

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Osteoporosis and osteoporotic fractures in an aging society are socioeconomic health issues.1 Anti-osteoporosis medications help to prevent the occurrence of fractures and complications. Moreover, multidisciplinary approaches to early functional recovery after osteoporotic fractures, particularly hip fractures, can reduce the socioeconomic costs.2
The four major osteoporotic fractures include distal radius fracture, proximal humerus fracture, vertebral fracture, and hip fracture. The characteristics of each fracture and the severity of complications are different.3 Hip fractures cause significant bleeding and increase morbidity and mortality.4 Spine fractures occur repeatedly and cause kyphotic deformities.5 Proximal humerus fractures are quite functional after union, despite residual angular deformity, because of the large range of motion of the shoulder.6 Ulnar-plus deformity and dorsal angulation after distal radius fracture reduce patient satisfaction after treatment.7 Older patients have also many underlying diseases, which hamper recovery after fracture. Consequently, patients' quality of life is decreased, their dependence on others is increased, and chronic pain increases mental stress.8 In the study of Jang et al.,910 differences in the duration of the increase in the risk of suicide death after fracture were observed due to differences in characteristics between vertebral fractures and hip fractures and combinations of these factors. Therefore, the risk of suicidal death among older individuals associated with the different types of osteoporotic fractures is thought to differ. Also, to the best of our knowledge, no studies have evaluated suicide death related to upper limb osteoporotic fractures, and no studies have analyzed suicide deaths related to these four fractures in one model.
The purpose of our study was to investigate the incidence rate of suicide in elderly patients with osteoporotic fractures in a nested case-control model, based on nationwide cohort data, and to analyze the change in the risk of suicide death over time after each osteoporotic fracture, in comparison with controls.
Go to : 
METHODS
We used the National Health Insurance Service-Senior cohort (NHIS-Senior) of South Korea. The NHIS establishes claim databases for research purposes, which store all records of healthcare and long-term care services.1112 The NHIS-Senior consists of data from 558,147 people selected by a 10% simple random sampling of 5.5 million participants aged 60 years or over, in 2002.12 Under a compulsory social insurance system legislated by the National Health Insurance Act, all participants could be followed up until 2015, except for instances of death or emigration.13 The key variables in the NHIS-Senior cohort include all inpatient and outpatient medical claims data, such as codes for treatment procedures, prescriptions, and diagnoses.
Case and control selection criteria
As South Korean law requires all death certificates to be reported to Statistics Korea, information on death (date and cause) was collected from this agency and individually linked using unique personal identification numbers.12 Among the NHIS-Senior cohort, suicide cases were identified as those whose deaths were categorized as “Intentional Self-Harm,” International Statistical Classification of Diseases and Related Health Problems, 10th Revision (ICD-10) codes X60 to X84. The time of the event (index date) was defined as the date of death by suicide.
Case and control patients were matched based on sex and age at the index date. Controls were randomly selected at a 1:5 ratio from the set of individuals who were at risk of becoming case patients at the time when suicide cases were selected. Individuals excluded during patient selection were also excluded from the risk set.
Osteoporotic fractures
Considering previous studies, newly developed osteoporotic fracture patients were identified from the NHIS-Senior cohort from 2003 to 2015.141516171819 Each indicator variable corresponding to the four major types of osteoporotic fractures was defined as follows.
Incident hip fracture
First admission to an acute care hospital with ICD-10 diagnostic codes S720 (femoral neck fracture) or S721 (intertrochanteric fracture), and recipients of typical related surgeries, including internal fixation, hemiarthroplasty, or total arthroplasty.16
Incident vertebral fracture
First admission to an acute care hospital with ICD-10 codes S22.0 (fracture of the thoracic spine), S22.1 (multiple fractures of the thoracic spine), S32.0 (fracture of the lumbar spine), M48.4 (vertebral fatigue fracture), and M48.5 (collapsed vertebra, not elsewhere classified), and recipients of typical procedures, including vertebroplasty, kyphoplasty, or instrumentation.17
Incident proximal humerus fracture
First admission to an acute care hospital or first outpatient visit with ICD-10 codes S422 (fracture of the upper end of the radius), or S423 (fracture of the humeral shaft), and recipients of typical procedures, including open reduction, closed pinning, external fixation, hemiarthroplasty, total shoulder arthroplasty, shoulder spica, or velpeau cast.18
Incident distal radius fracture
First admission to an acute care hospital or first outpatient visit with ICD-10 codes S526 (fracture of the lower end of the radius), or S526 (fracture of the lower end of both the ulna and the radius), and recipients of typical procedures, including open reduction, closed pinning, external fixation, closed reduction, long arm splint, or long arm cast.19
Fracture patients whose first fracture developed in 2002 were excluded in order to select incident fracture patients. Patients under the Medical Aid program were also excluded to eliminate the possibility of incomplete information.
