

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Providing appropriate sedation to pediatric patients in the emergency department (ED) is essential but requires caution.123 Pediatric sedation, particularly in younger patients, can create difficulties in maintaining airways when compared with adults and poses a higher risk of adverse events related to sedative use.45 Moreover, sedation in the ED is performed unexpectedly, associated with more painful procedures, and is more time-sensitive than scheduled sedation outside the ED.6 Accordingly, it is crucial to select sedatives with fewer adverse events while considering the purpose of sedation, patient age, and procedure duration in the ED.78
Chloral hydrate (CH) remains in use as a sedative for pediatric patients in Korea because of its convenient oral administration. However, it is no longer available in the United States because of safety concerns.9101112 Cases with serious adverse events, including mortalities, have been associated with medication errors or prolonged sedation up to 24 hours. Therefore, CH is thought to be inappropriate for ED use.131415 Additionally, CH has no analgesic effects and frequently causes sedation failure among pediatric patients > 3 years of age.1014 For these reasons, the Korean guidelines for pediatric procedural sedation and analgesia released by the Korean Society of Pediatric Emergency Medicine in 2012 recommended less primary use of CH and proactive use of ketamine for painful procedures performed in the ED.16
In this context, it is necessary to explore the trends in pediatric sedation in Korean EDs. This study aimed to investigate the characteristics of patients and sedatives used in the ED and their changes over 12 years. We used a nationwide population database to ensure comprehensive understanding and coverage of the wide variations in pediatric sedation in the ED across institutions and disparate physicians.1017
METHODS
Study design
We conducted a nationwide population-based retrospective study among pediatric patients aged ≤ 15 years who received sedatives in the ED and were discharged during 2007–2018. Patients were identified using the Korean Health Insurance Review and Assessment Service (HIRA) database after an appropriate access approval. HIRA is a major organization involved in the Korean government-run national healthcare system that reviews and collects medical claims data generated from healthcare provider reimbursements.18 This healthcare system covers approximately 98% of the over 50 million population of Korea and contains patient information, diagnosis, healthcare provider information, and treatment details in a structured form (Supplementary Table 1).18 Data extracted from the HIRA database are available to researchers on appropriate requests for public research.
The main outcomes of this study were: 1) patient characteristics and type of sedatives used each year and 2) their changes throughout the study period. Two categories of variables, patient characteristics (age, sex, ED level, and diagnosis) and type of sedatives used, were analyzed. We divided patients into 5 age groups: < 1 year, 1–3 years, 4–6 years, 7–10 years, and 11–15 years. ED level was categorized as regional emergency center, local emergency center/specialized care center (including advanced pediatric emergency center), and local emergency facility via search codes (Supplementary Table 2). HIRA uses the Korean Standard Classification of Disease Version 6 (KCD6), which is based on the International Classification of Diseases 10th Revision (ICD-10), for diagnostic information. Diagnosis of injury was established for codes S00–T98 and illness for other codes.18 Patients who initially visited the ED but were admitted to the inpatient unit were excluded because HIRA data does not distinguish whether sedation was administered during the ED stay or after inpatient unit admission. The sedatives were recorded using the drug classification codes provided by the Ministry of Health and Welfare of Korea (Supplementary Table 3). Opioids, such as morphine and fentanyl, were not included because they were predominantly used for analgesia, not sedation, in the ED. These data did not determine the number of times the same sedative was administered to a patient, and ≥ 2 different sedatives used in a patient were regarded as multiple.
Statistical analysis
Descriptive statistics are presented as numbers and percentages. Trend tests were used to investigate the changes in pediatric sedation over the years during the study period or by increasing patient age. All statistical analysis were performed using SAS Enterprise Guide Software version 7.1 (SAS Institute, Inc., Cary, NC, USA).
