

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Central precocious puberty (CPP) refers to the gonadotropin-dependent onset of puberty before the age of 8 years in girls.1 CPP is caused by the premature reactivation of the hypothalamic-pituitary-gonadal axis (HPG axis).2 Gonadal stimulation by gonadotropin induces an increase in sex steroid secretion that leads to the premature onset of sexual characteristics and is associated with a growth spurt and accelerated skeletal maturation that compromises adult height.3
Synthetic gonadotropin-releasing hormone (GnRH) analogues are the treatment of choice for CPP. These drugs suppress gonadotropin secretion through the desensitization and downregulation of GnRH receptors by exposing them to continuous rather than pulsatile GnRH release, leading to the decrease in gonadal steroid levels to prepubertal levels.45 GnRH analogues reverse or stabilize pubertal development, and growth is normalized without adversely affecting the resumption of puberty and the final height.67
The 1-month depot formulation of GnRH analogue is the primary formulation used in the treatment of CPP.4 It provides a steady release of the drug and significantly improves the short-and long-term outcomes in children affected by CPP without adverse effects during and after the treatment.489 A 3-month depot formulation of GnRH analogue has been developed, and short-term trials showed its efficacy in children with CPP.1011121314 However, a comparison of efficacy between the 1-month and 3-month depot formulations in suppressing the HPG axis has been rarely reported.14 One of the GnRH analogues, triptorelin, is available in depot formulations that can be injected every month or every 3 months and has been approved for use in patients with CPP in a number of countries throughout the world. Since CPP might require several years of treatment, the need for using the 3-month formulation is increasing to improve the treatment compliance and quality of life of children under treatment. Therefore, more data for the 3-month formulation to treat CPP are necessary to support the replacement of the 1-month formulation.
In this study, we analysed the outcomes in Korean girls with CPP treated with the triptorelin acetate (TA) 1-month depot (3.75 mg) or triptorelin pamoate (TP) 3-month depot (11.25 mg) to compare their efficacy in suppressing the HPG axis.
METHODS
Patients
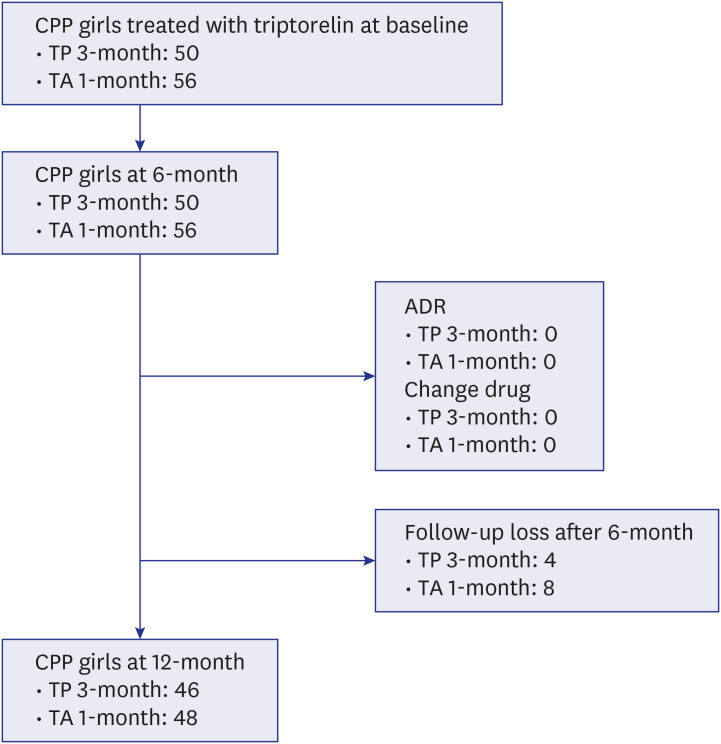
A retrospective analysis of the results of GnRH analogue therapy in 106 girls with idiopathic CPP during the period 2015 to 2019 at the pediatric endocrinology clinic of Korea University Hospital was performed. All patients had proven CPP based on the following criteria: breast development before the age of 8 and pubertal luteinizing hormone (LH) levels (peak LH level ≥ 5.0 IU/L) on a GnRH stimulation test (100 µg/m2 i.v.).1516 Additional inclusion criteria were CPP girls in under age 9 years at diagnosis, weight over 20kg, bone age (BA) advancement ≥ 1 year over chronological age (CA) by the Greulich-Pyle Method17 and naïve to GnRH analogue before initiating treatment with TP. We excluded the CPP girls with an identified etiology, such as growth hormone deficiency, brain tumor or cranial irradiation, and girls with any chronic diseases, such as chronic nephrosis, asthma, and epilepsy were excluded from the study (Fig. 1).