Statistical analyses
The incidence rates of suicide and 95% confidence intervals (CIs) among osteoporotic fracture patients were calculated using a generalized linear model with a Poisson distribution and were presented as the number of suicides per 100,000 person-years. Conditional logistic regression analysis was performed to evaluate the association between each type of osteoporotic fracture and the risk of suicide death. All four types of fracture indicator variables were simultaneously included in the model. Adjusted odds ratios (aORs) and 95% CIs were estimated. In addition to matching variables for the nested case–control study design, we adjusted for the following confounders: past medication history (anti-hypertensive agents, antidiabetic agents, lipid-lowering agents, steroids, benzodiazepines, opioids, anti-rheumatic agents, non-steroidal anti-inflammatory agents [NSAIDs]), COX-2 inhibitors, antiplatelet agents, anti-Parkinson medications, anti-Alzheimer medications, aspirin, anti-epileptic drugs, warfarin, anti-psychotic drugs), past medical history (neoplasm, ischemic heart disease, stroke, chronic kidney disease, depression), Charlson Comorbidity Index (CCI), household income level, registered disability, residential area, calendar year of suicide, and number of outpatient visits. For each subject, the number of comorbidities was assessed by diagnostic codes during the 3 years before the index date using Quan's ICD-10 coding algorithm of the CCI score.20 The presence of CCI disease-constituting categories was defined by at least two outpatient visits or one admission upon the primary or first secondary diagnosis. A history of depression was defined as the presence of a diagnostic code for depression or any prescription of antidepressants within 1 year. Opioid medication history was categorized by prescription days. Prescription of other medications for more than 28 days was used to define patients who had taken corresponding medications.
Statistical significance was set at P < 0.05. All statistical analyses were conducted using SAS Enterprise Guide version 7.1 (SAS Institute, Cary, NC, USA).
Ethics statement
The design and protocol of this study were approved by the Institutional Review Board in Daejeon Eulji Medical Center (IRB No. EMC 2020-08-018-001). Written informed consent was waived due to the nature of retrospective study.
Go to :
RESULTS
We identified 19,915 patients with hip fracture, 23,473 patients with radius fracture, 2,299 patients with humerus fracture, and 21,096 patients with spine fracture from 2003 to 2015 among individuals aged over 60 years (Table 1). The incidence rate of suicide death in elderly patients with hip fracture was 120.7/100,000 person-years (95% CI, 97.8–149). This was the highest rate among the four types of fractures during the entire follow-up period. In particular, the incidence rate of suicide death was the highest, at 217.5/100,000 person-years (95% CI, 157.6–300.3), within 1 year of hip fracture. The incidence rates of suicide deaths were 181.5/100,000 person-years (95% CI, 130.3–252.8) in cases with spine fracture, 142.9/100,000 person-years (95% CI, 46.1–442.9) in those with humerus fracture, and 71.2/100,000 person-years (95% CI, 43.6–116.1) in those with radius fractures. For all other fractures except radial fractures, the incidence rate of suicide death decreased over time.
