

 PDF
PDF Citation
Citation Print
Print



A close contact in a severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) context is defined by the Centers for Disease Control and Prevention (CDC) as someone who has been within 6 feet of a SARS-CoV-2 -infected person for a cumulative total of 15 minutes or more over a 24-hour period.1 Non-close contacts can continue daily life and are requested by health authorities to self-monitor and perform SARS-CoV-2 polymerase chain reaction (PCR) if they develop symptoms.2 However, non-close contacts as well as close contacts can end up diagnosed as coronavirus disease 2019 (COVID-19) after exposure, and non-close contacts can make further contacts and transmit the infection. However, there is limited data on the proportion and characteristics of secondary cases initially classified as non-close contacts. Therefore, we aimed to investigate the proportion of secondary cases initially classified as non-close contact, and the characteristics of non-close contact exposure to the index patients in a nosocomial outbreak.
This study was performed in a tertiary care hospital in Seoul, South Korea, from March 2020 to March 2021. We analyzed the secondary nosocomial COVID-19 cases initially classified as close contact versus non-close contact. Close contacts were defined as 1) those who were in close proximity (< 6 feet) for at least cumulative 15 minutes within 2 days of symptom development in the index, or within 2 days of the date of collection of a positive specimen in indexes that were asymptomatic,1 2) inpatients or guardians who shared the same (multi-patient) room with the case patient or anyone who had a meal with the index (equivalent exposure to household), or 3) contact with the index patient when an aerosol-generating event that occurred without appropriate personal protective equipment (PPE) (N95 or FFP2-equivalent respirator, face shield/goggles, gown, and gloves). Non-close contacts were defined as those who did not meet the criteria of close contact but had possible temporal or spatial contact with the confirmed patient. We performed whole-genome sequencing (WGS) for specimens from index and secondary cases to confirm or refute their association, whenever possible. Detailed contact tracing, definition, and method of WGS are described in Supplementary Material 1.
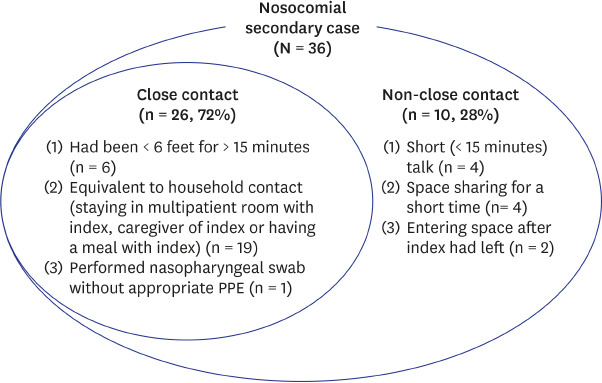
During the study period, there were 440 close contacts and 2,198 non-close contacts from 14 index cases (9 patients or caregivers and 5 healthcare workers [HCWs], Supplementary Table 1). There were 26 (5.9%) secondary cases from close contacts and 10 (0.5%) from non-close contacts (P < 0.001 by χ2 test) (Fig. 1). The secondary attack rates among close contact were 1.2% (1/81), 6.9% (6/87), 7.0% (19/272) in 1st, 2nd, and 3rd wave, respectively (P = 0.142). The secondary attack rates among non-close contact were 0% (0/1125), 0.9% (2/234), and 1.0% (8/839) in 1st, 2nd, and 3rd wave, respectively (P = 0.005) (Supplementary Fig. 1). We performed WGS for 22 SARS-CoV-2-infected individuals with vague epidemiologic links (7 index and 15 secondary cases), but failed in 4 cases due to poor sample quality. We performed WGS for 5 pairs of the index and secondary cases classified as non-close contact, but 2 pairs failed due to poor sample quality. Most close contacts (19 [73%]) were equivalent to household contacts, as they were caregiver of the index patient, stayed in a multi-patient room with index, or had a meal with the index. Six (23%) close contacts had been within 6 feet of an infected person for a cumulative total of > 15 minutes as revealed by interview or CCTV. The remaining HCW (4%) had taken a nasopharyngeal swab for SARS-CoV-2 PCR without appropriate PPE (wearing KF94 mask and gloves without goggle and gown).
