

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Bronchiectasis is a chronic respiratory disease characterized by the permanent dilatation of bronchi and impairment of mucociliary clearance of bronchial secretions, which consequently lead to the clinical syndrome of cough, increased sputum production, and recurrent respiratory infection.1 Approximately half of the patients with bronchiectasis experience exacerbations twice or more every year, which are characterized by the acute deterioration of respiratory and/or systemic symptoms that necessitate changes in treatment modalities and even lead to hospital admission.23 Preventing the exacerbation is a key target in the management of bronchiectasis because it is associated with increased airway inflammation, progressive lung damage, poor quality of life, and even mortality.45
Although the causes of bronchiectasis exacerbations are not known, bacterial infection is well known as one of the most important risk factors for frequent exacerbations and hospitalizations. However, there are still many patients who experience exacerbations without evidence of bacterial infection. Hence, recent studies have examined other etiologies for exacerbations, such as viruses and air pollution.678 Gao et al.8 first reported a higher prevalence of viral infections during exacerbations, as compared with during the steady state, in patients with bronchiectasis. Also, a recent pilot study investigating the incidence rate of respiratory viruses in patients with bronchiectasis revealed that only 28% of patients with exacerbations had viral polymerase chain reaction (PCR) performed on admission, with 39% (9/23) of those tests being positive for a respiratory virus, whereas a bacterial and fungal culture was performed in 88% of admissions, with 30% positive results.7
Due to the relatively low level of concern and awareness of viral etiologies in acute exacerbations of bronchiectasis, no studies have investigated the incidence rate and distribution of viral pathogens in a large number of patients. Therefore, we aimed to assess the rate of viral detection in acute exacerbations of bronchiectasis, and the clinical factors associated with viral detection.
Go to : 
METHODS
Study design and approval
We performed a retrospective, single-center study to assess viral infections in acute exacerbations of bronchiectasis.
Study subjects
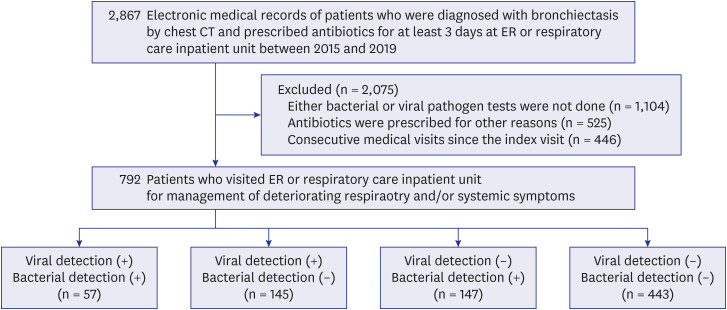
The patients were diagnosed with bronchiectasis by chest computerized tomography, but did not have a past medical history of interstitial lung disease. In Asan Medical Center, which is a 2,700-bed referral hospital in Seoul, South Korea, we selected 2,867 medical visits that included records of antibiotic prescription for more than 3 days following admission to a respiratory care inpatient unit or emergency room between 2015 and 2019. After excluding cases: 1) that did not include diagnostic tests for bacterial and viral pathogens, 2) in which antibiotics were prescribed for reasons other than acute exacerbation of bronchiectasis, and 3) where admission was not during the first medical visit for deteriorating symptoms, 792 patients were included for analysis (Fig. 1).
Definition of exacerbation
In the present study, acute exacerbation of bronchiectasis was defined as deterioration of two or more of the following symptoms,2 including at least one respiratory symptom, for at least 48 hours: 1) cough, 2) sputum volume and/or consistency, 3) sputum purulence, 4) breathlessness and/or exercise tolerance, 5) fatigue and/or malaise, 6) hemoptysis, and 7) fever, regardless of the presence of pneumonia.
Microbiological examination
A diagnostic test for viral identification, multiplex reverse-transcription PCR, was performed on all study subjects using a nasopharyngeal swab specimen or bronchoalveolar lavage (BAL) fluid to detect influenza viruses, respiratory syncytial virus (RSV), adenovirus, human metapneumovirus, parainfluenza virus types 1 to 4, enterovirus, rhinovirus, human coronavirus OC43/HKU1, human coronavirus 229E, human coronavirus NL63, and bocavirus using Anyplex RV16 (Seegene Inc., Seoul, Korea) between January 2015 and November 2018 and Allplex RP (Seegene Inc.) between December 2018 and December 2019. In cases where BAL was conducted, we additionally included shell viral culture for influenza virus, parainfluenza virus, RSV, cytomegalovirus, and adenovirus (Diagnostic Hybrids, Inc., Athens, OH, USA).