Methods
Among 106 girls, 50 were treated with the TP 3-month depot formulation (11.25 mg, TP 3-month group) and 56 were treated with the TA 1-month depot formulation (3.75 mg, TA 1-month group). The TP 3-month depot was administered every 3 months, and the TA 1-month depot was administered once a month by intramuscular injection. Triptorelin 3-month depot is recommended in patients over 20 kg without dose change. There is no information on dose reduction for under 20 kg or young children. We injected fixed one dose, 1 vial in patients over 20 kg for the treatment. Serum LH, follicle-stimulating hormone (FSH), and estradiol concentrations were measured after GnRH analogue injection every 6 months for therapeutic monitoring. LH and FSH were measured by the immunoradiometric (IRMA) kit (Beckman Coulter, CA, USA). The measurement range for LH was 0.16 to approximately 180 IU/L and FSH was 0.17 to approximately 180 IU/L. Estradiol was measure by radioimmunoassay kit (Cisbio Bioassays, Codolet, France), the mearuement range was 8 pg/mL to 5000 pg/mL. The single LH and FSH serum levels were measured 60 minutes after Triptorelin injection (Triptorelin-stimulated measurement). LH levels below 2.5 IU/L were considered adequate for HPG axis suppression (LH suppression).18
In both groups, the other assessments included height and weight (at baseline, 6 months, and 12 months), the calculated height velocity (at 6 months and 12 months), body mass index (BMI), and calculate the standard deviation score (SDS) of the height, weight, and BMI based on the 2017 Korean National Growth Charts for children and adolescents (at baseline, 6 months, and 12 months)19; pubertal development according to the Tanner stage (at baseline, 6 months, and 12 months); and BA determination by the Greulich-Pyle Method (at baseline, 6 months, and 12 months).20 BA divided by the CA (BA/CA) was used as an index of bone age advancement.
Statistical analysis
Statistical analysis was conducted using R statistical software (R for Windows V.3.5.1; The R Foundation for Statistical Computing, Vienna, Austria). Continuous variables were expressed as mean ± standard deviation. The differences in continuous variables between the two groups were evaluated using Student's t-test. Categorical variables were evaluated using the χ2 test instead. A P value of < 0.05 was considered statistically significant for all the tests.
RESULTS
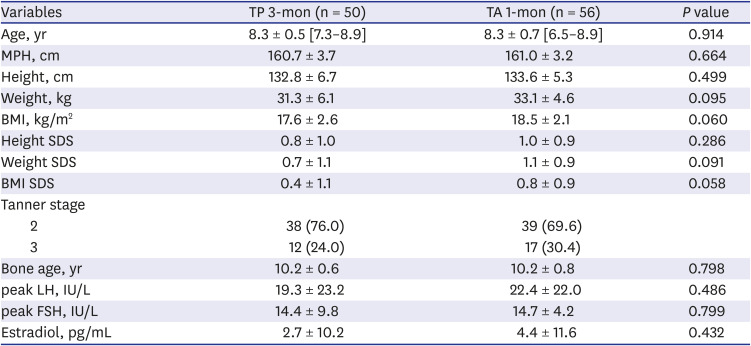
The baseline characteristics of patients in the TP 3-month and TA 1-month groups at the initiation of TP therapy in terms of age, weight, height, BMI, pubertal stage, bone age, peak LH level, and peak FSH level are outlined in Table 1. No significant differences were observed between the two groups in auxological and hormonal features (Table 1). The initial mean GnRH-stimulated peak LH levels were 19.3 ± 23.2 IU/L and 22.4 ± 22.0 IU/L (TP 3-month and TA 1-month, respectively), and the peak FSH levels were 14.4 ± 9.8 IU/L and 14.7 ± 4.2 IU/L (TP 3-month and TA 1-month, respectively) and the levels were not statistically different between the two groups (P = 0.486 and 0.799 respectively).
