

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Sedation is a key practice in intensive care units (ICUs) for minimizing patient discomfort and anxiety, facilitating mechanical ventilation (MV) and enabling essential ICU procedures.12
Critically ill patients have been heavily sedated and immobilized which often resulted in post-intensive care syndrome, leading to severe cognitive dysfunction and neuromuscular disability lasting months to years.3 In addition, critically ill patients are susceptible to adverse drug events due to organ dysfunction, unstable hemodynamics, unpredictable absorption, protein binding, and altered pharmacokinetics and pharmacodynamics secondary to drug interactions.4 When aimed at the same sedation target, benzodiazepines more frequently reach above-target sedative depths than dexmedetomidine.5 Daily sedation interruption6 and the Awakening and Breathing Coordination, Delirium monitoring/management and Early exercise/mobility bundle78 reduced the duration of MV, ICU length of stay (LOS) and hospital mortality by reducing pain, oversedation, and delirium. Recent controlled studies have suggested that light sedation using dexmedetomidine-based or propofol-based sedation in ICU patients reduces the ICU LOS and the duration of MV, compared to deeper sedation with benzodiazepines.9 The transition toward light sedation has been strongly recommended since the 2013 Pain, Agitation, and Delirium guidelines.10 The updated 2018 guidelines recommend using non-benzodiazepine sedatives (either propofol or dexmedetomidine) instead of benzodiazepines for critically ill adults undergoing MV, given the improved short-term outcomes for ICU LOS, MV duration, and delirium.1112 However, there has been no large scale investigation of the correlation between in-hospital mortality and the type of sedative used in patients who require MV for 48 hours or more.
The National Health Insurance Service (NHIS) database used in our study contains all claims data for the population covered under the National Health Insurance (NHI) program and the Medical Aid program in Korea. The NHIS provides its database to researchers after de-identification of private and sensitive information for research purposes.13
Our study objective was to assess the correlation between sedatives and mortality in critically ill patients who required MV for 48 hours or more using the NHIS database. We hypothesized that non-benzodiazepine-based sedation for patients requiring MV may be associated with lower in-hospital mortality.
Go to : 
METHODS
Data source and study population
Data from adult patients (aged ≥ 18) who underwent MV for ≥ 48 hours between 2008 and 2016 were identified and extracted from the NHIS database by searching for the NHI codes AJ100, AJ110, AJ120, AJ130, AJ140, or AJ150 during the patients' hospitalizations. Data on underlying comorbidities such as hypertension (I10–13), diabetes mellitus (E10–14 and R81), coronary artery disease (I20–23), chronic kidney disease (K74), cerebrovascular disease (I63–67), and malignancy (C34, C79, C82–85, C90, C91, and C161) were extracted from the database using International Classification of Diseases 10th revision (ICD-10) codes. The Elixhauser comorbidity index, derived from 30 disease entities using ICD-10 codes14 and shown to correlate with hospital mortality,15 was used as a covariable to adjust for disease severity. The Elixhauser comorbidity system has been shown to be slightly superior to the previously used Charlson comorbidity system at adjusting for comorbidity.16
Data on in-hospital mortality, ICU LOS, and hospital LOS were also extracted. Because death certificates are automatically reported to the NHI, the patients' one-year mortality was detected when NHI healthcare coverage was terminated due to death.
Primary and secondary outcomes
The primary outcome was in-hospital mortality. Secondary outcomes were trends in sedative use, ICU LOS, hospital LOS, and 1-year mortality. In-hospital mortality and 1-year mortality was defined as death occurring during the hospital stay and death within 1 year after hospital discharge, respectively. Risk factors for in-hospital mortality and 1-year mortality were also evaluated.
Definition of groups and case volume
The benzodiazepine group consisted of patients who were administered benzodiazepines (a total dose of midazolam ≥ 60 mg, lorazepam ≥ 40 mg, or diazepam ≥ 100 mg) with or without other sedative agents for sedation during MV. The non-benzodiazepine group consisted of patients who did not receive any benzodiazepines or received benzodiazepine less than the predetermined dose. The case volumes were categorized as follows: low (< 300 cases/year), medium (300–500 cases/year), and high (> 500 cases/year).
