

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Since December 2019, coronavirus disease 2019 (COVID-19) has spread worldwide, without decreasing trend. While 80% of COVID-19 patients have a mild clinical course,1 an unexpected increase in the number of deaths related to COVID-19 have resulted in an overwhelming medical burden in some areas. The ongoing pandemic has generated serious socioeconomic and healthcare problems due to the high mortality, especially in high-risk groups, and large number of patients in areas with limited medical resources. The overwhelming number of patients with COVID-19 infection combined with high-risk individuals for mortality makes it difficult to control the COVID-19 pandemic. Therefore, prediction of individualized risks for COVID-19 mortality is essential for estimating the severity of the clinical course of the disease. This would help in classifying the high-risk groups, which would help improve survival rates related with COVID-19.
COVID-19 mortality varies across countries ranging 1.4–4.3%, but the number of deaths due to COVID-19 is higher than that due to other respiratory viral infections, such as seasonal influenza.2345 The individualized prediction of COVID-19-related mortality is important for prioritizing patients with a high risk of mortality in terms of the allocation of limited medical resources.
Previous studies on the estimation of severity and mortality of COVID-19 showed diverse results, with the identification of a limited number of predictors, such as age and sex.678910 Age and underlying diseases are known factors associated with higher risks of mortality in patients with COVID-19,2671112 which is partially related with increased severity and susceptibility to COVID-19.1314 However, heterogeneity in age and underlying diseases could affect COVID-19-related mortality, and therefore, findings from previous studies were inconclusive.2689 In other studies, laboratory or radiologic findings were included in the factors predicting severity or mortality associated with COVID-19.1516171819 However, data on these factors are available for a limited number of COVID-19 patients in clinical settings and it takes time to obtain the results of laboratory and radiological examinations, thereby delaying the prediction of mortality and severity in patients with COVID-19.
In this study, we investigated the baseline characteristics of patients with COVID-19 and developed nomograms for predicting the probabilities of COVID-19-related mortality and 30-day and 60-day survival using data obtained at the time of admission, including individual's underlying diseases.
METHODS
Study population
The present study enrolled 5,626 confirmed cases of COVID-19 from the nationwide multicenter study between February 1 and April 30, 2020. During the study period, all confirmed cases of COVID-19 in South Korea were included since all patients were hospitalized regardless of their clinical presentation. Patients were followed-up until the end of their hospital stay. During the hospital stay, all patients were monitored by the Korea Disease Control & Prevention Agency of the National Medical Center; the database of information on patients with COVID-19 could be obtained from this agency. COVID-19 was confirmed via real-time reverse transcription-polymerase chain reaction assays using nasal and pharyngeal swab samples in accordance with the World Health Organization guidelines.2021 Data on baseline characteristics, such as age, sex, date of death, symptoms at the time of admission due to COVID-19, underlying diseases, and clinical severity were obtained retrospectively and anonymously under the leadership of the Central Disease Control Headquarters of South Korea. Height and weight of each patient were measured at the time of admission for treatment of COVID-19. Information on underlying diseases was collected by the doctors at the time of admission, by questioning the patients regarding the presence or history of any underlying disease.
Available items
Data on baseline characteristics, such as age, sex, height, and weight were obtained at the time of admission. Data on age were obtained in the form of age groups, using intervals of 10 years, but not individual age. Body mass index (BMI, kg/m2) were calculated using each patient' height and weight due to the significant effect of BMI on health outcome in patients with COVID-19.22 Clinical manifestations at the time of admission included fever, defined as a body temperature of > 37.5°C; cough; sputum; sore throat; rhinorrhea; myalgia; fatigue; dyspnea; headache; altered consciousness; vomiting/nausea; and diarrhea. Underlying diseases included diabetes mellitus (DM), hypertension, heart failure, cardiovascular diseases, asthma, chronic obstructive pulmonary disease (COPD), chronic kidney disease, cancer, chronic liver disease, rheumatoid/autoimmune disease, and dementia. The severity of COVID-19 was classified as mild, moderate, or severe as follows; mild, no interference with daily life or interference with daily life but no need for oxygen therapy during illness; moderate, requirement of oxygen via diverse routes (use of nasal cannula, oxygen mask, or non-invasive ventilator care); and severe, application of invasive ventilator care, multi-organ failure/ECMO use, or death.