RESULTS
Patient characteristics
Patient demographic and sedation characteristics during the study period are summarized in Table 1. Sedation was performed in total 468,221 ED visits during 2007–2018. Proportion of sedation performed visits among annual ED visits of pediatric patients aged ≤ 15 years is provided. The number of annual ED visits could not be obtained during 2007–2008; therefore, we recorded 399,320 sedation performed visits, which were at least 3.81% of overall ED visits of pediatric patients during 2009–2018. The main features of the patients were 1–3 years of age (71.0%), male (64.0%), and underwent sedation at a local emergency center/specialized care center (65.2%) for diagnoses related to injury (93.5%). An increase in sedation use over time was observed in patients 4–6 years of age (from 13.8% to 21.8%) when compared with patients 1–3 years of age (from 71.0% to 66.4%). Additionally, sedation use increased in the regional emergency centers (from 32.2% to 40.9%) when compared with local emergency facilities (from 9.1% to 2.1%) during the study period.
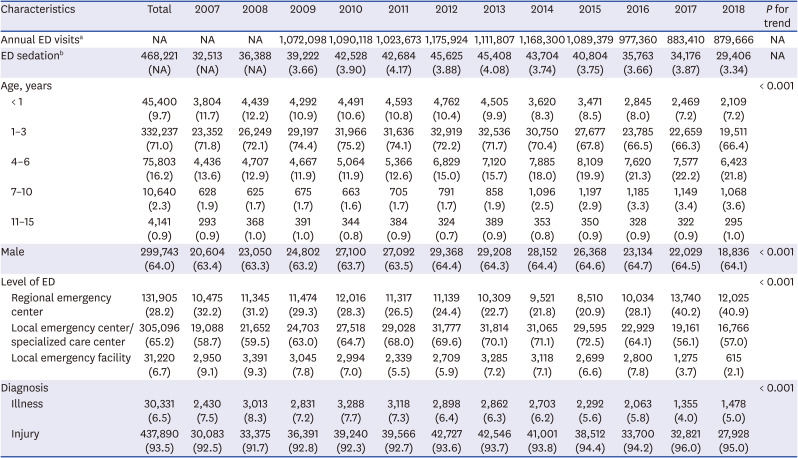
Table 1
Changes in patient characteristics
Values are presented as number (%).
ED = emergency department, NA = not applicable.
aNumber of annual ED visits of pediatric patients aged ≤ 15 years. Data in 2007 and 2008 could not be obtained; bNumber and proportion of sedation performed visits among annual ED visits.
![]()
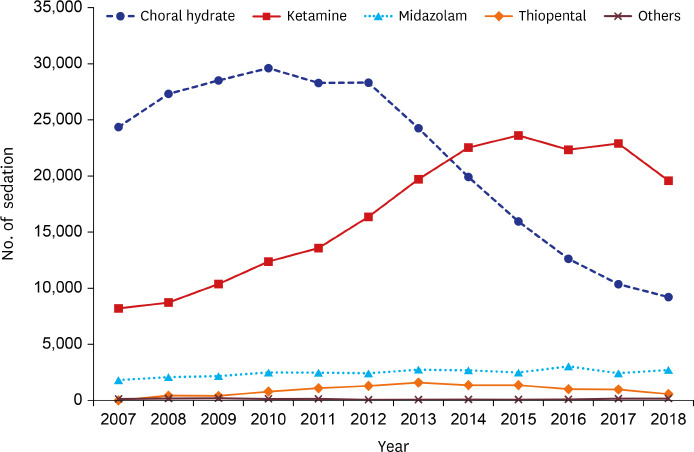
Changes in sedative use
CH (51.6%), ketamine (40.0%), and midazolam (5.9%) were the most common sedatives used in the ED during the study period. Thiopental, etomidate, propofol, and pentobarbital (2.5%) were used infrequently. Changes in sedative use are shown in Fig. 1; their specific numbers and proportions are provided in Supplementary Table 4. CH use gradually decreased from 70.6% in 2007 to 28.6% in 2018, whereas ketamine use increased from 23.8% in 2007 to 60.7% in 2018. Use of midazolam slightly increased from 5.2% in 2007 to 8.4% in 2018. These changes made ketamine the most used sedative since 2014. Furthermore, ketamine use steadily increased in all ED settings in all age groups; the increase was most prominent in 1–3 years and 4–6 years of age groups (Table 2). The decreased use of CH was prominent in patients < 1 year, 1–3 years, and 4–6 years of age (Supplementary Table 5).
