

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The coronavirus disease 2019 (COVID-19) pandemic has dramatically changed daily life.1 It became mandatory to wear a mask indoors and outdoors to prevent the spread of infection, and a number of countries closed their borders. Moreover, to prevent person-to-person transmission, lockdowns have been initiated in many countries. In South Korea, based on the number of infections, incremental increases in the stringency of social distancing measures have been implemented, and the prohibition of private meetings held indoors has been enforced. These social and environmental changes that can lead to social isolation may increase risk factors and decrease rescue factors associated with suicidal behavior.
Suicide is a major social and public health issue.23 Suicide was the fifth leading cause of death in South Korea in 2019.4 The suicide rate is on the rise, and South Korea has the highest suicide rate among OECD countries.5 The number of suicide attempts is up to 30 times greater than the number of completed suicides, and suicide attempts are correlated with social, cultural, environmental, biological, and psychological factors.23 The implementation of social distancing and lockdown to prevent the spread of COVID-19 lead to workplace closures and economic declines, resulting in employment instability that rendered millions of people jobless. Students took classes online at home, and social isolation was enforced in Korea. Indoor social gatherings and groups of more than 5 people in restaurants and bars were prohibited. Patients living in nursing homes experienced virtually complete quarantine due to the limitations imposed on family visits. During the pandemic, factors such as social isolation due to the enforcement of national policies intended to stop the spread of the disease (e.g., social distancing, lockdown, etc.), the fear of infection, and economic problems such as decreased income and unemployment may increase the rates of suicide and lead to changes in the clinical features associated with suicide attempts.67
Multiple cases of suicide related to COVID-19 have been reported in many countries.678910 A study in Japan reported that the suicide rate increased during the pandemic compared to before the pandemic.8 However, few studies have assessed changes in the lethality of suicide attempts associated with COVID-19 compared to before the pandemic. The risk-rescue rating scale (RRRS) can be used to evaluate lethality based on the level of risk and the possibility of rescue in those who have attempted suicide, and the validity and reliability of the RRRS have been shown to be satisfactory.11121314 The low-rescue and high-risk suicide attempts among patients who visited the ED after attempting suicide were considered more lethal suicide attempts.12 Due to the cultural environmental changes related to COVID-19, patients visiting the emergency department (ED) after attempting suicide may exhibit different clinical features associated with risk and rescue factors that affect the lethality of suicide. Additionally, social isolation or social disconnection during the COVID-19 pandemic may affect the probability of discovery by a rescuer and the time from the event to discovery of rescue factors.
Thus, the aim of this study was to investigate whether the factors affecting the lethality of suicide attempts differed before and during the COVID-19 pandemic using the RRRS in patients who attempted suicide and visited the ED. Second, we analyzed the demographic and psychologic factors affecting low-rescue suicide attempts in patients who attempted suicide.
METHODS
Study design
This study was conducted in the ED of a tertiary academic hospital and suicide crisis prevention center in South Korea. We performed a retrospective study of data obtained from medical records and counseling surveys from the ED-based suicide crisis prevention center. This suicide crisis prevention center in our hospital was started in 2017. All patients visiting the ED after a suicide attempt are registered, and counseling is requested during hospitalization. The aim of our prevention center is to prevent suicide by promoting collaboration between local communities and a tertiary-level ED.
Study population and protocol
Patients who had attempted suicide, were older than 15 years of age and had visited the ED after their suicide attempt between March 2019 and September 2019 (prepandemic period) and between March 2020 and September 2020 (during the COVID-19 pandemic) were included in the study. Patients who died on arrival after a suicide attempt were included. If it was impossible to interview the patient, counseling with the guardian was conducted. The exclusion criteria were patients with an unclear cause of the attempt and missing data.