Statistical analysis
Chi-square or Fisher's exact tests were performed to test the association between two nominal variables. Continuous variables were compared using the t-test or Welch t-test. The Mantel-Haenszel χ2 test was used to test the correlation between two ordinal variables or between dichotomous and ordinal variables.
From the total population, 4,426 patients were included in the prediction model after excluding 1,200 patients with any missing information on the variables. The mortality rate of the excluded patients was 9.42% (n = 113). Logistic regression analyses and a Cox proportional hazards models were used to construct a well-calibrated and discriminative nomogram for predicting mortality as well as 30-day and 60-day survival probabilities.
Cox proportional hazard equation applied in the present study was as follows:
S(t) = S0(t)exp(χβ)
χβ = 2.58 × age + 0.84 × sex + 0.67 × fever + 1.58 × dyspnea + 0.69 × DM + 0.82 × cancer + 1.49 × dementia
t = 30, S0(t) = 0.995
t = 60, S0(t) = 0.985
age = {0, <70 years1, ≥70 years, sex = {0, female1, male, fever = {0, no1, yes, dyspnea = {0, no1, yes, DM = {0, no1, yes, cancer = {0, no1, yes, dementia = {0, no1, yes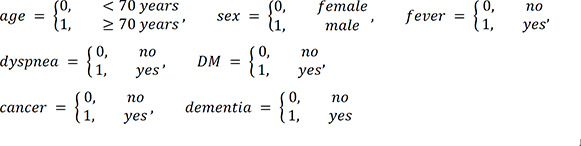
Logistic regression model applied in the present study was as follows:
χβ = −7.05 + 2.81 × age + 1.08 × sex + 0.97 × fever + 2.14 × dyspnea + 1.17 × DM + 1.38 × cancer + 2.12 × dementia
age = {0, <70 years1, ≥70 years, sex = {0, female1, male, fever = {0, no1, yes, dyspnea = {0, no1, yes, DM = {0, no1, yes, cancer = {0, no1, yes, dementia = {0, no1, yes
To validate the models, the total population was randomized into the train and test sets at a ratio of 7:3. The balance between the two sets was checked using through the χ2 test, and no significant differences were observed in all variables. To construct the logistic regression model, we obtained crude odds ratios (ORs) via univariate logistic regression analysis of the train set. We constructed a multivariate logistic model by including variables with P values < 0.2 in the univariate analysis and those with the lowest Akaike information criterion using the backward stepwise approach.23 Finally, we obtained the final prediction model after extracting insignificant variables. The validation of the logistic regression model was checked by the calibration curve and area under the curve (AUC) in the test set. The same approach was used for the construction of a Cox proportional hazards model. The validation of the Cox proportional hazards model was checked using Harrell's C-index, time dependent AUCs, and calibration curves. The constructed models can be used on the web-based risk calculator (https://koreastat.shinyapps.io/RiskofCOVID19/).
Overall, statistical analyses were performed using the R programming language and environment version 4.0.2 (R Foundation for Statistical Computing, Vienna, Austria). P values < 0.05 was considered statistically significant.
RESULTS
Baseline characteristics of the study population
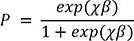
The present study included 5,626 confirmed COVID-19 cases. Table 1 describes the baseline characteristics of the study population: 2,319 (41.22%) patients were male; 15.45% patients were older than 70 years, and 33.47% patients had at least one underlying disease. With respect to underlying diseases, the prevalence of hypertension was the highest (21.35%), followed by that of DM (12.28%) and dementia (3.98%). The mortality rate of COVID-19 was 4.27% in this study.
Table 1
Baseline characteristics of the study population
Values are presented as number (%).
COVID-19 = coronavirus disease 2019, SD = standard deviation, ECMO = extracorporeal membrane oxygenation, DM = diabetes mellitus, COPD = chronic obstructive pulmonary disease.
aMultiple responses.
![]()
Symptoms at the time of COVID-19 diagnosis
The most common symptom of COVID-19 was cough (22.60%) in all age groups, followed by sputum (15.63%), except among those in the 0–9 years group (Supplementary Table 1). Fever was more common in children (18.84% in the 0–9 years group vs. 13.26%–15.64% in other groups), whereas dyspnea was more common in the elderly, especially in those older than 70 years (14.42% in the older than 70 years group vs. 1.45–8.09% in other groups).
