

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Gout is the most common inflammatory arthritis in adults, and its prevalence and incidence are increasing worldwide.123 Gout is now considered a curable disease as its pathophysiology is well understood, early and accurate diagnosis is possible, and effective treatment drugs are available.456 Nevertheless, studies have shown that gout is still managed ineffectively, with the majority of patients still experiencing acute attacks, progressive joint damage, and disease-related complications.78 Owing to evidence-based guidelines published by international specialty societies in recent years, there has been a great improvement in the standard care of gout.591011 However, the treatment goal might not be met unless patients take efforts toward making lifestyle changes and adhere to prescribed urate lowering therapy (ULT). Recent meta-analyses revealed low overall adherence rates to ULT of 46–47% in patients with gout,1213 which is considered the lowest adherence rate to therapeutic drugs among chronic illnesses requiring maintenance therapy.14
Recent studies have shown the importance of patient perspectives and preferences for ULT adherence. Changes in perspectives through educational interventions have resulted in improved treatment adherence in patients with gout.1516 In contrast, distorted illness perceptions had negative effects on patients' attitudes toward gout management leading to poor treatment adherence.17 Therefore, clinical practice guidelines are now including patient perspectives and preferences as their values are likely to play critical roles in treatment decisions and adherence.181920 The American College of Rheumatology (ACR) treatment guideline for gout included patient panel recommendations and conducted an in-depth focus group meeting to better understand the values of patients with gout and to improve the decision-making process regarding treatment.21 However, there are limited studies exploring patients' perspectives and preferences about gout management, especially in different cultural and regional settings. Therefore, we investigated patients' perspectives and preferences regarding gout and gout management in Korea and their impacts on adherence to ULT.
Go to : 
METHODS
Study population and recruitment
Consecutive patients with physician-diagnosed gout visiting the rheumatology outpatient clinics of 16 tertiary hospitals were invited to participate in a brief paper-based survey from February 2020 to August 2020. Of 829 patients invited, 818 (98.7%) agreed to participate in the study.
Survey questions
The survey consisted of 20 questions regarding gout and gout management. We collected the following information from the participants: 1) age, sex, and body mass index; 2) disease duration; 3) comorbidities; 4) number of gout attacks in the past year; 5) current use of ULT; 6) ULT adherence; 7) use of alternative treatments; and 8) perspectives and preferences regarding gout and gout management. Surveys with a questionnaire response rate of less than 50% were excluded from the analysis. Of total 818 surveys collected, 9 were excluded due to inadequate response rate. Among all respondents, patients currently receiving ULT were classified into the following 2 groups according to ULT adherence: ULT adherence ≥ 80% group (number of days not taking ULT medication in the past 1 month was ≤ 5) and ULT adherence < 80% group (missed days of ULT were ≥ 6).
Statistical analysis
A descriptive analysis was performed to summarize the baseline characteristics of respondents. We used the Mann−Whitney test and χ2 test for comparing continuous and categorical variables between the two groups. Univariate analysis and multivariate logistic regression analysis were performed using ULT adherence as a dependent variable. Variables with a P value < 0.1 in the univariate analysis were included in the multivariate regression analysis (backward likelihood ratio method) to determine the factors associated with ULT adherence. All data were analyzed using IBM SPSS (version 22; IBM Corp., Armonk, NY, USA). A P value < 0.05 was considered statistically significant.
Ethics statement
This study was approved by the Institutional Review Board of all participating hospitals (Institutional Review Boards of Ewha Womans University Mokdong hospital [EUMC 2020-01-007-003], Gangneung Asan Hospital [2020-02-010], Gyeongsang National University Hospital [2020-02-016], Kyung Hee University Hospital [2020-06-079], Gil Medical Center [GAIRB 2020-0-47], Samsung Changwon Hospital [2020-02-002], Kangbuk Samsung Hospital [2020-01-012-001], Konkuk University Medical Center [2020-01-002], Samsung Medical Center [SMC 2019-12-162], Chonnam National University Hospital [CNUH-2020-046], Seoul St. Mary's Hospital [KC20QCDI0095], Kangwon National University Hospital [KNUH-2020-02-003-001], Asan Medical Center [2020-0068], Gyeongsang National University Changwon Hospital [GNUCH-2020-03-011], Chungnam National University Hospital [CNUH-2020-046], and Chung-Ang University Hospital [2020-001-411]), and was performed in accordance with the Declaration of Helsinki. Informed consent was obtained from the study participants.