After reviewing the medical and counseling records of patients who had attempted suicide, demographic data, including clinical factors, were collected. The demographic data included age, sex, medical history of chronic disease, employment status, and the time from suicide attempt to discovery. Other clinical factors were the method of the suicide attempt, the motivation of the suicide attempt, the initial vital signs in the ED, the initial Glasgow coma scale score, alcohol ingestion, previous suicide attempt history, and previous psychiatric history. In this study, patients who attempted suicide were divided into two groups based on whether they attempted suicide before or during the COVID-19 pandemic.
Suicide lethality was assessed using the RRRS.11 The RRRS is calculated based on five risk factors and five rescue factors. The risk factors consist of the method used, impairment of consciousness, toxicity, reversibility, and treatment required. The rescue factors include location, the person initiating rescue, the probability of discovery, the accessibility to rescue, and delay until discovery. Each of these factors is rated on a 3-point scale (1, 2, or 3) (Supplementary Table 1). After the risk and rescue factors are assessed, the points are summed to yield the total risk score and the total rescue score.11 High-risk suicide attempts were those with a total risk score of 11–15 points, and low-rescue suicide attempts were those with a total rescue score of 5–11 points. We defined high-lethality suicide attempts as those that were both high-risk and low-rescue attempts.12
Statistical analysis
The statistical analyses were performed using SPSS ver. 16.0 (SPSS, Chicago, IL, USA). The χ2 and Fisher's exact tests were used to compare categorical variables between patients who attempted suicide before and during the COVID-19 pandemic. The Mann-Whitney U test was used for nonnormally distributed variables, which are expressed as the medians (interquartile ranges; IQRs). P values less than 0.05 were considered significant. A multivariate logistic regression model was constructed to identify the independent risk factors. Age, male sex, medical history of chronic disease, previous suicide attempt, unemployed status, previous psychiatric history, alcohol ingestion and COVID-19 pandemic were set as variables to assess the demographic and psychologic factors affecting low-rescue suicide attempts. These variables are known clinical factors with significant correlations with suicide attempt lethality or risk-rescue ratio on the basis of a previous studies.12131415 The Hosmer–Lemeshow test was confirmed for goodness of fit for logistic regression models. The results are presented as odds ratios (ORs), 95% confidence intervals (CIs), and P values. N is the number of patients in each group.
Ethics statement
The data were reviewed and approved by the Incheon St. Mary's Hospital Institutional Review Board of the Catholic University of Korea (approval No. OC21RISI0033). The Incheon St. Mary's Hospital is a tertiary teaching hospital at which approximately 60,000 patients visited the ED. Informed consent was waived due to the retrospective study of medical records, which was confirmed by the Institutional Review Board of this hospital.
RESULTS
Characteristics of the study population
Of the 541 patients who visited to the ED after suicide attempts for whom surveys were completed in the ED-based suicide crisis prevention center during the study period, 23 patients with incomplete or missing data were excluded. Thus, 518 patients were included in this study, 275 (53.1%) of whom attempted suicide during the COVID pandemic. The most common suicide attempt methods were ingesting poison, cutting and stabbing (450 patients; 87.0%). Seventeen (3.3%) were dead on arrival (completed suicide) at the ED after a suicide attempt.
The median (IQR) age was 38 (24–55) years, and 205 (39.6%) patients were male. Age, sex, and method of suicide attempt were not significantly different between the periods before and during the COVID-19 pandemic. Suicide attempts associated with mental disorders were more common in the before COVID-19 group (P < 0.001). The medical history of chronic disease was significantly higher in the group of patients who attempted suicide during the COVID-19 pandemic (P = 0.011). The history of a previous suicide attempt differed significantly between the two groups (P = 0.016). Additionally, employment status which are factors associated with socioeconomic status, differed significantly between the two groups (P = 0.001) (Table 1).
