

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Sepsis is a life-threatening condition characterized by bacteremia and clinical signs of systemic infection.1 Preterm infants are prone to sepsis owing to their immature innate immunity and prolonged hospitalization.2 Over 20% of very low birth weight infants (VLBWIs) are diagnosed with late-onset sepsis (LOS).2 A stronger inflammatory response is associated with LOS than with early-onset sepsis, which is vertically transmitted.3 Some studies using preclinical models have suggested that perinatal sepsis induces alterations in the developing brain since it impacts neuronal migration, gliogenesis, and myelinogenesis, which occur at a late gestational age and is predominant in the first 2 weeks of postnatal life.45 Together, these factors may result in white matter injury and diffuse injuries to premyelinating oligodendrocytes, which have been shown to be closely associated with an increased risk of impaired cognitive and motor functions.6 Although several studies have been conducted on the neurodevelopmental impact of sepsis in preterm infants,78 only a few studies have directly focused on the association between neonatal sepsis and the neurodevelopmental outcome.910 Until now, in South Korea, no studies have addressed neurodevelopmental outcome associated with LOS in VLBWIs. This study is based on the Korean Neonatal Network (KNN), which is a nationwide database on VLBWIs across South Korea. We aimed to evaluate the effect of LOS during hospitalization at neonatal intensive care unit (NICU) on neurodevelopmental outcome using Bayley scales of infant development (BSID) at 18–24 months of corrected age in VLBWIs. Since brain injury of preterm infants frequently occurs at a gestational age ≤ 32 weeks,11 we focused on VLBWIs ≤ 32 weeks of gestation. We also aimed to ascertain the impact of LOS after adjusting for perinatal risk factors that may affect neurodevelopmental outcomes and parental education status.
Go to : 
METHODS
Study population
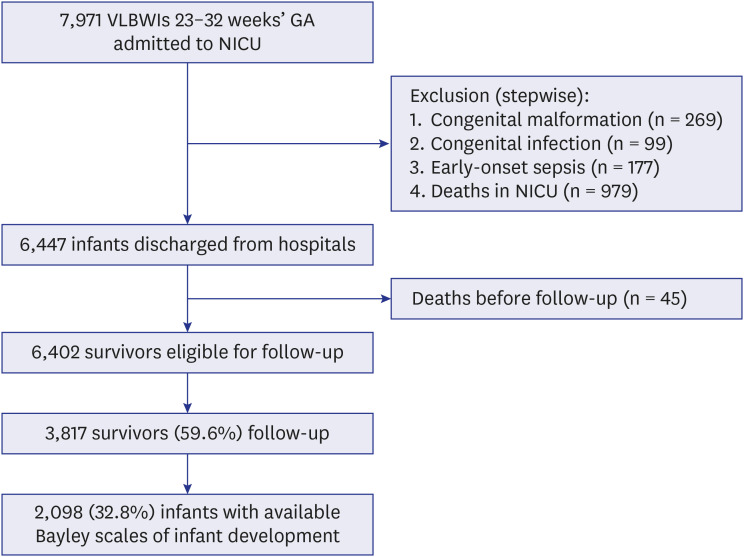
This is a population-based study of VLBWIs born at 23+0–32+6 weeks of gestation between January 2014 and December 2017 who were admitted to a NICU that participated in the KNN. Infants with severe congenital anomaly, congenital infection such as TORCH and syphilis or early-onset sepsis were excluded from the study. The KNN includes a database that accounts for approximately 70% of VLBWIs in South Korea. Data were collected at each participating center and entered into a data program. The study variables were defined according to the KNN manual. The present study was approved by the KNN data management committee. Fig. 1 shows the details of the study population. Follow-up was proposed at the time of hospital discharge for all 6,447 surviving infants. However, 45 infants died before follow-up and a total of 6,402 eligible survivors remained for follow-up at 18–24 months of corrected age. However, although follow-up could be done for a final total of 3,817 (59.6%), only 2,098 survivors (32.8%) who completed the BSID were included in this study.