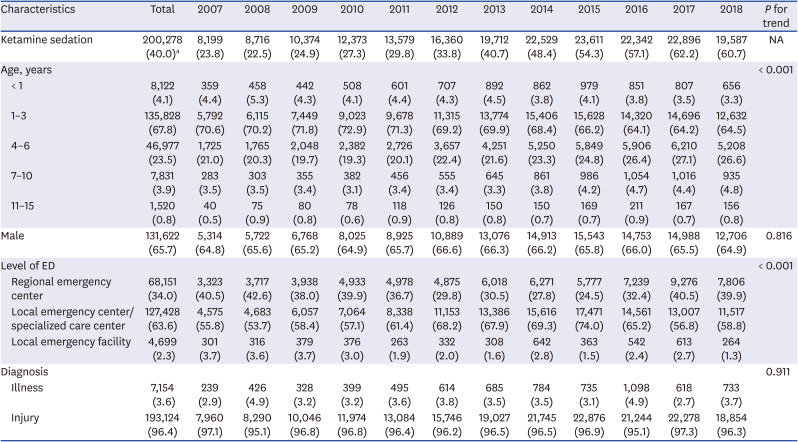
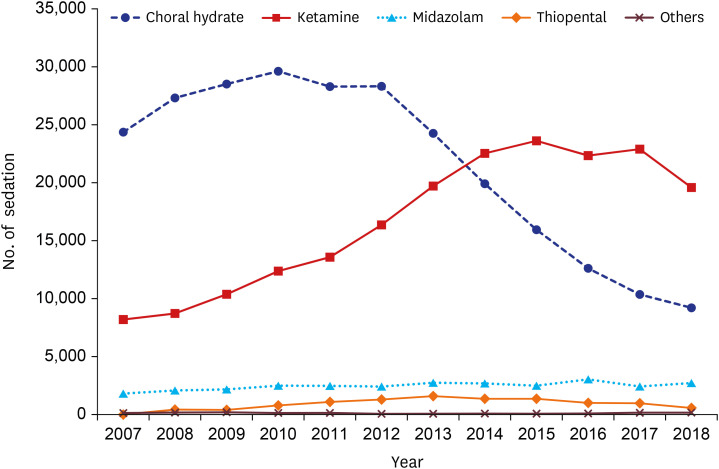
Table 2
Changes in ketamine use
Values are presented as number (%).
ED = emergency department, NA = not applicable.
aProportion of visits ketamine was used among total ED sedation.
![]()
Sedation characteristics by patient age groups
Sedation characteristics, including the type of sedatives used according to patient age groups, are provided in Table 3. The proportion of sedation decreased among patients aged ≥ 1 year and with increasing patient age (1–3 years, 71.0%; 4–6 years, 16.2%; 7–10 years 2.3%; 11–15 years, 0.9%). Patients aged < 1 year accounted for 9.7% of overall sedation and had a relatively considerable proportion of diagnoses related to illness (12.6%). The most used sedative over the study period was CH in patients aged ≤ 3 years (< 1 year, 74%; 1–3 years, 54.5%), ketamine in patients aged 4–10 years (4–6 years, 57.6%; 7–10 years, 67.0%), and midazolam in patients aged 11–15 years (42.8%). Multiple types of sedatives were used in 6.6% of all patients who underwent sedation, and this proportion increased with increasing patient age (< 1 year, 4.7%; 1–3 years, 6.6%; 4–6 years, 7.2%; 7–10 years 9.3%; 11–15 years, 0.9%; 11–15 years, 14.5%).
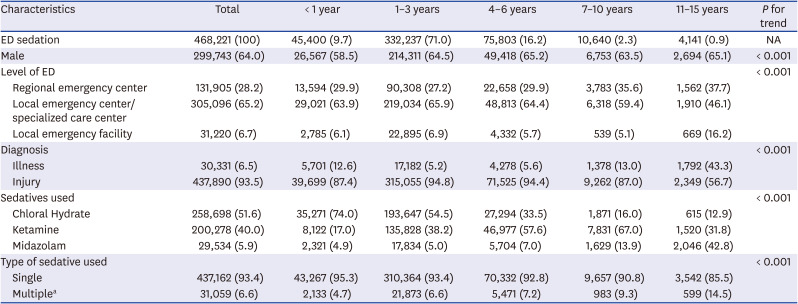
Table 3
Sedation characteristics according to patient age groups
Values are presented as number (%).