Table 1
Demographic characteristics of the patients
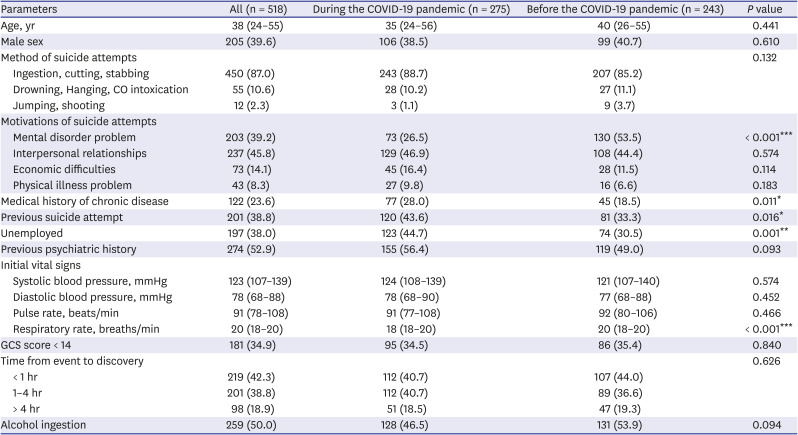
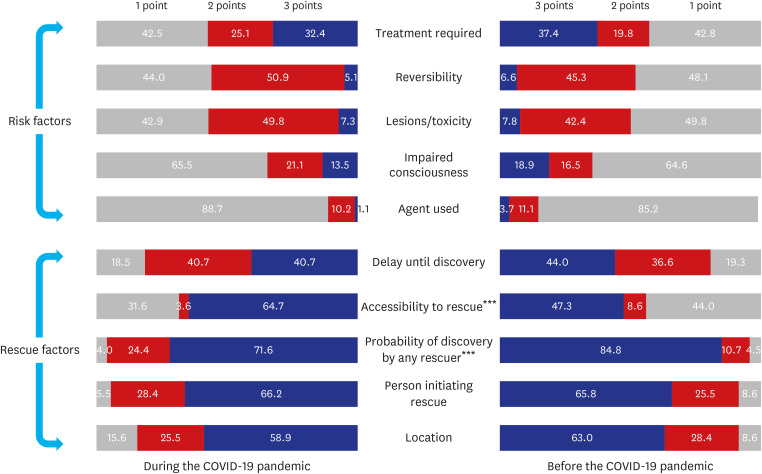
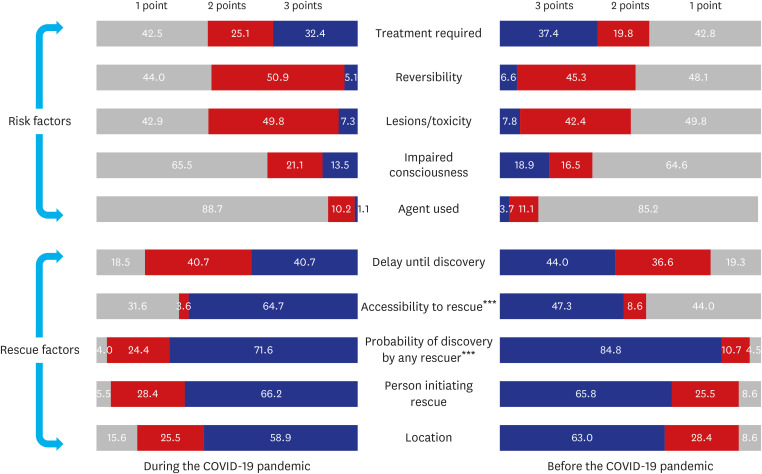
Fig. 1 shows the frequencies of the risk and rescue factors among these subjects. A score of 3 points for accessibility to rescue (3 points: asked for help, 2 points: dropped clues, 1 point: did not ask for help) was significantly more common during the COVID-19 pandemic (P < 0.001). However, a score of 3 points for the probability of discovery by any rescuer (3 points: high and almost certain, 2 points: uncertain, 1 point: accidental discovery) was less common during the COVID-19 pandemic (P < 0.001).
Fig. 1
Frequencies of scores before and during the COVID-19 pandemic.
Values are expressed as number (%) and the χ2 test was used for statistical analysis.
COVID-19 = coronavirus disease 2019.