Neurodevelopmental outcome
A total of 3,817 infants visited the centers for clinical follow-up; however, only 2,098 infants could be evaluated using the BSID at 18–24 months of corrected age by a trained psychologist at each center. Each center evaluated infants using the BSID second edition (BSID-II) or third edition (Bayley-III). Of the 2,098 infants, BSID-II was used to evaluate 1,113 (53.1%) infants, while Bayley-III was used to evaluate 985 (46.9%) infants. According to previous studies that compared scores between BSID-II and Bayley-III, both cognitive and motor delays were defined as scores < 70 in BSID-II and scores < 80 in Bayley-III, respectively.1213 As defined by those studies, we used a composite score for the cognitive function of Bayley-III, which calculated the average of cognitive and language scores.
Definition
Early-onset sepsis was defined as a confirmed infection within the third postnatal day of life.14 LOS was defined as a postnatally acquired infection which occurred after the third postnatal day of life.2 Only sepsis confirmed by blood culture was considered. Intraventricular hemorrhage (IVH) was defined using Papile's criteria by cranial ultrasonography.15 Since imaging was performed according to each hospital's policy, the worst grade among the cranial ultrasonography results during hospitalization was adopted. Intrauterine growth restriction (IUGR) was defined as birth weight less than the 10th percentile for the gestational age, based on a sex-specific growth chart.16 Since this study admitted the scores of both BSID-II and Bayley-III, we developed the variables ‘motor delay’ and ‘cognitive delay’ to combine the results. To develop these variables, the value of each result (0: normal, 1: delay) was entered according to the definition for BSID-II or Bayley-III.
Statistical analysis
Statistical analyses were performed using IBM Statistical Package for the Social Sciences statistics, version 23 (IBM, New York, NY, USA). Data are expressed as number (%) or mean ± standard deviation. Univariate analyses of categorical variables were performed using a χ2 test, and a t-test was used for continuous variables. To test for LOS as a risk factor for neurodevelopmental delay, multiple logistic regression was used and adjusted for clinical variables selected in the univariate analysis. Criteria for entry and removal were P < 0.05 and P > 0.10, respectively. To solve multicollinearity, variation inflation factors were measured, and the variable with a value of more than 10 was excluded. The fitness of the models used was checked using the Hosmer-Lemeshow goodness-of-fit test. A P value < 0.05 with two-tailed comparisons was considered significant.
Ethics statement
The KNN registry was approved by the institutional review board at Ewha Womans University Mokdong Hospital (approval No. EUMC2013-09-003), and informed consent was obtained from the parents at enrollment.
Go to :
RESULTS
Of the 6,402 VLBWIs discharged from the NICU, 1,170 (18.3%) had LOS. LOS was identified in 419 (20.0%) of the 2,098 VLBWIs with available BSID. The most frequently detected organisms were coagulase-negative Staphylococcus (48.8%) and coagulase-positive Staphylococcus aureus (14.6%) in 1,170 VLBWIs with LOS. Gram negative and gram positive bacteria accounted for 19.0% and 79.5% of them, respectively. The different organism, such as gram negative or gram positive bacteria, did not affect cognitive or motor delays (P = 0.686 in cognitive delay and P = 0.408 in motor delay). Survivors who were eligible for follow-up but did not have a BSID score had a higher gestational age, higher birth weight, and less frequency in comorbidities compared with those who had a BSID score (Table 1). VLBWIs with LOS who had a BSID score showed lower gestational age, lower birth weight, longer duration of hospitalization, prolonged mechanical ventilation, and longer period to reach full enteral feeding. The prevalence of comorbidities, such as IVH ≥ grade 3, IUGR, periventricular leukomalacia (PVL), and necrotizing enterocolitis (NEC) ≥ grade 2, and the frequency of postnatal steroid use was higher in VLBWIs with LOS. The ratio of maternal or paternal college graduation was lower in LOS group. However, the frequency of preterm rupture of membrane, histologic chorioamnionitis, and antenatal steroid use was not different in VLBWIs with and without LOS (Table 2). Cognitive delay was found in 392 (18.7%) of the 2,098 infants with available BSID. Cognitive delay was significantly more frequent in cases of IVH ≥ grade 3, IUGR, bronchopulmonary dysplasia (BPD), PVL, NEC ≥ grade 2, and postnatal steroid use and in male infants. The ratio of maternal and paternal college graduation was lower in VLBWIs with cognitive delay (Table 3). Motor delay was found in 347 (16.5%) of the 2,098 infants with available BSID. Motor delay was significantly more frequent in cases of IVH ≥ grade 3, IUGR, BPD, PVL, NEC ≥ grade 2, and antenatal or postnatal steroid use and in male infants (Table 4). In multivariate analysis, LOS was significantly related to cognitive delay but not related to motor delay. Both cognitive and motor delays were significantly associated with IVH ≥ grade 3, IUGR, PVL, NEC ≥ grade 2, and duration of mechanical ventilation. Male infants and NEC ≥ grade 2 were associated with only motor delay, whereas paternal college graduation was associated with only cognitive delay (Table 5).