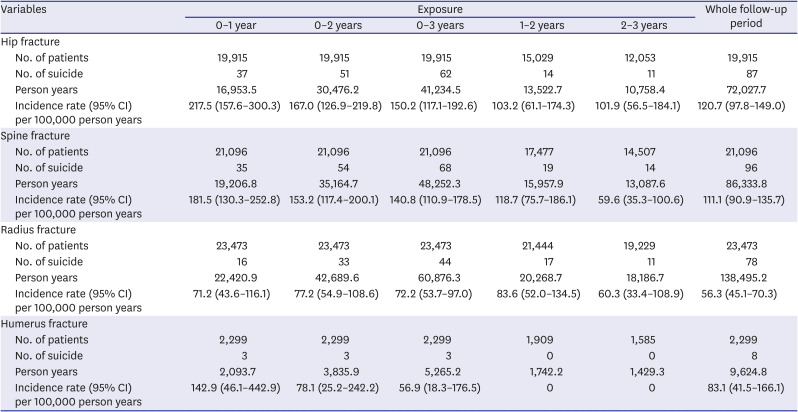
Table 1
Incidence rates of suicide in elderly patients with each fracture
![]()
In the NHIS-Senior cohort, 3,070 suicide cases and 15,350 controls were identified (Table 2). The two groups showed even distributions in the matched variables, including age, sex, and calendar year. Patients in suicide cases were more frequently admitted to hospital (odds ratio [OR] = 3.74; 95% CI, 3.44–4.07) and visited outpatient visits more often than the controls (OR = 1.33; 95% CI, 1.28–1.37). Patients in suicide cases were more frequently exposed to opioids (OR = 1.66; 95% CI, 1.51–1.82), benzodiazepines (OR = 2.34; 95% CI, 2.14–2.56), and NSAIDs (OR = 1.46; 95% CI, 1.51–1.82) than were controls. In addition, patients in suicide cases more often had a history of depression (OR = 3.4; 95% CI, 2.94–3.94) and neoplasms (OR = 2.1; 95% CI, 1.81–2.44) than did controls.
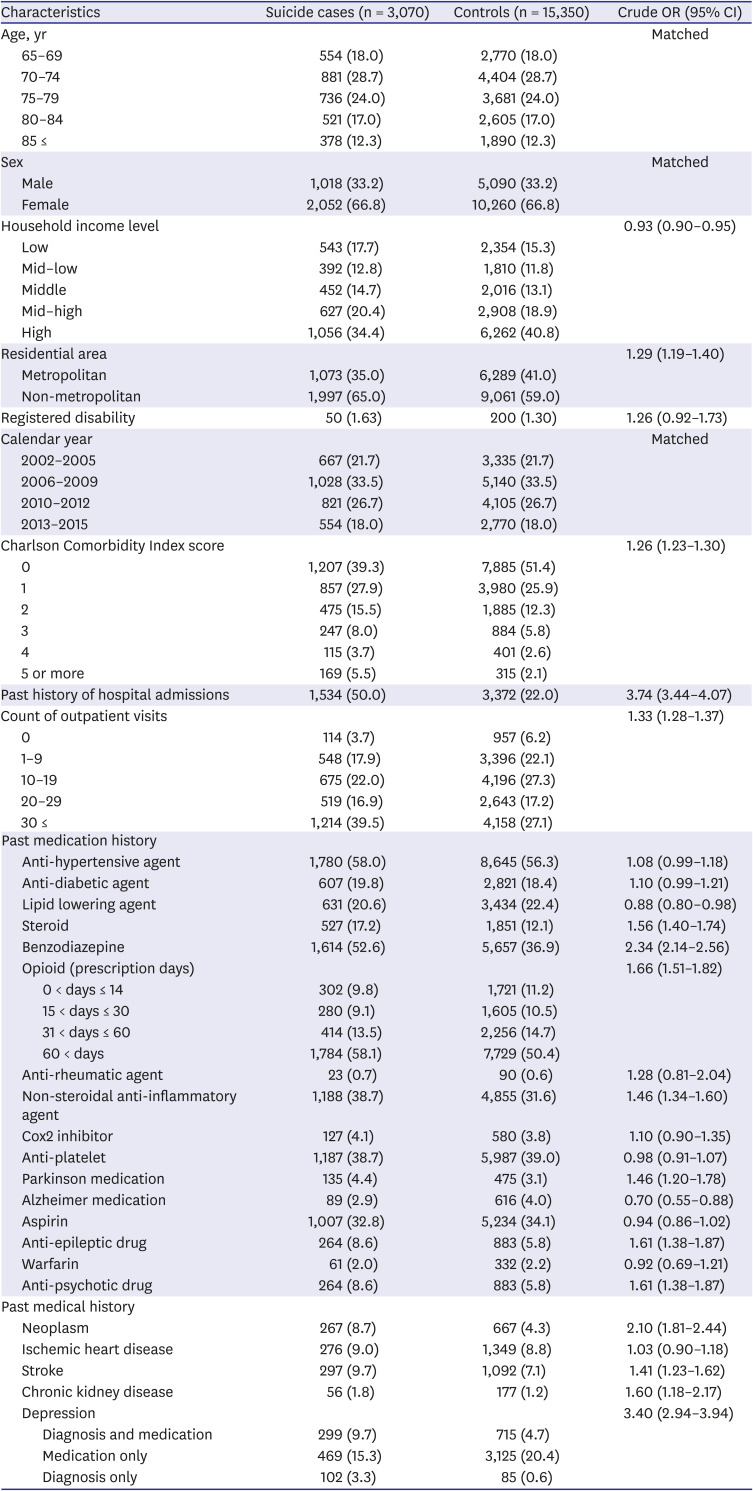
Table 2
Baseline characteristics of suicide cases and controls
![]()
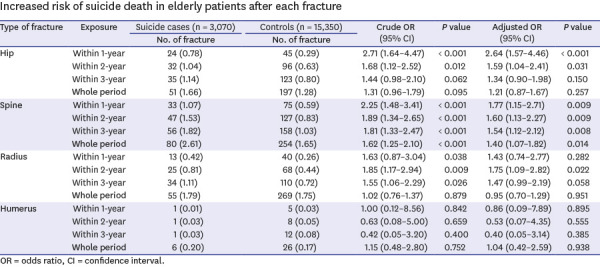
Table 3 shows the relationship between each fracture type and the risk of suicide deaths among elderly patients. Patients with incident hip fracture showed an increased risk of suicide death within 1 year after fracture (aOR = 2.64; 95% CI, 1.57–4.46; P < 0.001) compared to controls. However, the increased risk of suicide death in patients with hip fracture lasted only up to 2 years (aOR = 1.59; 95% CI, 1.04–2.41; P = 0.031). Spine fracture increased the risk of suicide deaths for all observation periods. On the other hand, there was