***P < 0.001.
Eighty-two (15.8%) of the total number of suicide attempts were high-risk suicide attempts, defined by a total risk score of 11–15 risk, and 172 (33.2%) of the suicide attempts were low-rescue suicide attempts, defined by a total rescue score of 5–11 points. In total, 33 (6.4%) patients made high-lethality suicide attempts. The total risk score and rescue score were not significantly different before and during the COVID-19 pandemic. The proportions of high-risk suicide attempts and high-lethality suicide attempts did not differ significantly between the two periods. The proportion of low-rescue suicide attempts was significantly higher during the COVID-19 pandemic (P = 0.046). The rates of hospital admission, intensive care unit admission and mortality were not significantly different between the two periods (Table 2).
Table 2
Risk-rescue score and outcome of the patients

The analysis of 501 patients excluding those who completed suicide showed similar results. The proportion of patients who made low-rescue suicide attempts differed before and during the COVID-19 pandemic (P = 0.036) (Supplementary Table 2).
Prediction of low-rescue suicide attempts
For all the subjects, age and the COVID-19 pandemic were independent risk factors for low-rescue suicide attempts (OR, 1.02; 95% CI, 1.00–1.03; P = 0.006) (OR, 1.52; 95% CI, 1.03–2.25; P = 0.034). This multivariate logistic regression analysis for low-rescue suicide attempts was acceptable according to the Hosmer-Lemeshow goodness of fit test (χ2 = 9.5, P = 0.298). Regarding psychiatric factors, the history of previous suicide attempts and previous psychiatric history were not significant independent factors (Table 3).
Table 3
Multivariate logistic regression model for low-rescue suicide attempts
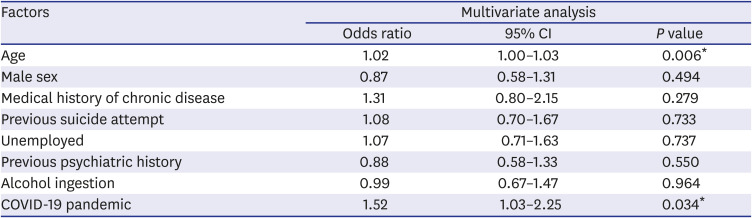
Multivariate logistic regression analysis excluding patients who completed suicide is presented in Supplementary Table 3. Age (OR, 1.01; 95% CI, 1.00–1.03; P = 0.021) and the COVID-19 pandemic (OR, 1.49; 95% CI, 1.00–2.21; P = 0.049) were independent risk factors for low-rescue suicide attempts.
DISCUSSION
This analysis of the demographic and psychiatric factors influencing low-rescue suicide attempts revealed that age and the COVID-19 pandemic were independent risk factors. Mortality due to suicide increased during the Spanish Flu outbreak and the severe acute respiratory syndrome outbreak in 2003.1617 It has been suggested that psychological, social, and economic factor, such as stress due to the fear of infection, depression due to social isolation, and economic crises such as a decrease in income and unemployment could contribute to increased suicide rate.1617 The higher the lethality of the suicide attempt, the more likely it is to result in death, and the lethality can be predicted by considering various risk factors and rescue factors.1112 If the risk score is high and the rescue score is low, the attempt is considered a high-lethality attempt.1112 Therefore, since low-rescue suicide attempts are related to a higher mortality rate, it is important to identify the factors influencing low-rescue suicide attempts. In this study, the COVID-19 pandemic was associated with an OR of 1.52 for low-rescue suicide attempts. Recent studies have reported that depressive symptoms, psychological distress, stress, and anxiety have increased during the COVID-19 pandemic.91819 Suicide attempts may be affected by this emotional stress and social stress. Quarantines can intensify depressive mood and anxiety.1819 Due to the recent demographic characteristics of Korean society, single-person households are on the rise and accounted for 30.2 percent of total households in 2019.20 In addition to these demographic characteristics, the social isolation and economic difficulties caused by the pandemic can lead to absence of family support and disconnection in social relationships, so the rescue scores for those attempting suicide can be expected to be low during the pandemic.