Diagnostic tests for bacterial pathogens were performed by gram staining and culture of either expectorated sputum or lower respiratory tract specimens in all study subjects. In applicable cases, the results of diagnostic tests, including a Binax NOW™ urinary antigen test for Streptococcus pneumoniae and Legionella pneumophila serogroup 1 (Binax Inc., Portland, ME, USA) and PCR for Mycoplasma pneumoniae, Chlamydia pneumoniae, and L. pneumophila using Seeplex PneumoBacter assay (Seegene Inc.) between January 2015 and August 2015 and AmpliSens® for M. pneumoniae, Chlamydophila pneumoniae, and L. pneumophila-FRT (InterLabService Inc., Moscow, Russia) between September 2015 and December 2019, were also included in the analysis. In cases where BAL was conducted, gram staining and culture of BAL fluid were incorporated. Sputum adequacy was determined based on the Murray and Washington's grading system, and sputum specimens of grades 4 to 6 were considered acceptable in the present study.9
Laboratory and pulmonary function tests
Data on laboratory findings were collected and reviewed, including white blood cell count, eosinophil count and C-reactive protein, as well as pulmonary function tests, including forced expiratory volume in 1 second. These data were obtained when the patients were in a non- exacerbated state between 2 years and at least 1 week before the beginning of the exacerbation.
Statistical analyses
All data are presented as means (± standard deviations) or medians (interquartile ranges) for continuous variables, and numbers (%) for categorical variables. Data were compared using Student t-tests or Mann-Whitney U tests for continuous variables, and χ2 or Fisher's exact tests for categorical variables. All tests were two-sided, and P values less than 0.05 were considered statistically significant. Multivariate regression analyses were used to calculate adjusted odds ratios (ORs) and 95% confidence intervals (CIs). Variables employed in the multivariate regression analyses were selected on the basis of a statistical significance level of less than 0.1 in the univariate analysis, together with the treatment duration. All data were analyzed using SPSS software (version 24.0; SPSS, Chicago, IL, USA).
Ethics statement
The study protocol was approved by the Institutional Review Board (IRB) of Asan Medical Center (IRB No. 2020-0397), which waived the requirement for informed consent because of the retrospective nature of the study.
Go to :
RESULTS
Characteristics of subjects
Our eligibility screening identified 792 patients with bronchiectasis who visited the emergency room or a respiratory care inpatient unit due to deteriorating respiratory and/or systemic symptoms and were prescribed antibiotics during the 5-year study period (Fig. 1). The median age of the 792 patients was 70.0 years, and 40.3% were female. Of the eligible patients, 172 (21.7%) had chronic obstructive pulmonary disease (COPD) and 72 (9.1%) had asthma as comorbidities (Table 1).
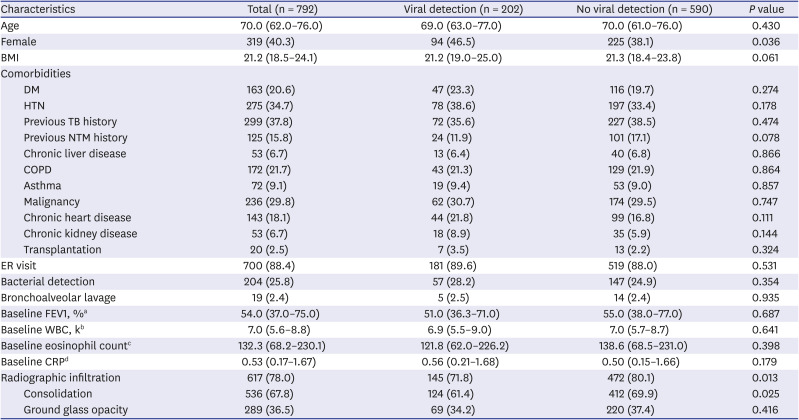
Table 1
Characteristics of 792 patients with bronchiectasis exacerbation
Values are presented as median (interquartile range) or number (%).
Of the 792 patients, bacterial pathogens were found in 204 (25.8%) patients. Among the patients in whom bacterial pathogens were identified, both bacteria and viruses were detected in 57 (27.9%) patients.
BMI = body mass index, DM = diabetes mellitus, HTN = hypertension, TB = tuberculosis, NTM = nontuberculous mycobacterium, COPD = chronic obstructive pulmonary disease, ER = emergency room, FEV1 = forced expiratory volume in 1 second, WBC = white blood cell, CRP = C-reactive protein.
aData on the baseline FEV1 were available for 363 patients; bData on the baseline WBC count were available for 585 patients; cData on the baseline eosinophil count were available for 583 patients; dData on the baseline CRP were available for 442 patients.
