiritual health status, how do you rate your current general health status?” Participants answered with 5 levels of responses: excellent, very good, good, poor, and very poor. Students who answered good or above were considered as having “good health status,” and those who answered below good were considered as “poor health status.”
Attempted weight control
To evaluate attempted weight control, students were asked if they had attempted weight control of their own will in the last year. Participants responded with one of the following four options: tried to reduce weight, tried to maintain weight, tried to increase weight, or never tried to control weight.
Weight-control program attendance
Middle and high schools in Korea implemented the integrated obesity management program developed by the Ministry of Education, and adapted the program according to their individual school settings. Students who responded to the questionnaire answered ‘Yes’ or ‘No’ when queried on their participation in the weight-control program at school.
Improper weight control efforts
Improper weight control efforts are defined as behaviors that try to reduce or increase weight in the case of normal weight, and behaviors that try to maintain or increase weight in the case of overweight or obesity. Also, in the case of underweight individuals, improper weight control efforts include trying to lose weight or to maintain weight.
Dietary habits
Based on the dietary guidelines developed by the Ministry of Health and Welfare of Korea, and the Youth Risk Behavior Web-based Survey conducted by the Centers for Disease Control and Prevention of Korea [21], 5 unhealthy and 5 healthy dietary habits were selected to evaluate health-related dietary habits. The 5 unhealthy dietary habits include: 1) Eating meals or snacks using vending machines, 2) Eating while watching TV, 3) Eating alone, 4) Eating instant foods more than twice a week, and 5) Daily intake of junk foods such as soft drinks, hamburgers, and pizza. The 5 healthy dietary habits referred to the following habits: 1) Having breakfast regularly, 2) Eating milk or dairy foods every day, 3) Eating vegetables and fruits every day, 4) Eating sweet or salty food rarely, and 5) Eating less food for weight control. The subjects were asked to respond based on their behaviors in the past week, and answers reflected data for individuals who did or did not engage in such behavior.
Data analysis
Demographic characteristics of the study participants and the proportion of participants who attempted weight control were compared by considering the individual BMI, using t-tests. Differences in attempted weight control were analyzed by sex and BMI with χ2 or Fisher's exact test. To evaluate the relationship between BMI, and both health status and weight-control program attendance, we applied logistic regression models. Additionally, we investigated the effect of weight-control program attendance on improper weight-control efforts using logistic regression analysis. The relationships between weight-control program attendance and dietary habits were analyzed using multivariate logistic models after adjusting for age and sex. All data were analyzed using the SPSS software version 23.0 (Armonk, NY, USA), and R software version 3.5.1 in RStudio® version 1.1.456 (R Studio Inc., Boston, MA, USA). A P-value < 0.05 is considered statistically significant.
Go to :
RESULTS
Demographic characteristics of study participants
More than half the participants were female (53.8%) and high school students (54.2%). When categorized by obesity, most students were of normal weight (79.1%), followed by overweight (7.2%), underweight (6.9%) and obese (6.7%). Descriptive statistics for the 1,742 student participants enrolled in the study are provided in Table 1.