Statistical analysis
After classifying patients depending on the use of benzodiazepines, the two groups were compared using the Mann-Whitney U test for continuous variables due to the skewed distribution. The χ2 test was used to compare categorical variables due to the large sample size. The correlation between the use of benzodiazepines and the annual in-hospital mortality between 2008 and 2016 was assessed using the Pearson's correlation test. In-hospital and one-year mortality were assessed using a logistic regression model after adjusting for age, sex, comorbidities, and the mean Elixhauser comorbidity index. We assessed the goodness-of-fit for logistic regression using the Hosmer-Lemeshow test and used a Poisson regression analysis to examine trends across the study period and sedatives after adjusting for age, sex, and mean Elixhauser comorbidity index.
All analyses were performed using SAS 9.4 (SAS Institute, Cary, NC, USA). The results were considered statistically significant when the P value was < 0.05.
Ethics statement
This study was a retrospective cohort study and the study protocol was approved by the Institutional Review Board of Seoul National University Hospital (1801-023-912). The need for informed consent was waived by the institutional review board due to the retrospective design of the study.
Go to :
RESULTS
Between January 2008 and December 2016, 55 centers in Korea admitted 158,712 patients requiring MV for ≥ 48 hours. Some 39.7% (63,043) of these patients were administered benzodiazepines during their ICU stays, the most commonly employed of which was midazolam (97.6%).
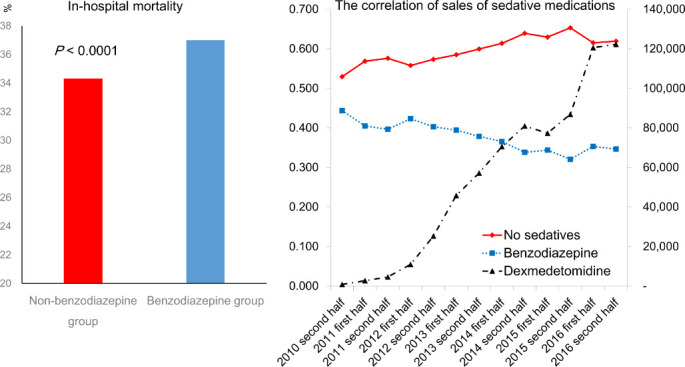
The overall in-hospital mortality rate was 35.4% (56,133/158,712). The benzodiazepine group had significantly higher in-hospital and one-year mortality than the non-benzodiazepine group (37.0% vs. 34.3%, 55.0% vs. 54.4%, respectively, Table 1). The relative risk of in-hospital mortality in the benzodiazepine group was 1.08 (1.07–1.1) compared to the non-benzodiazepine group, with a relative risk increase of 8.04%. The overall median ICU and hospital LOS were 12 days and 26 days, respectively. The median ICU and hospital LOS were longer for the benzodiazepine group than for the non-benzodiazepine group (13 vs. 12 days, 27 vs. 26 days, respectively; Table 1).
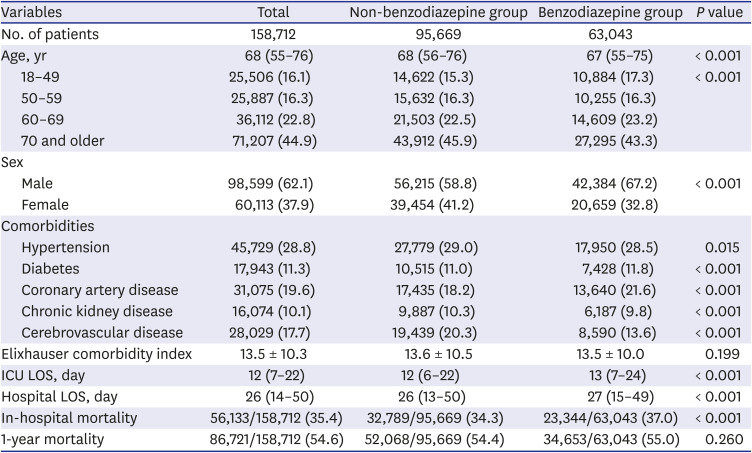
Table 1
Characteristics of patients and centers
Numbers reported as number (%), median (interquartile range), or mean ± standard deviation.