![]()
Overall, a viral pathogen was identified in 202 (25.5%) patients and a bacterial pathogen was identified in 204 (25.8%) patients. Among these, 57 (7.2%) patients were infected with both viral and bacterial pathogens (Table 1).
Microbiological examination
PCR to detect respiratory viruses was performed with nasopharyngeal swab specimens in 788 patients (99.5%), whereas BAL fluid was used in 19 patients (2.3%). Both specimens were used in 15 patients (1.9%).
For gram staining and culture, expectorated sputum was submitted by 780 patients (98.5%), and 54.2% of the expectorated sputum specimens had acceptable sputum quality. However, lower respiratory tract specimens were obtained from 107 patients (13.5%), and 84.1% were of acceptable quality.
The urinary antigen tests for S. pneumoniae and L. pneumophila serogroup 1 were performed in 684 (86.4%) and 549 patients (69.3%), respectively. PCR for M. pneumoniae and C. pneumoniae was performed in 320 patients (40.4%), while PCR for L. pneumophila was performed in 306 patients (38.6%).
Viral pathogens and seasonality
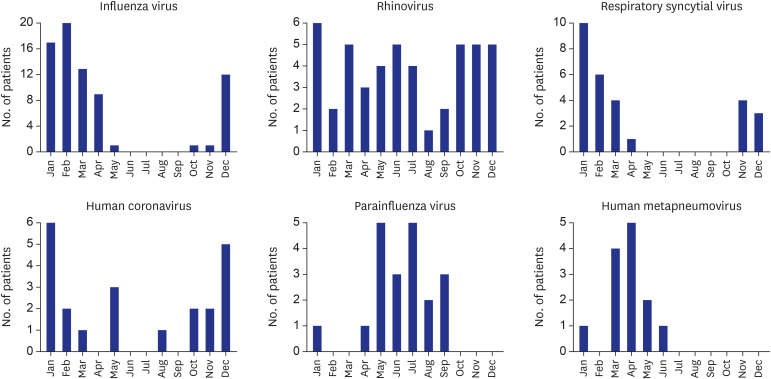
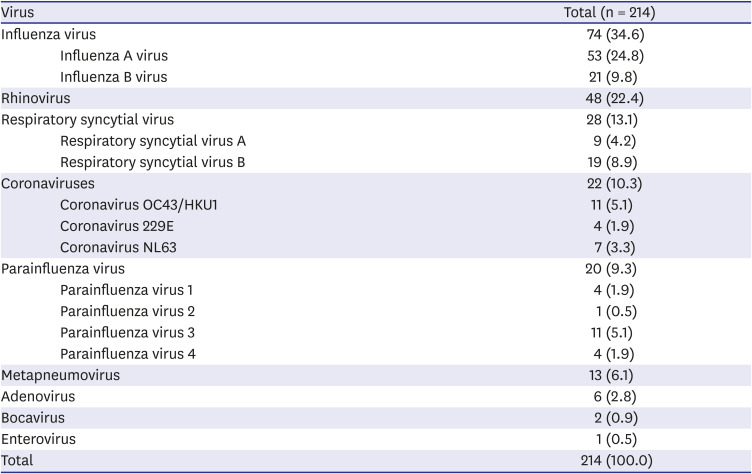
Table 2 and Fig. 2 show the proportions and seasonal distributions of the viral pathogens detected in patients whose exacerbations were due to viral infection. The most common viral pathogen isolated was influenza A virus (24.8%), followed by rhinovirus (22.4%), influenza B virus (9.8%), RSV B (8.9%), and human metapneumovirus (6.1%).
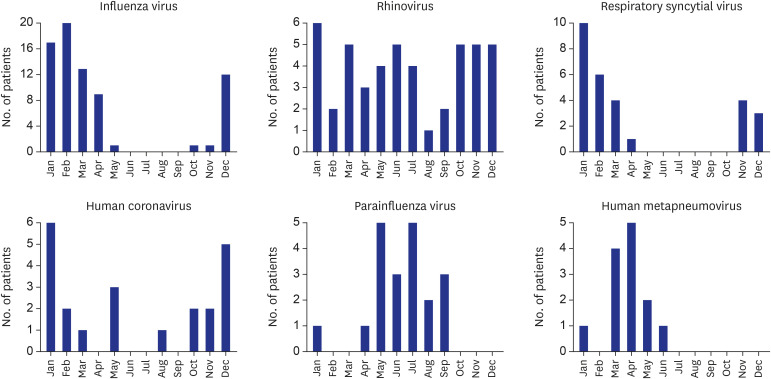 | Fig. 2Seasonal distribution of viral pathogens detected in patients with acute exacerbation of bronchiectasis. Adenovirus, bocavirus, and enterovirus were excluded because the number of cases detected was less than 10.