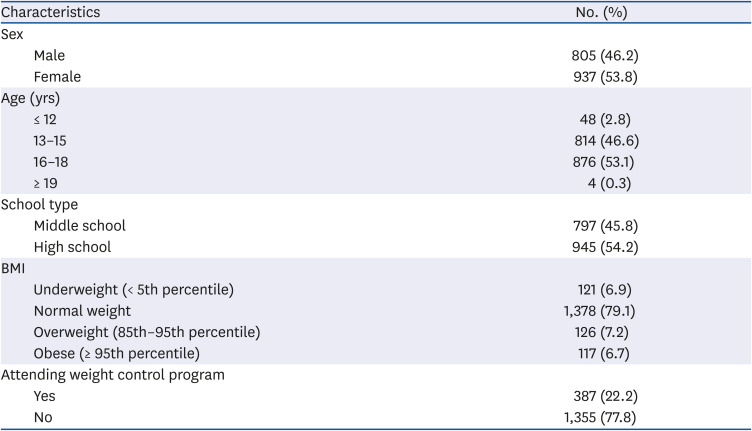
Table 1
Demographics of study participants (n = 1,742)
![]()
Attempted weight control by BMI status and sex
Among the students who did not try to control their weight, we observed a decreased percentage of respondents with increasing BMI: 32.2% responders in the underweight group, 30.8% in the normal weight group, 20.5% in the overweight group, and 14.5% in the obese group. Table 2 presents the relationships between attempted weight control, and both BMI status and sex. Compared with 15.7% participants in the underweight group who tried to lose weight, more than half the participants in the overweight and obese groups attempted losing weight (54.8% and 58.1%, respectively, Table 2). Nearly half the 766 female respondents in the normal weight group tried to lose weight, which was a significantly higher proportion than the male respondents (48.7% vs. 21.4%, respectively; P < 0.001).
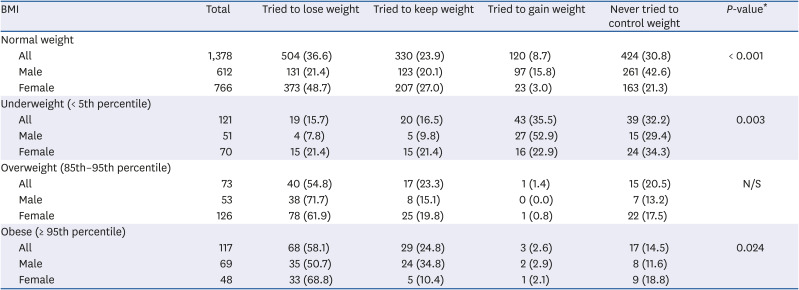
Table 2
Attempted weight control as per the BMI (kg/m2) status and sex
Values are presented as number (%).
BMI, body mass index; N/S, not significant.
*χ2 or Fisher's exact test was used to determine the P-values.
![]()
However, in the overweight and obese group, no significant difference was obtained between male and female respondents. In the underweight group, more female students attempted to lose weight as compared to male students (21.4% vs. 7.8%, respectively; P < 0.001), and fewer female students tried to gain weight compared to male students (22.9% vs. 52.9%, P = 0.003). No significant differences were found in the obese group between sexes.
Both BMI extremes coincide with health status dissatisfaction
As childhood obesity is influenced by physical and mental health, we examined whether students in each BMI category were dissatisfied with their physical, mental, social, and overall health (Table 3). Students with poor health status who responded poor or extremely poor on the questionnaire, were considered to be dissatisfied with their health status. Obese students were significantly more dissatisfied with physical (adjusted odds ratio [aOR] = 1.90; 95% confidence interval [CI] = 1.57–2.31; P < 0.001), mental (aOR = 1.77; 95% CI = 1.46–2.15; P < 0.001) and spiritual health (aOR = 2.03; 95% CI = 1.23–2.14; P = 0.001), as compared to students with normal weight. There was no significant difference between underweight and overweight students compared to normal weight students.

Table 3
Self-reported health status associated with BMI in multivariate logistic regression analysis*
aOR, adjusted odds ratio; 95% CI, 95% confidence interval; N/S, not significant.
*Adjusted for age and sex; †Poor health status includes the following responses: poor, very poor.
![]()
Relationship between weight-control program attendance with the BMI status and improper weight control efforts
Previous studies have shown that school-based weight-control program participants show favorable outcomes in terms of BMI. We therefore investigated this finding in our nationwide student population. Table 4 displays results of the logistic regression analysis examining the association between weight-control program attendance and BMI status.