ICU = intensive care unit, LOS = length of stay.
![]()
The use of benzodiazepine was significantly correlated with in-hospital mortality between 2008 and 2016 in the Pearson's correlation test (correlation coefficient, 0.491, P = 0.038).
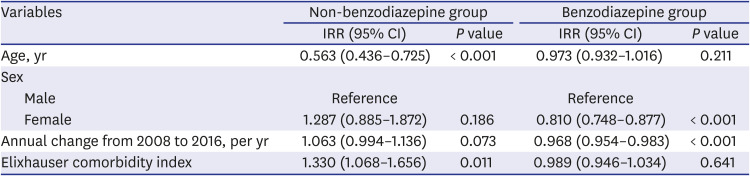
Benzodiazepine use decreased from 2008 to 2016, after adjusting for age, sex, and mean Elixhauser comorbidity index in the Poisson regression analysis (incidence rate ratio, 0.968; 95% CI 0.954 – 0.983; P < 0.001; Table 2). Since the second half of 2010, dexmedetomidine sales have continuously increased, whereas the use of benzodiazepines has steadily decreased, and the correlation was significant (correlation coefficient, −0.861; P < 0.001; Fig. 1).
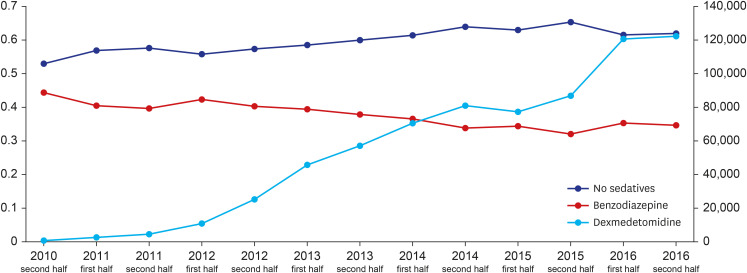 | Fig. 1The correlation of sales of sedative medications (Dexmedetomidine data from IQVIA Sales Audit from 2010 3Q to 2016 4Q).
|
Table 2
Trends in use of sedatives in patients requiring mechanical ventilation for 48 hours or more in the intensive care unit
Poisson regression after adjusting for age, sex, and mean of Elixhauser comorbidity index. Use of sedatives per 100 patients.
IRR = incidence rate ratio, CI = confidence interval.
![]()
In the multivariable logistic regression analysis, the benzodiazepine group was associated with higher in-hospital and one-year mortality compared to the non-benzodiazepine group. Older age, lower case volume (≤ 500 cases/year), chronic kidney disease, and higher Elixhauser comorbidity index were common significant risk factors for in-hospital and one-year mortality (Table 3).
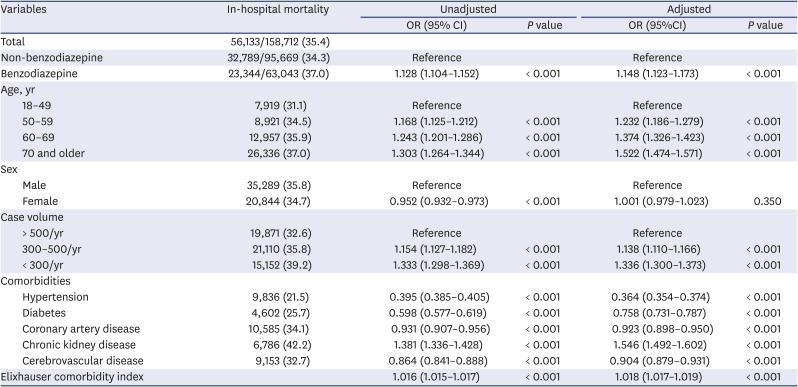
Table 3
Univariable and multivariable logistic regression analyses for in-hospital mortality
Numbers reported as number (%) and OR (95% CI).
Multivariable logistic regression after adjusting age, sex, case-volume, and comorbidities.
OR = odds ratio, CI = confidence interval.