Go to :
RESULTS
Characteristics of the subjects
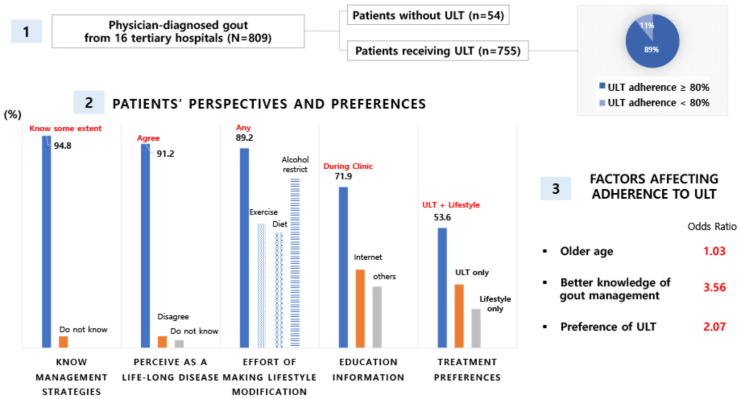
Table 1 shows the characteristics of 809 physician-diagnosed patients with gout who completed the survey. The mean [standard deviation] age was 53.5 [13.7] years, 97.6% of patients were male, and the mean [SD] disease duration was 8.2 [7.9] years. Comorbidities were detected in 67.7% of patients, with the most common comorbidity being hypertension (43.5% of patients), followed by dyslipidemia (27.2%). Although 755 (94.5%) of patients were receiving ULT, 57.7% experienced gout attacks in the past year and 13.3% experienced 4 or more attacks. Of those receiving ULT, 673 (89.1%) had a ULT adherence rate of ≥ 80% and 82 (10.9%) had a ULT adherence rate of < 80%. Febuxostat was prescribed in 41.5% of patients using ULT, followed by allopurinol (18.3%) and benzbromarone (2.0%), and 34.2% of patients replied that they did not know the name of the drug they were taking. Use of alternative treatments, including natural supplements and herbal remedies, was reported in 16.4% of patients.
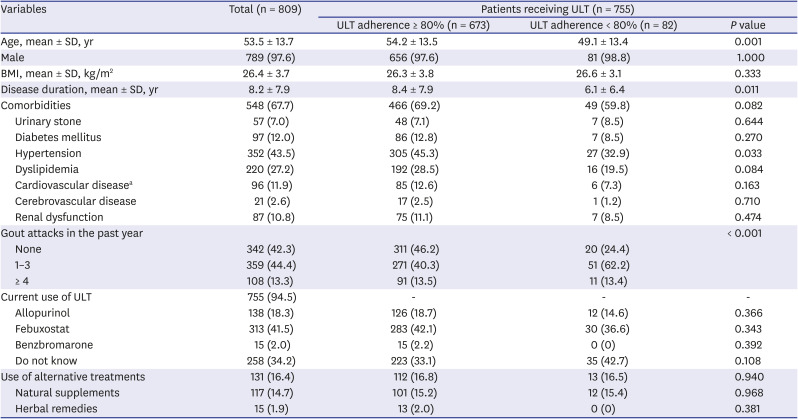
Table1
Characteristics of the subjects
Data are presented as number (%).
ULT = urate lowering therapy, SD = standard deviation, BMI = body mass index.
aIncludes ischemic heart disease, myocardial infarction, arrythmia, congestive heart failure.
![]()
Patients' perspectives and preferences regarding gout and gout management
A total of 94.8% of respondents answered that they acknowledged gout management strategies to some extent, and 91.2% of patients perceived gout as a life-long disease. Most patients (89.2%) were making efforts toward practicing at least one of the lifestyle modifications, including regular exercise, diet modification, and alcohol restriction. Restriction of alcohol intake, regular exercise, and dietary modification were practiced by 75.9%, 55.6%, and 51.6% of patients, respectively. Patients mainly obtained information on gout management during their clinic visit (71.9%), followed by internet searching (35.0%). Approximately half of the patients (53.6%) preferred managing their disease with both ULT and lifestyle modification, 28.4% preferred ULT only, and 17.4% preferred lifestyle modification only (Table 2).
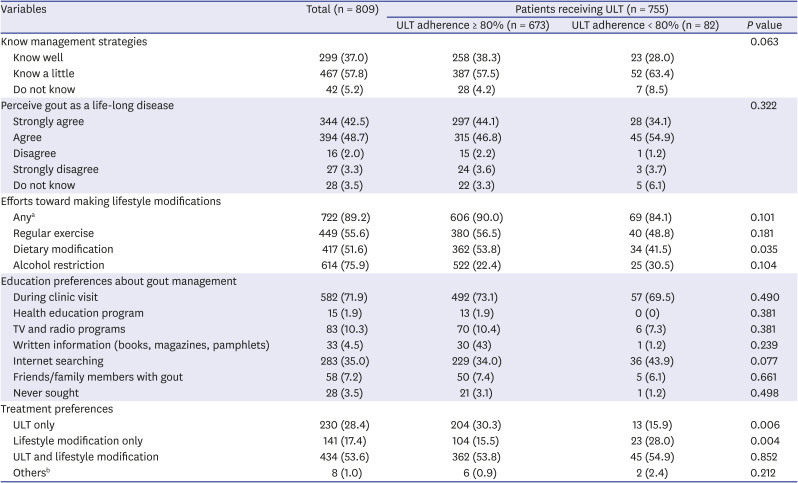
Table 2
Patients' perspectives and preferences regarding gout and gout management
Data are presented as number (%).