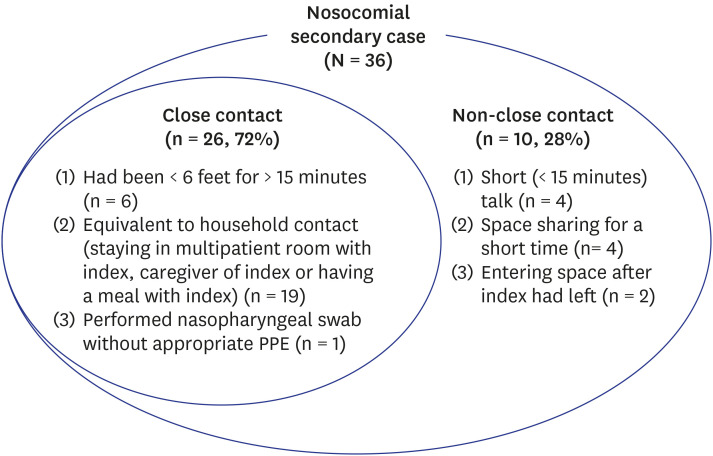
Detailed characteristics of the exposure of the 10 non-close contacts are presented in Supplementary Table 2. Of the 10 non-close contacts, four (40%) had brief conversations (median, 1.5 minutes; range, 0.3–3) while both were masked, four (40%) shared a space, with both masked, but without talking (using the ward communal utility room at the same time, staying in the same ward but in different cubicles, being in the office while the index cleaned there, and brushing teeth in the bathroom while index environmental cleaners were there cleaning) and the remaining two (20%) entered the space after the index had left (entered a shared shower room with poor ventilation, and changed bed-linen that the index had used, respectively). Of the 10 non-close contacts, only one was responsible for secondary transmission, but 5 without 2-week quarantine were eventually diagnosed as SARS-CoV-2 infection that resulted in additional contacts (Supplementary Table 2). Index 14 (Supplementary Table 1) was probably the index of other HCW (D in Supplementary Table 2) without any close contact; they had short conversation (20 seconds) 1 day before symptom onset of index 14. We could not perform WGS for this pair.
In this study, we found that at least a quarter of SARS-CoV-2 transmissions in a healthcare setting occurred among non-close contacts. Secondary cases that were initially classified as non-close contact had conversations of a median of 1.5 minutes with the index, shared space with the index, or entered the space after the index had left. Similarly, Mack et al.3 showed that of 21 persons with transmission suspected to have occurred within a national football league club, 12 (57%) had no interactions of more than 15 consecutive minutes, 7 (33%) had no interactions of more than 15 cumulative minutes per day, and 8 (38%) had no interactions of more than 5 consecutive minutes. Another study also found that 4 of 23 infected healthcare workers (17%) had < 15 minutes cumulative exposure to SARS-CoV-2-infected patients in a nosocomial outbreak.4 The timeframe of 15 minutes for the definition of close contact is arbitrary, and based mainly on the mechanism of droplet transmission. When classifying close contact and non-close contact, not only proximity between index and contacts and the duration of exposure, but other factors should be considered; the symptoms of the index, aerosol-generating acts such as coughing and singing, environmental factors such as crowding, adequacy of ventilation, indoor or outdoor setting, size of the indoor space, and PPE. There is growing evidence for airborne transmission of SARS-CoV-2,5678910 and missed non-close contact may result in subsequent transmission because of the nature of pre-symptomatic transmission.111213 Therefore, revision of the definition of close contact taking into account the nature of airborne transmission may be needed. Taken together, the definition of the close contact based on time duration and distance between individuals is not sufficient to identify contacts at risk. World Health Organization suggested separate ways to identify contacts in different settings and added ‘other situations as indicated by local assessments' in addition to a close contact.14 It is worth noting that contact tracing should be flexibly performed rather than stick to defined close contacts because no definition could be perfect. In addition, secondary case among non-close contact is problematic especially in HCWs, because they continue working after exposure and they can make further contacts to other HCWs and patients. In our study, five of 10 non-close contact (Supplementary Table 2 – A, B, D, H, and J) had worked after epidemiologic investigation, then diagnosed as COVID-19 later resulting additional contacts. However, work restriction for all non-closed contact is impossible due to staff shortage. Based on our results, we have taken into account for various factors including the space size, the adequacy of ventilation, and cycle threshold value of index patient when classifying the close contact and non-close contact with/without work restriction. In addition, close monitoring for symptom development, and frequent testing regardless of symptoms during incubation period in non-close contacts is needed.