Table 1
Baseline characteristics of the TP 3-month depot and 1-month depot groups
Hormonal suppression
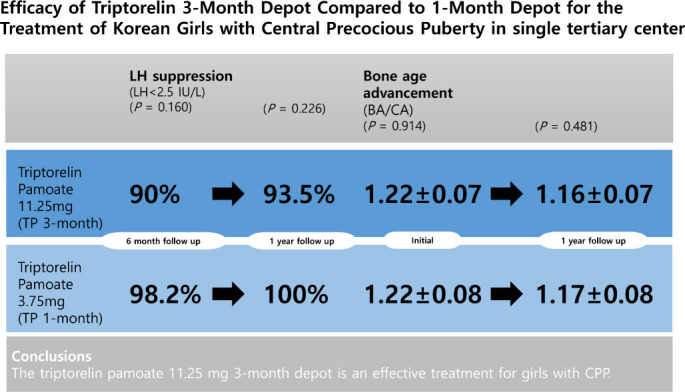
The TP 3-month group comprised 45/50 (90%) responders after 6 months and 43/46 (93.5%) after 12 months with an adequately suppressed LH response, and the TA 1-month group comprised 55/56 (98%) and 48/48 (100%) responders at 6 months and 12 months, respectively. The analysis at 12 months was conducted with the data of 46 patients in the TP 3-month group and 48 patients in the TA 1-month group due to follow-up loss. The proportion of responders did not show statistical differences between the TP 3-month and TA 1-month groups both after 6 months and 12 months (P = 0.160 and 0.226, respectively) (Table 2). Regarding the clinical characteristics of the patients who did not suppressed appropriately in 6 or 12 month after treatment with TP 3-month, there were no particular differences in Tanner stage, bone age, BMI and accompanying diseases compared to the responders of TP 3-month group.
Table 2
Suppressed LH responsea after treatment with TP 3-month and TA 1-month depots

| Variables | LH < 2.5 IU/L | ||
|---|---|---|---|
| TP 3-mon | TA 1-mon | P value | |
| 6 mon | 45/50 (90.0) | 55/56 (98.2) | 0.160 |
| 1 yr | 43/46 (93.5) | 48/48 (100) | 0.226 |
The mean Triptorelin-stimulated LH levels were 1.5 ± 1.3 IU/L (TP 3-month) and 0.8 ± 0.5 IU/L (TA 1-month) at 6 months (P < 0.001), and 1.2 ± 0.9 IU/L (TP 3-month) and 0.6 ± 0.3 IU/L (TA 1-month) at 12 months of treatment (P < 0.001). (Table 3).
Table 3
Mean LH and FSH levels after triptorelin injection (Triptorelin-stimulated response)

Clinical efficacy
The changes after 1 year of treatment were compared with the baseline in both groups. The Tanner stage was 2 or 3 in both groups and was evenly distributed at the beginning of the treatment. Assessment at 12 months showed that breast development was not progressed in both the TP 3-month and TA 1-month groups. During the treatment, height velocity decreased from 7.2 ± 2.2 cm/year to 6.2 ± 1.2 cm/year in the TP 3-month group and from 7.5 ± 4.2 cm/year to 5.6 ± 2.7 cm/year in the TA 1-month group after 6 months and 1 year of treatment, respectively. There were no statistically significant differences between the two groups (Table 4).
Table 4
Changes in height velocity and bone age advancement in girls at months 6 and 12 after treatment with the TP 3-month depot or TA 1-month depot
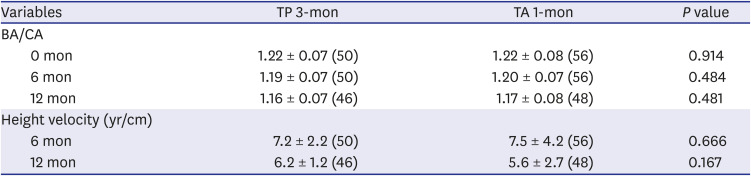
Bone age advancement was not significantly different between the two groups at any visit (Table 4). The degree of bone age advancement (BA/CA) decreased from 1.22 ± 0.07 and 1.22 ± 0.08 years at baseline (P = 0.914) to 1.16 ± 0.07 and 1.17 ± 0.08 years after 1 year in patients treated with the 3-month and 1-month depots, respectively (P = 0.481) (Table 4).
DISCISSION
Until now, the 1-month (4-week) depot GnRH analogues were most frequently used as the treatment of choice for CPP. However, a 3-month depot has become available over the past 10 years. Triptorelin is a long-acting GnRH analogue for the standard treatment of CPP.4222324 Triptorelin is available as an acetate salt and a pamoate salt. The acetate salt was used in the first formulation of triptorelin and pamoate salt is used to enable slow-release formulations of pharmaceutical agents having physicochemical properties suitable for sustained release.272829 The efficacy of the 3-month depot has been proven; however, most studies were performed on a too small scale or over a short-term and were not comparative studies.101112 Comparative studies between the Triptorelin 3-month and 1-month depots for the treatment of CPP are scarce.2122 Hence, we assessed the efficacy of the TP 3-month (11.25 mg) depot compared with that of the TA 1-month (3.75 mg) depot in suppressing the gonadotropin secretion in patients with CPP for the first time in Korea. We demonstrated that the efficacy of the TP 3-month depot was similar to that of the TA 1-month depot. Stimulated LH levels declined approximately one-tenth of the baseline levels until the first follow-up (at 6 months) and were sustained for 1 year in both groups. BA advancement and height velocity were suppressed at 1 year of treatment.