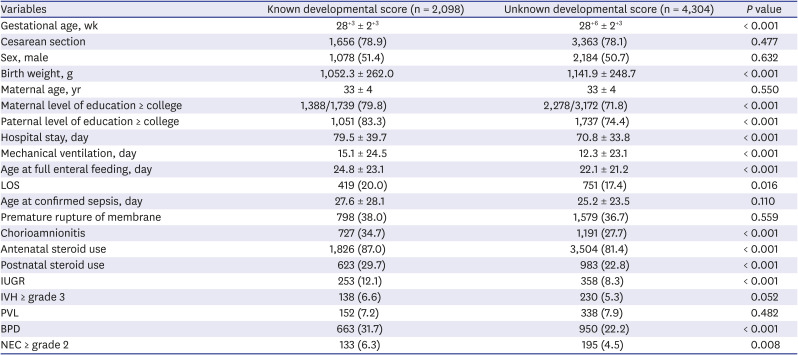
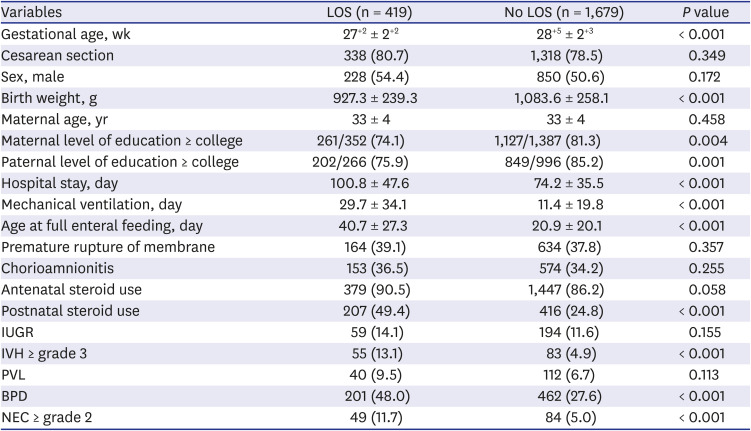
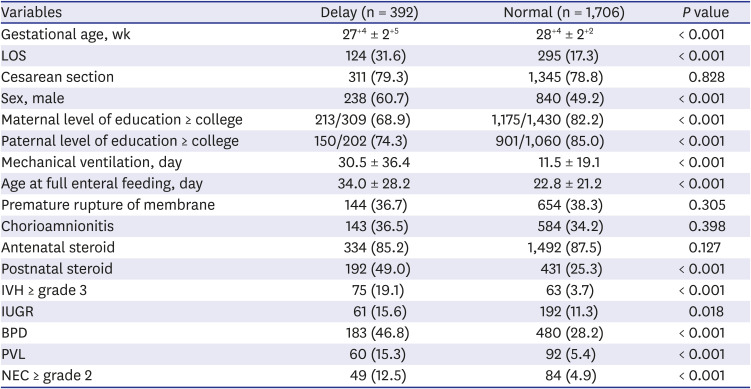
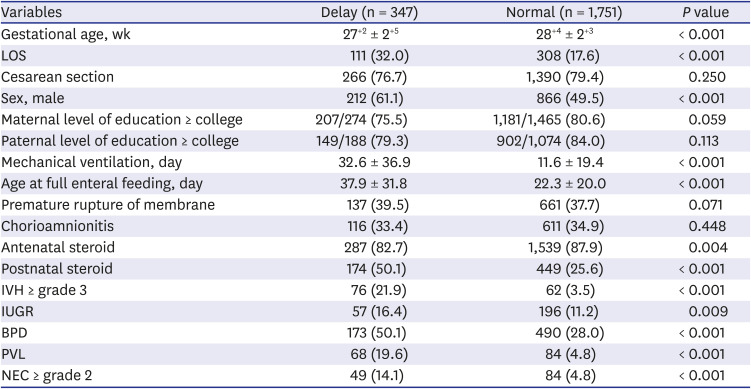
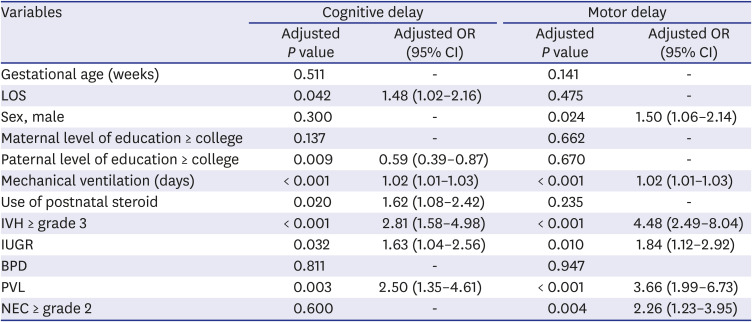
Table 1
Clinical characteristics in enrolled preterm infants compared to survivors without known developmental score
Values are presented as number (%). Continuous variables are expressed as mean ± standard deviation.
LOS = late-onset sepsis, IUGR = intrauterine growth restriction, IVH = intraventricular hemorrhage, PVL = periventricular leukomalacia, BPD = bronchopulmonary dysplasia, NEC = necrotizing enterocolitis.
![]()
Table 2
Comparison of clinical variables in enrolled preterm infants with and without LOS
Values are presented as number (%). Continuous variables are expressed as mean ± standard deviation.
LOS = late-onset sepsis, IUGR = intrauterine growth restriction, IVH = intraventricular hemorrhage, PVL = periventricular leukomalacia, BPD = bronchopulmonary dysplasia, NEC = necrotizing enterocolitis.
![]()
Table 3
Cognitive delay as a function of clinical characteristics