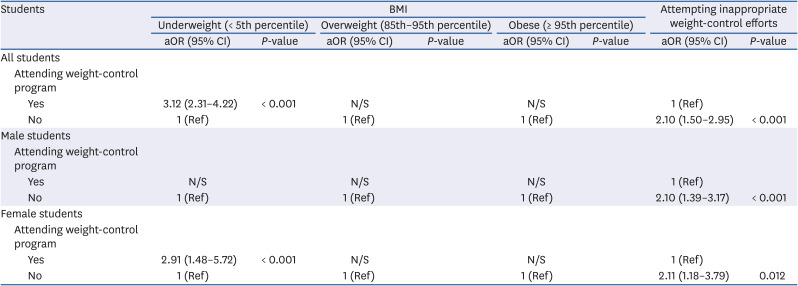
Table 4
BMI and improper weight-control efforts according to weight control program attendance in logistic regression analysis*
![]()
We found that compared to students who did not attend a weight-control program, students who attended the program were more likely to be underweight (aOR = 3.12; 95% CI= 2.31–4.22; P < 0.001). Moreover, examining this association separately in male and female students revealed that female students who attended a weight-control program were more likely to be underweight (aOR = 2.91; 95% CI = 1.48–5.72; P < 0.001), as compared to those who did not attend the program. However, no such significant difference was found in male students. Overall, students who did not attend the program were more likely to attempt improper weight control (aOR = 2.10; 95% CI = 1.50–2.95; P < 0.001), as compared to students who attended a weight-control program (Table 4). This significant relationship between weight-control program attendance and improper effort to control weight was also observed when evaluated separately in males (P < 0.001) and females (P = 0.012).
Relationship between weight-control program attendance and dietary habits
Table 5 details the association between weight-control program attendance and dietary habits. Unlike students who did not attend a weight-control program, students who attended the program were less likely to eat meals or snacks using vending machines (aOR = 1.54; 95% CI = 1.12–2.13; P = 0.008), eat instant foods more than twice a week (aOR = 1.61; 95% CI = 1.18–2.21; P = 0.003), or eat junk food daily (aOR = 1.99; 95% CI = 1.40–2.84; P < 0.001). Furthermore, students who participated in a weight-control program were more likely to consume milk or dairy foods daily (aOR = 1.42; 95% CI = 1.04–1.95; P = 0.027), and less likely to eat sweet or salty foods (aOR = 1.85; 95% CI = 1.33–2.57; P < 0.001).
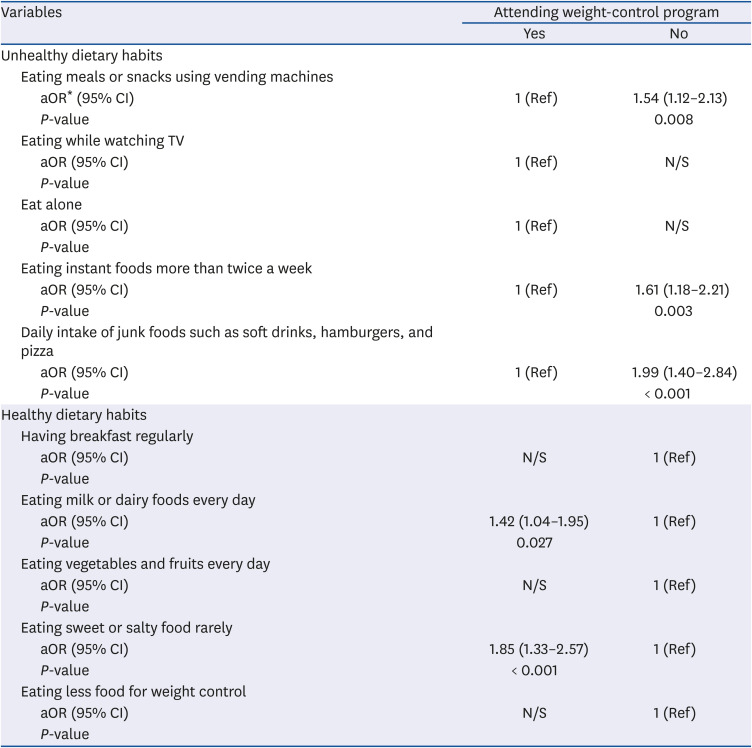
Table 5
Relationship between weight-control program attendance and dietary habits by multivariate logistic regression analysis
aOR, adjusted odds ratio; 95% CI, 95% confidence interval; N/S, not significant.