The criteria for the biochemical efficacy of adequate LH suppression during GnRH analogue therapy are controversial. The HPG axis can be evaluated by measuring unstimulated or stimulated (following GnRH analogue administration) serum LH, sex steroid, or urinary gonadotropin concentrations.232425262728 In one study, subcutaneous triptorelin (100 µg) was administered and the maximal LH response was noted after 60 minutes to confirm the diagnosis of CPP. The amount of TP injected was much lower than that in our study.29 Triptorelin has a superagonist effect, wherein a single injection of 1 µg of triptorelin per kg of body weight induces approximately a 10-fold release of LH relative to the same dosage of a GnRH analogue9. Therefore, stimulated serum LH levels following triptorelin administration could be used for monitoring the suppression of the HPG axis by administering leuprolide, another formulation of GnRH analogue using for CPP treatment.1726 In previous studies, the range of mean GnRH-stimulated peak LH level was from 0.97 ± 0.12 IU/L to 1.7 ± 3.2 IU/L during the first 12 months of treatment with triptorelin 11.25 mg, which was similar to the results of our study.1011 The cut-off value for therapeutic monitoring of LH suppression has been studied with GnRH analogue-stimulated LH levels; however, the appropriate value is still controversial.18303132 In this study, we used the LH level below 2.5 IU/L as the cut-off value for LH suppression based on a study with a Korean population.18
Our study showed that a significant reduction in LH levels after TP 3-month treatment compared to baseline levels, which is consistent with results from previous studies with triptorelin.10113334 Although the mean Triptorelin-stimulated LH level was higher in the TP 3-month group than in the TA 1-month group after therapeutic depot injection, the number of patients who showed lower than the LH suppression level (LH < 2.5 IU/L) was not significantly different between the two groups. Other studies with the triptorelin 3-month depot showed a similar decrease of LH and FSH levels after 6 months and 1 year of treatment. Recently, a study by Zenaty et al.34 showed that the peak LH level after 6 months of treatment with the triptorelin 3-month depot was 1.4 IU/L, which is slightly higher than 1.1 IU/L, the level of triptorelin 1-month depot and this is consistent with our study results. Although the clinical effects of two formulation were fairly equal, mean Triptorelin-stimulated LH level in the TP 3-month group showed higher than in the TA 1-month group. Further studies are needed on the long-term effects of mean LH level and its effects on prognosis.
FSH levels also significantly reduced after treatment and the mean FSH levels were slightly higher in the TP 3-month group than in the TA 1-month group, which is consistent with the results of other studies. In the study by Carel et al.11, the peak FSH levels were 1.7 ± 1.1 IU/L at 6 months and 2.2 ± 1.9 IU/L at 1 year of treatment.
We also evaluated the clinical efficacy of the triptorelin 3-month depot regarding the height velocity and bone age advancement. Height velocity tended to decrease between 6 months and 12 months of treatment in both groups, with no significant difference between the groups. This result was consistent with those of previous studies. Carel et al.11 reported that height velocity decreased from the baseline 9.0 ± 2.3 to 6.2 ± 1.7 cm/year and Chiocca et al.10 also showed that the height velocity decreased to prepubertal levels after 12 months of treatment. Bone age advancement also decreased in both groups after 1 year of treatment with no significant difference between the groups, which indicates that both treatments had adequate clinical efficacy. Two previous studies reported suppressed bone maturity after 1 year of triptorelin 3-month (11.25 mg) depot injection; one showed unchanged bone age with chronological difference11 and the other showed slightly decreased bone age after 1 year of treatment.10
The results of this study have several limitations. First, this is a retrospective study in single tertiary center. Consequently, our data may be limited by selection bias using record review and relatively small number of the cases included in the study. Second, it was conducted over a short period. Twelve months of duration only partially represents the entire treatment period. Further studies are necessary until the treatment is completed and the reproductive axis has recovered. Finally, the study recruited only girls with CPP, and boys were excluded. The efficacy study of triptorelin 3-month (11.25 mg) depot treatment for boys with CPP is also needed to determine the suppression of the HPG axis in both sexes.
In conclusion, the results of the present study demonstrate that the TP 3-month depot formulation effectively suppresses the progression of CPP in children with both hormonal suppression and clinical efficacy similar to that seen with the TA 1-month depot formulation. We suggest that the TP 3-month depot as well as TA 1-month depot can be used for the management of CPP.
 XML Download
XML Download