no evidence that humerus fracture increased the risk of suicide death at any time during the observational period (P > 0.05). Radius fracture did not increase the risk of suicide death within 1 year of fracture (aOR = 1.43; 95% CI, 0.74–2.77; P = 0.282), but increased the risk of suicide death within 2 years of fracture. Although marginally statistically significant (aOR = 1.47; 95% CI, 0.99–2.19; P = 0.058), an increased risk of suicide death was observed within 3 years of a radial fracture.
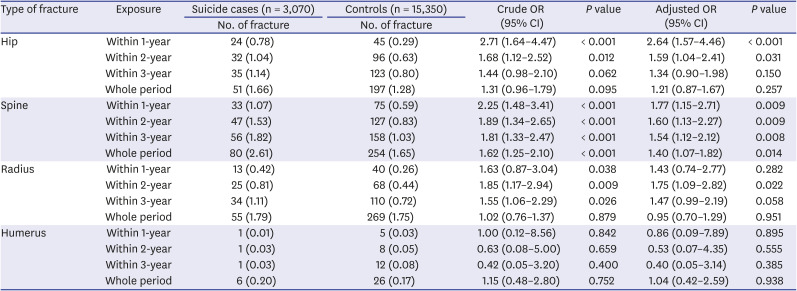
Table 3
Increased risk of suicide death in elderly patients after each fracture
![]()
Go to :
DISCUSSION
The main findings of this study are as follows. First, the incidence rate of suicide death in elderly patients with hip fracture was 217.5/100,000 person-years, that in those with spine fracture was 181.5/100,000 person-years, that in those with humerus fracture was 142.9/100,000 person-years, and that in those with radius fracture was 71.2/100,000 person-years, within 1 year of the respective fractures. Second, the risk of suicide death in elderly patients after each fracture over time was different for each fracture. The risk of suicide death was increased by 1.59 times within 2 years after hip fracture and by 1.4 times during the whole follow-up period after spine fracture. However, humerus fractures did not increase the risk of suicidal deaths. Moreover, although radius fracture did not increase the risk of suicide death within 1 year of surgery, it increased the risk of suicide death by 1.75-fold within 2 years of the fracture.