*Adjusted for age and sex.
![]()
Go to :
DISCUSSION
The current multi-institution survey undertaken by us provides evidence that participation in school-based weight-control programs is related to the student's inappropriate weight control efforts, dietary habits, and behavior. Students who did not participate in weight-control programs were likely to attempt inappropriate weight-control efforts. Additionally, students who attended the program were more likely to have healthy dietary habits, whereas those who did not attend were likely to have unhealthy eating habits. These results are consistent with previous studies [26303132], and indicate that participating in weight-control programs is related to not only inappropriate weight-control efforts, but also the behavior and dietary habits of the individual student.
Previous studies have thoroughly established that childhood obesity influences both the physical and mental health status [323334]. However, evidence for the effectiveness of school-based weight-control programs on weight-control awareness and eating habits is still limited. Other aspects of school-based weight-control program outcomes have been established, including progress toward ideal weight for students [263135] and improved student knowledge of nutrition [32]. Additionally, studies of dietary-habit modifications in response to school-based intervention programs have reported increased consumption of vegetables and fruits as well as selection of healthier foods [3036]. However, most of these studies did not include a nationally representative sample of secondary schools, and were simply tailored to school-specific circumstances. Since the association between participation in these programs, eating habits, and improper weight control attempts may differ depending on the situation of the school or characteristics of the students, a nationwide study population is necessary.
Our findings indicate that female adolescents who are underweight or normal tend to overestimate their weight status, as compared to their male adolescent counterparts. These results are comparable to a preceding study [37]. Previous studies have also reported a widespread distorted social perception that women are at their best when underweight, resulting in an increased socio-cultural pressure to participate in weight loss behaviors [3839]. Therefore, even if not required, many underweight female students attempt to lose weight inappropriately. Participation in an appropriate weight-control program was found to be significantly associated with attempting appropriate weight-control efforts, and was further linked to healthy eating habits and behaviors. These data indicate the need to educate adolescents, especially female students, to control their weight appropriately.
In the current study, the rate of attempting inappropriate weight-control efforts was higher in female students as compared to male students in all weight groups. Although we did not inquire about the specific weight control method, it is particularly important to maintain an appropriate weight during adolescence, since underweight, overweight, or obesity in childhood and adolescence negatively affects the lifelong health. An underweight adolescence increases the risk of infectious diseases [4041], whereas overweight or obesity in childhood has a high risk of affliction with obesity throughout life [6], increasing the risk of early onset of chronic diseases such as type 2 diabetes [4243], and negatively affecting educational achievement [44]. Additionally, since adolescents are more vulnerable to the media than adults, educating them on appropriate weight is essential for their protection [4546]. In other words, as the results of this study indicate, education on appropriate weight-control programs needs to be included in the school curriculum of adolescents.
This study has several limitations. First, due to the cross-sectional design of the study, our results demonstrate only associations and are unable to determine causation. However, this research provides meaningful nationwide data that includes school-specific differences. Second, there was considerable heterogeneity between the surveyed schools in terms of environment, program approach, and the program goal. Finally, this study did not include potential confounding factors, such as the surrounding environment and family-related factors.
In conclusion, attending school-based weight-control programs significantly relate to not attempting inappropriate weight-control efforts, and following healthy dietary habits. Since dietary habits and proper weight control efforts during childhood and adolescence impact the adulthood and lifelong health, inclusions of school-based weight-control programs are valuable to student health, and is anticipated to reduce public health burden in future.
Go to :
 XML Download
XML Download