Severity of COVID-19 according to underlying diseases
The prevalence of severe COVID-19 was the highest in patients with dementia (33.93%), followed by those with heart failure (33.90%) and chronic kidney disease (32.73%) (Supplementary Table 2). Similar to the prevalence of severe COVID-19, COVID-19-related mortality was the highest in patients with dementia (33.48%) (Supplementary Table 3).
Severity of COVID-19 according to age and sex
There was linear correlation between age and COVID-19 severity (Supplementary Table 4). The prevalence of severe COVID-19 was the highest in elderly people, especially those aged over 70 years.
Prevalence of underlying diseases according to age groups
The prevalence of some underlying diseases, such as hypertension, dementia, and cancer, was the highest in individuals older than 70 years (Supplementary Table 5), whereas that of rheumatoid or autoimmune diseases was the highest in patients aged 50–59 years.
Factors associated with COVID-19-related mortality
To identify potential factors that could predict COVID-19-related mortality, univariate and multivariate logistic regression analyses were performed, as indicated in Table 2. The following factors showed significant associations with COVID-19-related mortality: age ≥ 70 years; male; the presence of fever and dyspnea at the time of diagnosis; and underlying diseases such as DM, cancer, and dementia. The same predictive factors were identified in the final Cox proportional hazard model for 30-day and 60-day survival in patients with COVID-19 (Table 3).