Suicide in the elderly population is an important health issue in developed countries.21 Several studies have reported that suicide rates among older people in many countries are high.22 Various factors, such as physical disease, chronic pain, disability, dependency, and high treatment cost are associated with suicide in elderly individuals.23 They often have reduced emotional expression, making it difficult to notice risk of suicide attempt.24 In previous studies, the incidence rates of suicide death in elderly patients were 266.1/100,000 person-years within 1 year of hip fracture and 156/100,000 person-years within 1 year of spine fracture.10 The incidence rates of suicide death observed in this study were 217.5/100,000 person-years for hip fracture and 181.5/100,000 person-years for spine fracture, within 1 year of fracture. The slight difference between our results and those of previous studies may be due to differences in inclusion criteria, such as follow-up period and diagnostic code. The age-standardized suicide rate for those 70–79 years old in Korea in 2016 was 90.32 and 26.50/100,000 men and women, respectively.25 In patients with congestive heart failure and acute myocardial infarction, the suicide mortality rates were 59.6 and 44.6/per 100,000 person-years, respectively. Although there are differences depending on the type of cancer, and the economic, cultural, and religious characteristics of each country, the incidences rate of suicide death of cancer patients are 6.1–88.7/100,000 person-years.26 Compared to the results of the above studies, the incidence rates of humerus fracture and radius fracture reported in the present study are not considered to be high, except for the incidence rate of suicide death within 1 year of humerus fracture.
Changes in the risk of suicide death associated with osteoporotic fractures over time seem to reflect the characteristics of each fracture. Mortality rates in elderly patients with hip fracture are 20–37% at 1 year and 69.4% at 5 years after fracture.9 Since a large number of older hip fracture patients die within a short period after fracture, long-term surviving patients are likely to be those with good health or function, and it is considered that suicide risk increases only within 2 years. In contrast, the risk of suicide death increases during the entire follow-up period for spine fractures, given the characteristics of this type of fracture, which occurs repeatedly in multiple vertebral bodies.10 It has been reported that the treatment of humerus fracture is expensive, but compared to hip or spine fracture, the treatment cost is lower, and conservative treatment is a reasonable treatment option.27 In addition, even if angular deformity remains after treatment, the range motion of the shoulder is large, so that the functional results are quite good. This may underlie the lack of increased suicide risk after humerus fractures during the follow-up period in this study. Interestingly, in radial fractures, the risk of suicide death did not increase at 1 year after fracture, but a statistically significant increase in the risk of suicide death was observed within 2 years, and a marginally significant increase in risk was observed within 3 years after the fracture. Upper extremity fracture accompanied by hip fracture did not increase in-hospital mortality.28 In addition, such patients had higher functional capacity and were more independent before fracture. It has been reported that both non-surgical and surgical treatments, according to appropriate indications, show good results.29 However, distal radius fractures increased not only the risk of subsequent falls but also the risk of subsequent fracture.30 Therefore, it is thought that a rather late increase in the risk of suicide death after distal radius fracture is due to stress and loss of function because of the occurrence of subsequent fractures.
Our study had several limitations. First, diagnostic codes of the inclusion criteria may not represent the actual status of a patient's injury, which is a fundamental limitation of the insurance database. However, the incidence of osteoporotic fracture could be ascertained well, because almost all hospitals follow the fee-for-service system, and all surgical and treatment procedure costs are claimed. Despite the above mentioned drawback, the NHIS-Senior cohort has a large sample size with a very low follow-up loss rate over 13 years due to the nature of the national administration data. Additionally, the NHIS-Senior represents the entire population over 60 years of age in South Korea. Thus, it represents all elderly patients in South Korea. Second, since this study was based solely on the South Korean database, it is possible that regional, cultural, and religious biases were present. However, this study compared the risk of suicide deaths between osteoporotic fracture patients and their controls. Moreover, the association between severe injuries and the risk of suicide may not differ considerably among various cultural backgrounds. Therefore, we believe that the results of this study may be generalizable to other populations. Fourth, there was insufficient consideration of potential confounders, such as the presence of a spouse, that could increase the risk of suicidal death.
In conclusion, there were noticeable differences in both degree and duration of increased suicide risks depending on the type of osteoporotic fracture. These differences are thought to be due to variable characteristics of each fracture. Our findings show that mental stress and suicide risk in elderly patients after osteoporotic fracture should be assessed differently depending on the types of fracture.
Go to :
 XML Download
XML Download