|
Table 2
Viral pathogens detected in patients with acute exacerbation of bronchiectasis
![]()
Factors associated with viral infection in acute exacerbation of bronchiectasis
After excluding patients with evidence of bacterial detection to eliminate the effect of bacterial pathogens on exacerbation, we compared the characteristics of patients who experienced acute exacerbation with viral detection with those of patients who did not have any evidence of an infectious trigger (Table 3). In patients with acute exacerbation of bronchiectasis without bacterial detection, viral pathogens were detected in 148 patients, although no pathogens were found in 451 patients. These two groups were comparable except in the proportion of female patients (47.3% in the “viral detection only” group vs. 37.3% in the “no identified infectious cause” group; P = 0.030), proportions with a past medical history of chronic heart disease (25.7% vs. 17.1%, respectively; P = 0.021), and presence of radiographic infiltration at presentation (72.3% vs. 81.3%, respectively; P = 0.019).
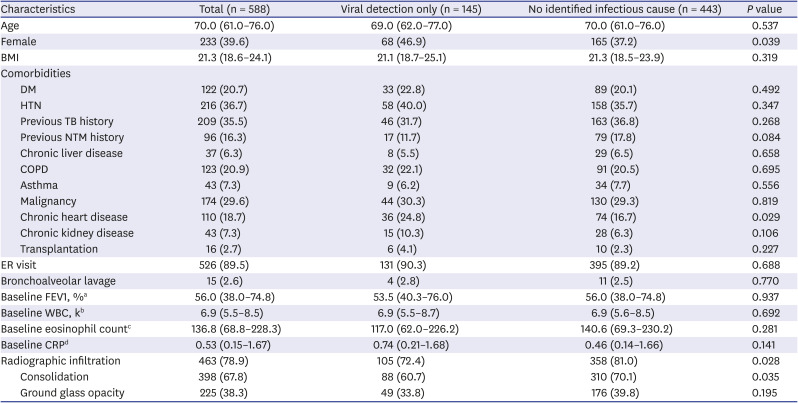
Table 3
Characteristics of the 588 patients with bronchiectasis exacerbation after excluding patients with detected bacterial pathogens
Values are presented as median (interquartile range) or number (%).
BMI = body mass index, DM = diabetes mellitus, HTN = hypertension, TB = tuberculosis, NTM = nontuberculous mycobacterium, COPD = chronic obstructive pulmonary disease, ER = emergency room, FEV1 = forced expiratory volume in 1 second, WBC = white blood cell, CRP = C-reactive protein.
aData on the baseline FEV1 were available for 264 patients; bData on the baseline WBC count were available for 430 patients; cData on the baseline eosinophil count were available for 429 patients; dData on the baseline CRP were available for 315 patients.
![]()
A multivariable analysis revealed that female sex (adjusted OR, 1.608; 95% CI, 1.094–2.363; P = 0.016) and chronic heart disease as a comorbidity (adjusted OR, 1.723; 95% CI, 1.096–2.708; P = 0.018) were positively associated with viral detection in acute exacerbation in patients with bronchiectasis, whereas the presence of radiographic infiltration (adjusted OR, 0.612; 95% CI, 0.395–0.948; P = 0.028) was negatively associated (Table 4).

Table 4
Analysis of factors related to viral detection in patients with acute exacerbation of bronchiectasis
The analysis was conducted in 588 patients after excluding the patients with bacterial pathogens.
OR = odds ratio, CI = confidence interval, NTM = nontuberculous mycobacterium.
![]()
Go to :
DISCUSSION
Acute exacerbation is a part of the natural course of bronchiectasis and, at the same time, is one of the most important prognostic factors of the disease.45 Bacterial infection, especially by Pseudomonas aeruginosa, is a well-established risk factor for developing exacerbations in patients with bronchiectasis; therefore, guidelines recommend using antibiotics during the exacerbation period if the patient is a known colonizer of the pathogen and even recommend long-term antibiotic therapy during stable periods if the patient experiences frequent (three or more) exacerbations each year.110 However, it is apparent that not all exacerbations are solely attributable to bacterial infections.67 In our real-world practice, we have come across numerous exacerbation cases in which we could not specify the causative bacterial pathogens despite repeated bacterial tests, including cultures and various antigen or antibody tests. Sometimes, viral pathogens are detected instead. Until recently, there has been low interest in viral roles in bronchiectasis exacerbations, because of which there are insufficient data to evaluate this. To the best of our knowledge, this is the first study to investigate the incidence rate and seasonal distribution of viral infection in a large number of patients who presented with exacerbation of bronchiectasis. The most important finding of the present study was that a viral pathogen was detected in approximately 25% of patients who were prescribed antibiotics for acute exacerbation of bronchiectasis with no evidence of bacterial infection. Of the viruses detected, influenza viruses were the most common (34.7%), followed by rhinovirus (22.7%), and RSVs (13.0%).