In rescue factor analysis, among the five rescue factors, a score of 3 points (high and almost certain) for the “probability of discovery by any rescuer” was less common during the pandemic. This category refers to the potential availability of any rescuer at the time of the suicide attempt. High, almost certain means that rescuers are nearby or will encounter the attempt immediately after it has occurred.11 Because of social isolation and quarantine measures implemented during the pandemic, leading to small social networks and infrequent interaction with social groups or families, individuals who have attempted suicide may show a low score for the “probability of discovery by any rescuer” as the results of this study indicate. The COVID-19 pandemic may have affected suicide lethality by influencing social factors related to increased low-rescue attempts. However, this study did not show any difference in lethality between suicide attempts made before and during the COVID-19 pandemic. This study is limited by the fact that the data were obtained from a single center, and it is necessary to further analyze the association of suicide lethality with rescue factors in prospective large-scale studies.
There have been reports in previous studies of a high lethality rate of suicide in older individuals.1521 Earlier studies indicated that depressive disorder, physical illness, and high suicidal intent were associated with high-lethality suicide attempts in older age groups.2223 In another study, patients who attempted suicide by ingesting poison were older in the low-rescue group than in the high-rescue group.12 One study of the RRRS reported that old age, male sex, alcohol intoxication, the presence of interpersonal stress, and a history of schizophrenia were independent factors associated with the risk-rescue ratio in individuals younger than 65 years of age.15 In this study, age was also an independent factor associated with low-rescue suicide attempts, which was consistent with previous studies. The pandemic may not have had an equal effect on the whole population of suicide attempters; for instance, it may have had more negative effects on some vulnerable individuals related to social isolation and social lockdown. Notably, it has been reported that there were more suicide attempts in older adults, those with preexisting mental illness, and those who were unemployed.242526 Older adults and individuals with serious preexisting mental illness may be vulnerable to suicide, self-harm and negative emotions through infrequent social interactions, requirements to stay home, increased risk of anxiety and aggravation of depression due to reduced social networks during the pandemic.2728
Unemployment is known to be a strong risk factor for suicide attempts.2930 Nordt et al.31 reported that the risk of suicide was elevated by 20–30% in those who were unemployed. Previous studies have predicted that the worldwide unemployment rate would increase due to the COVID-19 pandemic and that such an increase would be associated with an increase in suicide.3233 In this study, the unemployment rate differed in the groups of patients who attempted suicide before and during the COVID-19 pandemic. Therefore, in the case of a global disaster such as the COVID-19 pandemic, policies that can provide socioeconomic assistance such as unemployment benefits may be helpful for preventing suicide. In addition, to prevent vulnerable individuals from attempting to commit suicide, it is necessary to reduce the loneliness and psychosocial stressors experienced by this population due to isolation during the COVID-19 pandemic and to collaborate with community-based mental healthcare centers to facilitate social network integration for vulnerable individuals.
Our study has several limitations. First, this was a retrospective single-center analysis. Therefore, researchers collected emergency medical and counseling records and calculated the RRRS. This means that there is a risk of recall bias. Other confounders that could affect suicide attempts, such as variable psychiatric disorders, marital status, and factors related to socioeconomic status other than unemployment and monthly income, were not analyzed. During the study period, there were two waves of the COVID-19 pandemic in South Korea, and each wave occurred in a different location. The first wave was concentrated in Daegu metropolitan city, which is far from the Seoul, the capital city, and occurred in March. The second wave was concentrated in the metropolitan area of Seoul. Our center is located near Seoul. Due to these regional differences, the effects of the COVID-19 pandemic on individuals attempting suicide may vary, and the generalizability of the results from a single center is limited.
In conclusion, this study compared the factors affecting the lethality of suicide attempts between the periods before and during the COVID-19 pandemic using the RRRS and found that the COVID-19 pandemic was associated with low-rescue suicide attempts. These findings show that social policies and support may need to be strengthened to improve rescue factors among those attempting suicide during the COVID-19 pandemic or similar crises.
 XML Download
XML Download