Some may argue that transmission occurred via fomites in the 2 cases that entered a space after the index had left. However, the risk of surface transmission via fomites is considered to be low.15 In the case of I, the patient entered a small shower room where the ventilation system was not functioning adequately. In the case of J, staff changed the linen in the six-patient room; however, all other close contacts of the index in the hospital and family, and other contacts of the staff, had negative SARS-CoV-2 test. We believe that transmission occurred via virus lingering in the air or during the changing of bed linen; however, the possibility that the patient acquired a virus with the identical whole genome sequence from the other index patient or from other known contacts with this index patient not revealed by CCTV and interview is not ruled out. Although transmission through surfaces is no thought to be a common way that virus spreads,15 it is difficult to determine the relative contributions of inhaled droplets or aerosols and contaminated surfaces in cases that shared spaces with index or that entered a space after the index had left. In addition, droplets and aerosols are generated as a continuum, not divided dichotomously, so the environment where the period of floating in the air could be prolonged would be important for transmissibility.
There are several limitations to our study. First, it is single-center study evaluating contacts involving nosocomial transmission, and the number of cases analyzed was small. To generalize our finding, multi-center and community-based studies are needed. Second, we could not perform WGS for all the index-contact pairs, because some specimens were unavailable as the patients were diagnosed outside the hospital. In addition, the association was demonstrated by WGS in only three out of 10 cases (Supplementary Table 2). Therefore, the secondary cases in the study could be infected from other patients rather than from the presumed index cases. In addition, PPE use in the hospital might underestimate the transmission rate through close contacts. Third, the final decision on quarantine order for close contacts or non-close contacts by regional government epidemiologic investigators was subject to a certain epidemiologic situation (i.e., the presence of multiple- or super-spread events and the time from the symptom onset to the isolation), the nature of the essentialness of the HCW's job, and the viral load (Ct value) of the index patients. So, the quarantine policy in our hospital had changed over time, although the definition of close contacts did not change during the study period. In addition, the proportion of secondary cases initially classified as non-close contact may change depending on policy change or experience for SARS-CoV-2 transmission dynamics. As we shown in Supplementary Fig. 1, the secondary attack rate among non-close contacts was lower in 1st wave than the period thereafter. It may be associated with the policy or limited experience on SARS-CoV-2 outbreak during the early period of pandemic when there was an uncertainty of SARS-CoV-2 transmission characteristics. Finally, as the variant have been emerged, the proportion of secondary cases among non-close contact might also change. The study period was before the alpha and delta variants circulate in Korea.16 Alpha and delta variants have evolved to be more transmissible, and CDC recently reported that delta variant is as contagious as chickenpox.17 It should be determined whether secondary cases initially classified as non-close contact might increase if delta variant circulates dominantly. Further studies are needed in the era of dominancy of different variants.
In conclusion, at least one quarter of SARS-CoV-2 transmission events in a hospital occurred between non-close contacts. The definition of close contact for SARS-CoV-2 exposure based on droplet transmission should be revised to reflect the frequently airborne nature of SARS-CoV-2 transmission.
 XML Download
XML Download