![]()
Go to :
DISCUSSION
In this nationwide study, mechanically ventilated ICU patients who did not receive benzodiazepines had a lower risk of in-hospital mortality and an increased likelihood of earlier ICU discharge compared to patients who were sedated with benzodiazepines.
Data from current controlled studies suggest that sedation with dexmedetomidine or propofol instead of benzodiazepines can reduce the ICU LOS and MV duration for critically ill adults.9 These findings can be explained by a rapid onset of activity, rapid recovery after discontinuation, and easy titration of dexmedetomidine or propofol, whereas benzodiazepines are more likely to accumulate, especially when administered concomitantly with other drugs and administrated as a continuous infusion.1718 Midazolam, the most commonly used benzodiazepine in our data, is not recommended for long-term (≥ 48 hours) sedation1 because prolonged infusion results in prolonged time-to-awakening due to an accumulation of its active metabolite.19 However, there are few studies comparing sedatives in terms of clinical outcomes such as mortality in an ICU setting.
The lower in-hospital mortality rate associated with not using benzodiazepines is somewhat contradictory to previous studies, but the similar 1-year mortality rate is in accord with the existing literature. A recent network meta-analysis that included 52 randomized controlled trials (RCTs) comparing sedatives in MV patients associated dexmedetomidine with a shorter MV duration than benzodiazepines and propofol, and shorter hospital LOS than propofol. The meta-analysis also showed that midazolam was associated with a significantly higher risk of delirium than dexmedetomidine.20 However, the mortality rate was not significantly different between dexmedetomidine and other sedatives. Another meta-analysis comparing propofol to benzodiazepines that included 16 RCTs showed similar results, with a significant reduction in ICU LOS for patients treated with propofol and no significant difference in mortality between propofol and other sedatives.21 A recent RCT that examined mortality as a primary outcome of patients with sepsis who required MV demonstrated that using dexmedetomidine for sedation did not show a benefit in terms of mortality.22 Similarly, an open label clinical trial that compared dexmedetomidine and usual care for early sedation in ICU patients requiring MV also did not show a difference in 90 day mortality.23 The lack of a difference in the mortality rate could have been due to the study’s lack of power to detect a difference, a limitation the authors acknowledged.22 Recent studies reported that sedation depth predicted mortality2425 and sedation intensity was associated with mortality in an ascending relationship.26 The sedation target of the SPICE III trial23 was light sedation with a Richmond Agitation Sedation Scale (RASS) score of −2 to +1. However, more than 40% of patients in both dexmedetomidine and usual care groups were deeply sedated (RASS −5 to −3) in the first 2 full days after randomization. In addition, almost 75% of patients in the dexmedetomidine group received additional sedatives such as propofol, midazolam or both to achieve target sedation level. Therefore, it was suggested that no difference in 90-day mortality should be interpreted with caution because of the high percentage of deep sedation in both groups and use of additional sedatives in the dexmedetomidine group.27
Lonardo et al.28 reported that patients sedated with propofol had a lower risk of in-hospital mortality and were more likely to be discharged earlier from the ICU and MV discontinued compared to patients administered benzodiazepines. The authors analyzed only propofol as a non-benzodiazepine sedative, comparing midazolam and lorazepam using a multicenter ICU database (2003–2009) that included 3,300 patients. Similar to their study, our nationwide data (2008–2016) showed that patients administered non-benzodiazepines (including propofol and dexmedetomidine) had a reduced risk of in-hospital mortality and shorter duration of ICU LOS compared to patients who received benzodiazepines.