ED = emergency department, NA = not applicable.
aTwo or more of different sedatives used was regarded as multiple.
![]()
DISCUSSION
This nationwide population-based study explored approximately all cases of pediatric sedation performed at different levels of ED in Korea and demonstrated the characteristics of patients and changes in sedatives used during 2007–2018. The findings indicate that 1) pediatric sedation in the ED was performed mainly among patients aged 1–3 years for diagnoses related to injury; 2) the most commonly used sedative was ketamine, replacing the use of CH; and 3) the frequency of specific sedative use was dependent on age group over the study period (CH was more common in patients aged 1–3 years versus ketamine in patients aged 4–6 years). Notably, a decrease in CH use and increase in ketamine use among patients aged 4–6 years are considered plausible in compliance with the Korean guidelines for pediatric procedural sedation and analgesia.16
Pediatric sedation in the ED is widely accepted as a standard practice and is actively performed in Korea,1019 as evidenced by the many patients who underwent sedation during the study period. The proportion of pediatric sedation was at least 3.8% of overall ED visits during 2009–2018, which is comparable to the 1% reported by the Sedation Safety Study Group of Pediatric Emergency Research Canada.2 This previous study's data included sedation for painful procedures across 6 tertiary care pediatric EDs alone; therefore, our large-scale study, which included sedation for emergent diagnostic imaging, is more likely to reflect the overall proportion of pediatric sedation in the ED.20
Providing sedation for pediatric patients in the ED has become more systematic along with the development of pediatric emergency medicine over the last decade in Korea.21222324 This involves improvement in use of sedatives and changes in the level of ED which provide pediatric sedation. Most sedations were performed in the local emergency center/specialized care center or regional emergency center, whereas only 6.7% of sedation performed in the local emergency facility and this proportion has decreased (from 9.1% to 2.1%) during the study period. In addition, our results demonstrated increased use of ketamine and decreased use of CH. Ketamine was used most frequently among patients who were 4–6 years and 7–10 years of age, which seems reasonable due to the safety and efficiency of pediatric sedation in the ED. Ketamine is an effective sedative with safer characteristics compared with other sedatives; it preserves cardiovascular and respiratory stability due to its dissociative mechanism and sympathomimetic effects.725 Furthermore, it has a rapid onset time, relatively short-acting duration and brings early recovery.225
The Korean guidelines for pediatric procedural sedation and analgesia recommend selecting sedatives according to the purpose of sedation, patient age, and duration of the procedure.16 Ketamine use is increasingly prominent; therefore, detailed guidelines, such as specific practical situations, levels of ED, or administration methods, should be updated. Additionally, most pediatric sedation guidelines do not describe the use of multiple types of sedatives.4616 In several studies, the use of multiple types of sedatives has been reported to increase the risk for adverse events.21326 This study showed that increasing patient age was associated with the use of multiple types of sedatives; the reason for multiple sedative use or related adverse events in the older age groups could not be verified. Further research is required to stratify the risks associated with multiple sedative use among different age groups and this should be considered in the development of future guidelines.
This study has a few limitations owing to the characteristics of the HIRA database used. First, data for cases not covered by the national healthcare system, such as self-afflicted injuries or motor accidents, were excluded. Further, the use of emerging sedatives that were not eligible for reimbursement, such as dexmedetomidine, was not included. However, usage of such sedatives seems minimal among pediatric patients in Korean EDs. Second, only limited information could be accessed; the purpose of sedation, route of administration, and incidence of adverse events or sedation failure could not be identified. Moreover, it was indistinguishable how many times the same sedative was administered.
In conclusion, this first nationwide population-based study on pediatric sedation in Korean EDs demonstrated notable changes in the characteristics of patients and sedatives used. Advanced guidelines reflecting these changes are necessary. Furthermore, the establishment of a national pediatric sedation registry would be helpful to collect high-quality information to overcome the limitations of this study.
 XML Download
XML Download