Values are presented as number (%). Continuous variables are expressed as mean ± standard deviation.
LOS = late-onset sepsis, IVH = intraventricular hemorrhage, IUGR = intrauterine growth restriction, BPD = bronchopulmonary dysplasia, PVL = periventricular leukomalacia, NEC = necrotizing enterocolitis.
![]()
Table 4
Motor delay as a function of clinical characteristics
Values are presented as number (%). Continuous variables are expressed as mean ± standard deviation.
LOS = late-onset sepsis, IVH = intraventricular hemorrhage, IUGR = intrauterine growth restriction, BPD = bronchopulmonary dysplasia, PVL = periventricular leukomalacia, NEC = necrotizing enterocolitis.
![]()
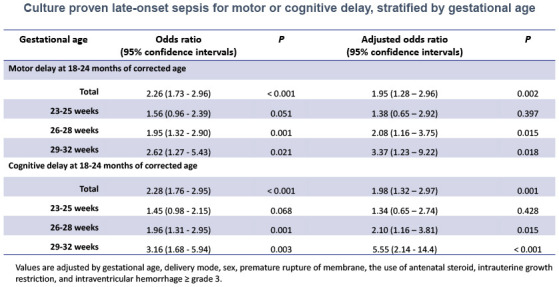
Table 5
LOS for cognitive or motor delays by multivariate analysis
Values are adjusted by all variables demonstrated in table.
OR = odd ratio, CI = confidence interval, LOS = late-onset sepsis, IVH = intraventricular hemorrhage, IUGR = intrauterine growth restriction, BPD = bronchopulmonary dysplasia, PVL = periventricular leukomalacia, NEC = necrotizing enterocolitis.