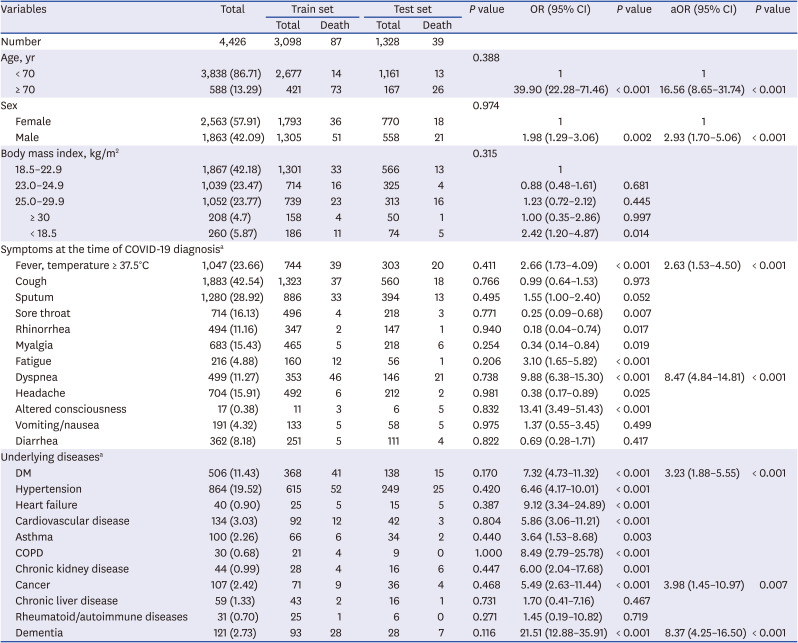
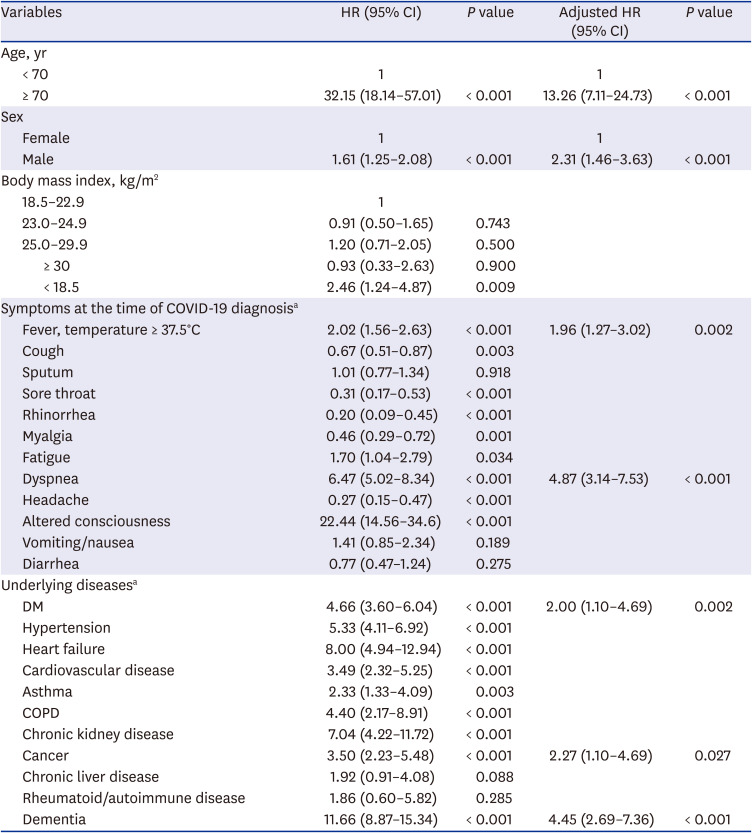
Table 2
ORs for factors associated with COVID-19-related mortality
COVID-19 = coronavirus disease 2019, OR = odds ratio, CI = confidence interval, aOR = adjusted odds ratio, DM = diabetes mellitus, COPD = chronic obstructive pulmonary disease.
aMultiple responses.
![]()
Table 3
Hazard ratios for factors associated with coronavirus disease 2019-related mortality
HR = hazard ratio, CI = confidence interval, DM = diabetes mellitus, COPD = chronic obstructive pulmonary disease.
aMultiple responses
![]()
Construction of a nomogram for predicting mortality in patients with COVID-19
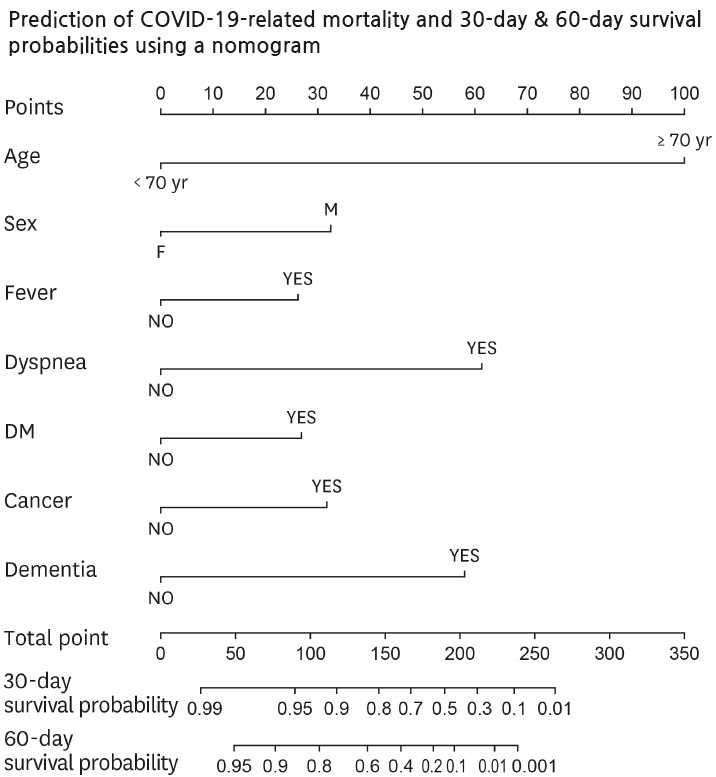
To identify high-risk patients, we constructed a predictive nomogram for mortality due to COVID-19 (Fig. 1). Points were assigned to patients based on age, sex, presence of specific symptoms including fever and dyspnea at the time of diagnosis of COVID-19, and the presence of specific underlying diseases (DM, cancer, and dementia), with a vertical line to the “Points” scale at the top of the nomogram (Fig. 1A). The actual and predicted mortalities due to COVID-19 were similar, and the calibration plot showed a mean absolute error of 0.006 (Fig. 1B), suggesting that the model was acceptable. Fig. 1C shows that the under the receiver operating curve (ROC) for COVID-19-related mortality was 0.926.