In our study, the non-benzodiazepine group consisted of patients treated with propofol, benzodiazepine less than the predetermined dose, or non-sedatives. Non-sedatives are defined in our study as the non-use of sedatives or the use of sedatives not covered by insurance. Korean ICUs have been using dexmedetomidine since the second half of 2010. However, we could not extract data from the NHIS database on dexmedetomidine use because the drug was not yet covered by the NHI in South Korea. Therefore, we assumed the use of dexmedetomidine from its sales volume, which steadily increased from the start, and then sharply increased since the second half of 2012. The trend is significantly related to a decrease in the rate of benzodiazepine use. The general trend and pattern of benzodiazepine use in ICU patients shown in our study is similar to a previous study which showed that benzodiazepine use decreased, whereas propofol, a non-benzodiazepine sedative, use increased in mechanically ventilated patients.29
Benzodiazepines were significantly associated with in-hospital mortality in the study by Lonardo et al.,28 and in our study, and are a known risk factor for delirium in critically ill patients.30 Activation of the γ-aminobutyric acid receptor has been proposed as a possible mechanism for this risk.31 The association between delirium and in-hospital mortality is also well known,32 thereby resulting in increased mortality for patients sedated with benzodiazepines who subsequently experience delirium. Another plausible explanation for increased mortality in the benzodiazepine group is the longer ICU LOS compared to the non-benzodiazepine group. Prolonged ICU stay is associated with an increase in ICU-related complications, such as delirium and mortality.33
Our study identified advanced age, low case volume, chronic kidney disease, and a higher Elixhauser index as risk factors for in-hospital and one-year mortality. Previous studies have confirmed that advanced age is a significant risk factor for mortality in critically ill patients34 and patients requiring MV.35 A recent study reported that pre-existing chronic kidney disease had a profound effect on the 30-day mortality and 1-year mortality of critically ill patients requiring MV in accordance with our study.36 Low case volume is associated with higher mortality37 due to the lower probability of multidisciplinary ICU teams and the implementation of patient care protocols such as light sedation with non-benzodiazepine sedatives.3839
The NHI program in Korea is a single-payer, universal healthcare system supported by the NHIS, providing health coverage to 97% of the Korean population, while the Medical Assistance Program supports the remaining 3% of the population with the lowest income.40 Whenever health care is provided, healthcare providers apply for reimbursement to NHIS, which is then recorded in the NHIS database. The breadth and completeness of the NHIS database used in our research is another strength of our study. Only explicit outcomes, such as mortality and LOS, were employed as final results. Although the NHIS database was the most appropriate database use to analyze the main clinical question of our study, the NHIS database lacked most of the clinical data.
Our study had several limitations. First, due to the relatively long study period, the outcomes of patients who underwent MV for ≥ 48 hours could have been affected by medical progress during the study period. However, considering the long history of lung protection ventilation, and the universal approach to medical advances, the impact of relatively long research periods is expected to be uniform and minimal. Second, we were unable to distinguish between medical admission and surgical admission, and we were unable to extract diagnoses on ICU admission from the NHIS database. However, patients who underwent MV for < 48 hours were excluded because their disease severity was considered low. According to a comprehensive report on ICUs by the Korean Society of Critical Care Medicine 2015, about 20% of ICU patients were admitted to the ICUs for postoperative care. In addition, about 10% of mechanical ventilated patients in the ICU were patients with postoperative acute respiratory failure in a previous multicenter survey study.41 Therefore, most the study population were severely ill medical patients. Third, it is difficult to ascertain the exact reason for sedative use. Although pre-determined cumulative doses were set for each benzodiazepine to include patients requiring sedation for MV, the pre-determined dose for each sedative was somewhat arbitrary. However, the pre-determined dose was set to exclude patients receiving the drug for procedural sedation and minimize exclusion of patients receiving subnormal dosages due to relatively shorter duration of MV. Also, patients requiring benzodiazepines for other reasons such as seizures including status epilepticus may have been included. Fourth, previous studies showed that deep sedation was related to complications such as ventilator-associated pneumonia,42 deirium,43 and death,26 but this study has a limitation in that the sedation depth could not be confirmed. In addition, 2018 PADIS guidelines recommended analgesia-first sedation or analgeia-based sedation.11 However, we could not assess whether adquate pain control was offered or not. Fifth, due to the lack of individual follow-up, the cause of death, especially at 1 year, was difficult to single out. Factors other than the type of sedative used for sedation in the ICU during the prior hospital admission may have contributed.
In conclusions, the use of benzodiazepines for sedating critically ill patients undergoing MV for > 48 hours was associated with higher in-hospital mortality and one-year mortality compared to the use of non-benzodiazepines. Considering the recent guidelines and the rapid increase in non-benzodiazepine use, sedation with non-benzodiazepines may have contributed to better short-term and long-term outcomes in patients who required prolonged MV.
Go to :
 XML Download
XML Download