When analyzed according to a monthly timeline, influenza viruses, RSVs and coronaviruses were more common in winter, while parainfluenza viruses and human metapneumovirus were prevalent in the summer and spring seasons, respectively. Rhinoviruses were detected all year round. The seasonal distribution patterns of respiratory viruses shown in the present study mostly correspond with those of earlier studies, although a slight difference was found in the case of human metapneumovirus, which showed a winter preponderance in another study.11121314 Various mechanisms underlying the seasonal variations of viral infections have been proposed in recent studies, including different meteorological factors, such as temperature and humidity, resulting from regional variations; differences in behavioral and environmental backgrounds; or the infectiveness of the virus itself.15161718
Exacerbations caused by respiratory viruses in patients with COPD and those with asthma are associated with more frequent and longer hospital stays, as well as a longer median symptom recovery time, when compared with nonviral exacerbations.192021 However, in bronchiectasis, the viral role in the severity of exacerbations remains unknown. One important prospective study that might give a hint to the viral role in bronchiectasis exacerbation was conducted by Gao et al.,8 and it revealed that viruses were more frequently detected and that markers of systemic and airway inflammation, such as serum interleukin-6, tumor necrosis factor alpha, and sputum interleukin 1 beta, were higher during exacerbation than during the steady state. This may suggest a viral role in triggering bronchiectasis exacerbations; however, further investigations are needed to understand the mechanisms underlying this.
One notable finding in the present study is that the proportion of patients with preexisting cardiovascular diseases—including congestive heart failure, cardiomyopathies, valvular heart disease, and coronary artery diseases—was significantly higher in cases of virus-positive exacerbations than in those of exacerbations with no identified infectious cause. Although no study has investigated this phenomenon in patients with bronchiectasis, some studies have reported high rates of underlying cardiac disease in patients with symptomatic RSV, influenza, and human metapneumovirus infections.2223 In addition, Mehta et al.24 reported in their post hoc analysis of patients with COPD that patients with preexisting congestive heart failure were significantly more likely to develop a symptomatic RSV infection than patients without congestive heart failure, which might suggest the possibility of an increased susceptibility to viral infections in patients with chronic heart disease.
However, we still could not specify the exact cause of exacerbation in a considerable number of patients (56.3%), which we labelled as having acute exacerbation with “no identified infectious cause.” The possible explanations for the deteriorating conditions in this group of patients could be heterogeneous, including air pollution, bleeding, and combined cardiovascular decompensation. However, some patients in this group could have had mycobacterial or fungal infections, as we did not routinely screen sputum acid-fast bacilli and set up fungal cultures as part of our initial evaluation of bronchiectasis exacerbations.
The present study has some limitations. First and most significantly, the study was conducted at a single referral center, with a non-randomized, retrospective design. Larger, prospective studies will be needed to confirm the prevalence of viral infections in bronchiectasis exacerbations and their role in developing exacerbations. Second, because we included only patients who were prescribed antibiotics and managed in the inpatient units and emergency room, a considerable number of patients with milder forms of acute exacerbations might have been excluded from this study, and this may have raised the severity level of the included patients. Third, due to the limitation of diagnostic tools, it is possible that the identified bacterial and viral pathogens are colonizers or contaminants rather than true pathogens. Additionally, the heterogeneous approach to microbiological examinations could have affected the viral and bacterial detection rates. Finally, in patients with underlying chronic heart disease, acute decompensated heart failure and pulmonary edema triggered by viral infection could have mimicked the respiratory symptoms and radiographic infiltration such as ground-glass opacity observed in the acute exacerbations of bronchiectasis. This might have affected the result of multivariable analysis in the present study.
In conclusion, we found that a viral pathogen was detected in approximately one-fourth of patients with acute exacerbation of bronchiectasis. Of the viruses detected, influenza viruses were the most common, followed by rhinovirus and RSVs. Larger, prospective studies to confirm this are needed, as well as more attention to viruses as causative pathogens for acute, deteriorating symptoms in patients with bronchiectasis.
Go to :
 XML Download
XML Download