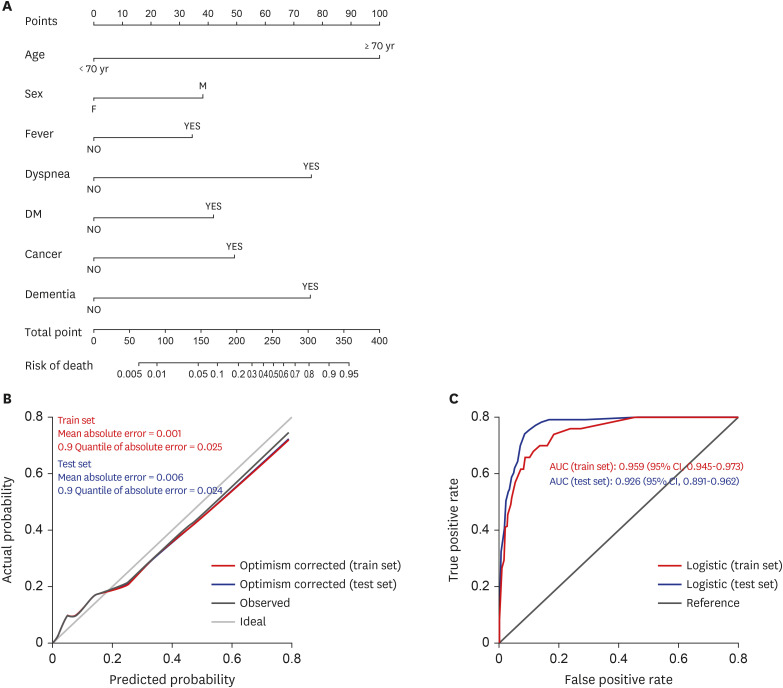
Fig. 1
Prediction of mortality in COVID-19 patients. (A) Nomogram for predicting mortality in patients with COVID-19. (B) Calibration plot of the actual and predicted probabilities in the train and test sets. (C) AUC of the nomogram is 0.959 (95% CI, 0.945–0.973) in the train set and 0.926 (95% CI, 0.891–0.962) in the test set.
COVID-19 = coronavirus disease 2019, AUC = the area under the curve, CI = confidence interval, DM = diabetes mellitus.
![]()
Construction of a nomogram to predict the 30-day and 60-day survival probabilities in patients with COVID-19
We constructed a predictive nomogram for 30-day and 60-day survival in patients with COVID-19 (Fig. 2A), including the same prognostic factors as those used in the model for COVID-19-related mortality. The nomogram demonstrated good accuracy for predicting 30-day and 60-day survival probabilities in patients with COVID-19 with a C-index of 0.906 (95% confidence interval, 0.883-0.929). Calibration curves indicated that there was no apparent shift from the perfect fit, with a good correlation between the predicted and observed values in the study population (Fig. 2B and C). The AUCs for 30-day and 60-day survival probability in patients with COVID-19 in the train set were 0.914 and 0.954, respectively (Fig. 2D and E). In the test set, the AUC for mortality was 0.926 (Fig. 1) and AUCs for 30-day and 60-day survival were 0.876 and 0.660, respectively (Fig. 2).