![]()
Go to :
DISCUSSION
We found that LOS in VLBWIs was associated with cognitive delay but not associated with motor delay at 18–24 months of corrected age after adjusting clinical variables that may affect neurodevelopmental outcomes. To date, several studies have confirmed that neonatal sepsis is a risk factor for neurodevelopmental delay.678 However, very few studies have directly investigated the potential link between sepsis and neurodevelopmental outcome.910 Stoll et al.9 reported that infected preterm infants who presented with isolated clinical infection, sepsis, or meningitis were significantly more likely to have a poor neurodevelopmental outcome at 18 to 22 months of corrected age. Mitha et al.17 and Bright et al.18 evaluated the effects of LOS on neurodevelopmental outcome in preterm infants at 5 years and 10 years of age, respectively. Mitha et al.17 suggested that the frequency of cerebral palsy occurrence was higher in infants with LOS, but there was no association between cognitive delay and LOS. In contrast, Bright et al.18 reported that infants with LOS were more likely to have cognitive delay but not motor delay. An increase in proinflammatory cytokines such as interleukin (IL)-6, IL-8, and tumor necrosis factor-α followed by sepsis interferes with maturation of the central nervous system by causing neuronal atrophy, delay in myelination, and acute reactive gliosis.41920 This pathophysiology can induce white matter damage, cerebral palsy, as well as cognitive delay, especially in preterm infants born at 23–32 weeks of gestation, which is the developmental window of vulnerability for brain injury.202122
In this study, the duration of hospital stay and mechanical ventilation were significantly longer, and the age for full enteral feeding was significantly higher in infants with LOS compared with infants without LOS. Furthermore, the frequency of major morbidities, such as IVH ≥ grade 3, BPD, PVL, and NEC ≥ grade 2, were higher in LOS group. At present, it is not clear whether these factors affected the occurrence of LOS or were the result of LOS.2324252627 The occurrence of chorioamnionitis was not different between VLBWIs with and without LOS. Chorioamnionitis is considered a risk factor for developing early onset sepsis in preterm infants, but recent data suggest that chorioamnionitis might be protective against LOS by modulating postnatal immunity.2829 In this study, cognitive and motor delays were associated with postnatal steroid use and male sex, respectively. Postnatal steroid has been well known to be associated with neurodevelopmental delay, and a previous study showed that preterm adolescents who received postnatal dexamethasone in the newborn period had smaller total brain tissue volumes than those who did not receive postnatal dexamethasone.30 Previous studies demonstrated that preterm male infants had a higher risk for major morbidities and mortality.3132 Several studies have also suggested a direct relation between the male sex and poor neurological outcome.3334 The results obtained in this study is in line with these reports.
The strength of the present study is that it is based on a large geographical cohort that includes approximately 70% of VLBWIs in South Korea. Furthermore, the data collection was obtained prospectively using the same strict guidelines of the KNN. In addition to various clinical variables, this study adjusted the effect of maternal age or parental level of education on neurodevelopmental outcome. The frequency of LOS was 18.3% in the 6,402 infants, and 20.0% in the 2,098 infants included in the analysis for neurodevelopment, which is lower compared with the frequency in previous studies (21–66%).17353637 This may be because the diagnosis of the present study was based on a specific criterion (a positive blood culture).
The main limitation of the present study is that the BSID was only evaluated in 2,098 infants (33%) among the eligible survivors, although more infants (60%) were present for their clinical follow-up. This loss of data could have led to biased results. The population of this study may not represent all VLBWIs in South Korea, because VLBWIs with BSID scores was smaller, younger, and more complicated compared with those without BSID. However, on the other hand, this study was not lack to see the effect of LOS on neurodevelopmental outcome because the study population included more than 2,000 VLBWIs and other clinical factors had been statistically adjusted.
The present study showed that VLBWIs with LOS were less than twice at risk of cognitive delay compared with those without LOS. This value is a little less than that obtained in previous studies.91732
In the present study, both versions of BSID-II and Bayley-III were accepted to increase the statistical power. Several studies have investigated the compatibility between BSID-II and Bayley-III and reported that Bayley-III scores are up to 10 points higher than BSID-II scores.121338 These studies suggested that Bayley-III scores < 80 provide the best definition of moderate-severe neurodevelopmental delay, which was equivalent to BSID-II scores < 70. We defined cognitive and motor delays according to these recommendations.
In conclusion, our study demonstrated a significant link between LOS and cognitive delay in VLBWIs born ≤ 32 weeks of gestation, even after adjusting parental social status and major clinical variables. Our findings are noteworthy to clinicians who counsel families of VLBWIs with LOS.
Go to :
 XML Download
XML Download