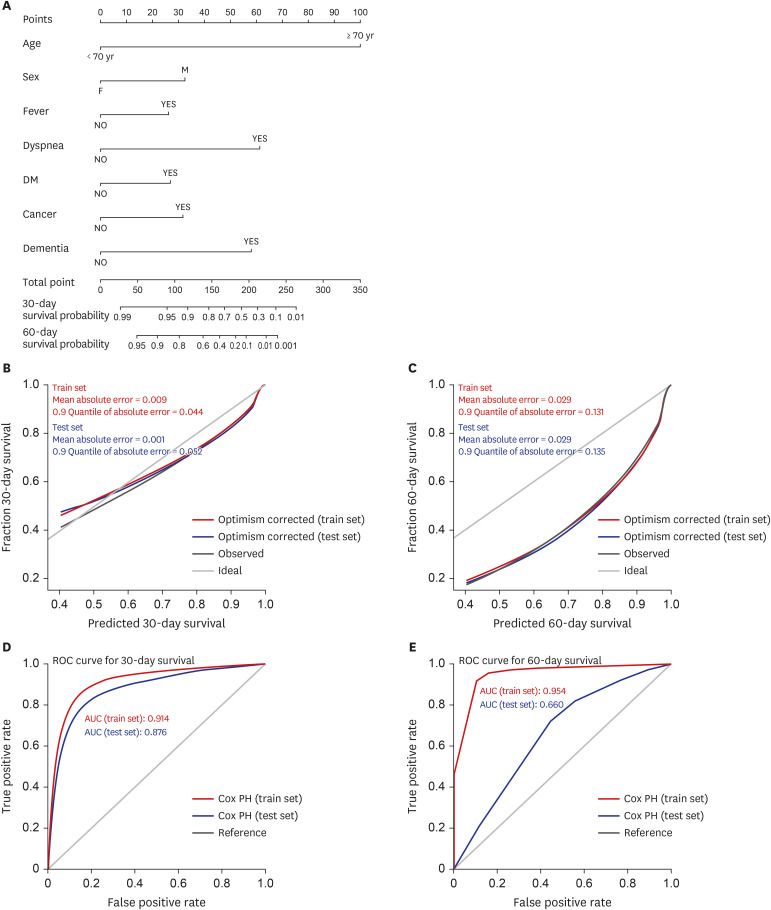
Fig. 2
Prediction of the 30-day and 60-day survival probabilities in COVID-19 patients. (A) Nomogram predicting the 30-day and 60-day survival probabilities in patients with COVID-19 in the train and test sets. Calibration plot of the actual and predicted probabilities for 30-day (B) and 60-day (C) survival in the train and test sets. The AUCs of the nomogram for predicting 30-day survival (D) and 60-day survival (E) in the train and test sets. DM = diabetes mellitus, ROC = receiver operating curve, AUC = area under the curve, COVID-19 = coronavirus disease 2019.
![]()
DISCUSSION
Even after a year post the emergence of COVID-19, severe cases of COVID-19 have caused socioeconomic and medical problems due to high mortality, especially in limited medical resource settings. Therefore, prediction of mortality early in the clinical course is essential in COVID-19 patients to stratify patients requiring intensive monitoring and aggressive therapy, thereby improving clinical outcomes. In the present study, we identified the predictive factors of COVID-19-related mortality using a nomogram that was validated using calibration plots and ROC curves. The prognostic factors included age ≥ 70 years; male sex; presence of fever and dyspnea at the time of COVID-19 diagnosis; and DM, cancer, and dementia as underlying diseases; these factors can be easily evaluated in the early phase of diagnosis without any additional tests. In addition, we investigated the factors associated with 30-day and 60-day survival in patients with COVID-19; the same prognostic factors were identified. Our findings can help guide policy makers on medical resource allocation in the uncontrolled COVID-19 epidemic era, thereby, improving public health outcomes. Our results would be more useful even in medium- or low- income countries with limited resources for diagnostic purposes.
Although various scoring systems can predict COVID-19-related mortality, we used a nomogram with calibration and discrimination for validation in this study, thereby enabling individualized and evidence-based risk estimation. Previous studies have suggested nomograms for predicting the risk of severe COVID-19 and COVID-19-related mortality using diverse laboratory findings, clinical features, and chest computed tomography (CT) findings.15161718192425 In the present study, we considered age, sex, body mass index, symptoms at the time of COVID-19 diagnosis, and underlying diseases for the prediction model as these parameters can be obtained in the early clinical course. This can be very helpful for identifying patients at risk of mortality at the time of COVID-19 diagnosis. In addition, the AUC for the prediction for COVID-19-related mortality in the present study was the highest compared to those in other previous studies, except for one that included chest CT findings as a predictive factor for severe COVID-19 (Supplementary Table 6). Significant laboratory markers, such as C-reactive protein, could be helpful for predicting the clinical course and outcomes of COVID-19 by reflecting the degree of inflammation.19 However, we did not include laboratory findings or imaging results as a limited number of patients underwent laboratory and imaging examinations in our study. Thus, our prediction model can be easily applied to predict the mortality of COVID-19 even in low- and middle-income countries.
Older age is known as a risk factor of COVID-19-related mortality, although the cut-off differs according to study populations.7826272829 Older age was identified to be a risk factor of a severe clinical course in other infections, including severe acute respiratory syndrome (SARS) and Middle East respiratory syndrome (MERS).3031 Similarly, in COVID-19, age was an independent prognostic factor for mortality and 30-day and 60-day survival. Older age can affect the clinical course of COVID-19 and COVID-19-related mortality, possibly through immunosenescence or a high prevalence of multiple underlying diseases.
Studies on the association of underlying disease with the severity and mortality of COVID-19 included various combinations of diseases, and therefore, these studies reported different results.3 Nevertheless, several underlying diseases, such as cancer, hypertension, and cardiovascular diseases, act as risk factors for severe COVID-19 or COVID-19-related mortality.21232 In COVID-19 patients with cancer, systemic immunosuppression associated with the cancer itself or anticancer therapy might affect the vulnerability to severe COVID-19 or COVID-19-related mortality, which is consistent with our findings. Diabetes, known to be a hazardous comorbidity in fatal COVID-19 cases, was also associated with COVID-19-related mortality in the present study. Although the reasons underlying this association have not been identified,2 persistent chronic inflammation in diabetes combined with poor control of blood glucose levels during the COVID-19 illness and combined comorbidities of diabetes in itself can affect the prognosis of COVID-19 in patients with diabetes.33 Some studies showed that patients with dementia, especially those living in care facilities, had an increased risk of COVID-19 and COVID-19-related mortality,343536 consistent with our findings. Living in care facilities favors the rapid spread of COVID-19 due to the increased likelihood of exposure to the virus in a closed environment, and furthermore, patients with dementia tend to have other underlying comorbidities. A meta-analysis of the association of underlying conditions with COVID-19-related mortality showed that previous studies on this topic included a limited number of underlying diseases and had limited sample sizes.2 In contrast, the present study included diverse underlying disease and used a nationwide registry of COVID-19 patients.
In the present study, the AUC for COVID19-related 30-day survival was excellent, whereas that for COVID-19-related 60-day survival was poor in the test set. These results might suggest that the prediction model based on age, sex, symptoms at the time of COVID-19 diagnosis, and underlying diseases would be appropriate for the prediction of COVID-19-related short-term survival. However, more delicate variables, reflecting clinical courses and laboratory findings, might be needed for better prediction of COVID-19-related long-term survival.
There are some limitations to our study. The sample size was considered to be limited because the study population was enrolled in the early period of the pandemic. However, previous studies on the prediction of COVID-19-related mortality/severity included smaller samples than that in our study (Supplementary Table 6).151617182537383940 Since the appropriate therapeutic strategies had not been established during the early epidemic of COVID-19, the mortality in the present study was less affected by medications, including anti-viral agents, that can affect the clinical course of COVID-19. The present study included patients from care hospitals where patients with dementia were hospitalized. The prevalence of dementia differs across study populations. One study reported a 7.5% prevalence,22 while some studies did not include dementia as one of the comorbidities of COVID-19.2 Since comorbidities are affected by herd infections in specific institutions, consideration of the specific situations on mass infection is needed while interpreting the results of related studies. Although AUCs for COVID19-related 30-day and 60-day survival in the train set were excellent, AUC for 60-day survival in the test set showed poor accuracy. Although we performed internal validation by classifying the total population into the train and test sets, external validation of the results is also needed to confirm our results. The variants of SARS-CoV-2 and COVID-19 vaccination status were not considered in the prediction model in the present study due to availability of limited information at the time of data collection. The prediction models for COVID-19-related mortality considering these factors can be developed after accumulation of sufficient information in the near future. The treatment strategies and clinical courses of COVID-19 prediction model were not included in the prediction model in the present study due to limitations in the available database. However, the results of the present study would be useful in predicting COVID-19-related mortality and in more efficient allocation of medical resources at an earlier stage. Finally, the present study was performed retrospectively, and therefore, validation using a prospective design is required to improve the statistical power of the results.
In conclusion, age ≥ 70 years, male sex, the presence of fever and dyspnea at the time of COVID-19 diagnosis, and DM, cancer, and dementia as underlying diseases are associated with an increased risk of COVID-19-related mortality, and these factors can be used for the prediction of 30-day and 60-day survival in COVID-19 patients. The results of the present study would be helpful in establishing therapeutic strategies for improving the clinical outcomes and guiding policy makers with regard to appropriate medical resource allocation.
 XML Download
XML Download