ULT = urate lowering therapy.
aPracticing at least one of regular exercise, dietary modification, and alcohol restriction; bOthers include natural supplements, herbal remedies, stress management, and joint injection.
![]()
Factors influencing adherence to ULT
Characteristics were compared between the group with ULT adherence ≥ 80% and the group with ULT adherence < 80% (Tables 1 and 2). On comparing the two groups, the group with ULT adherence ≥ 80% had a higher mean [SD] age (54.2 [13.5] vs. 49.1 [13.4] years, P = 0.001), a longer mean [SD] disease duration (8.4 [7.9] vs. 6.1 [6.4] years, P = 0.011), a higher prevalence of hypertension (45.3% vs. 32.9%, P = 0.033), and less gout attacks (P < 0.001). The group with ULT adherence ≥ 80% took more efforts toward making dietary modification compared with the group with ULT adherence < 80% (53.8% vs. 41.5%, P = 0.035). Regarding treatment preferences, the group with ULT adherence ≥ 80% preferred management of their disease with ULT only (30.3% vs. 15.9%, P = 0.006), while the group with adherence < 80% preferred management with lifestyle modification only (15.5% vs. 28.0%, P = 0.004).
Factors influencing ULT adherence were analyzed based on the results of the questionnaires (Tables 1 and 2). Univariate analysis showed that older age, longer disease duration, better acknowledgement of management strategies, practicing dietary modification, and preference for using ULT were associated with better adherence to ULT. In the multivariate analysis, older age (odds ratio [OR], 1.03, P = 0.002), better acknowledgment about gout management strategies (OR, 3.56, P = 0.011), and preference for using ULT (OR, 2.07, P = 0.007) were significantly associated with better ULT adherence (Table 3).

Table 3
Factors affecting adherence to ULT
![]()
Go to :
DISCUSSION
This is the first study to consider the perspectives and preferences of patients with gout and their impacts on adherence in Korea. We found that patients' perspectives and preferences about gout and its management had high impacts on adherence to ULT. Adherence was better in patients with older age, those with better knowledge of gout management strategies, and those who had preference for ULT.
We found that 94.5% of patients were using ULT, which is a much higher rate than 37.6% reported in a previous study performed in the United Kingdom (UK).8 In addition, the adherence rate to ULT in our study was much higher than that reported in previous studies. Our study demonstrated ULT adherence of ≥ 80% in 89.1% of patients receiving ULT, while previous studies reported adherence rates between 10% and 47%.12132223 High rates of ULT use and adherence found in our study could be related to 3 reasons. First, it could be due to the fact that our study only included patients receiving gout care from rheumatologists in tertiary centers, who had sufficient knowledge about gout and gout management. In a UK study showing a low rate of ULT use, gout was largely managed by general practitioners in primary care,8 who were mostly reluctant to offer ULT since they viewed gout as an acute condition and not as a chronic disease requiring life-long treatment.24 Second, the difference in practice patterns according to region might have influenced the rates of ULT use and adherence. Adherence rates to ULT were reported to be higher in studies performed in Asia (56%) compared with those performed in the United States of America (USA) (40%) and Europe (44%).13 Lastly, patients may have received sufficient information regarding the disease during their rheumatology clinic visits to form proper perceptions about gout and gout management which is important for their commitment to life-long care. This is reflected by the finding that most patients in our study reported that they received information about the disease during their clinic visits (71.9%), perceived gout as a life-long disease (91.2%), and were making efforts toward practicing at least one of the lifestyle modifications, including regular exercise, diet modification, and alcohol restriction (89.2%). It has been shown that distorted perception and lack of knowledge about the disease were major barriers for making adequate lifestyle changes and adhering to life-long ULT in patients with gout.72425 When appropriate and sufficient information about the disease is provided, patients with gout were shown to adhere to ULT for cure.2627
Although most of the patients were receiving ULT and adherence to medication in the recent 1 month was high, 57.7% of patients experienced gout attacks in the past year and 13.3% experienced 4 or more attacks in this study. This might be related with increased portion of patients not achieving the target uric acid level, relatively short period of time assessed for adherence, or short or interrupted duration of ULT in surveyed patients. As in previous study showing decreased incidence of gout attacks in a patient group achieving target uric acid level of < 6 mg/dL,28 we found in a sub-analysis of 50 gout patients receiving ULT that patients who had ULT adherence ≥ 80% had significantly lower uric acid level at the time of the survey compared with those who had ULT adherence < 80% (data not shown). Because of concerns for recall bias, adherence was assessed in only past 1 month, and duration of ULT was not included in the survey questionnaire. In addition, it may be due to the fact that although 94.8% of patients had some knowledge about the management strategies, only 37.0% knew the management strategies well. Continuous education has been shown to be important in improving adherence to ULT and preventing acute gout attacks. Nurse-led care that provides individualized education and engages patients in treat-to-target ULT resulted in achievement of the target uric acid level in 95% of patients at 2 years of follow-up.15
Education has been known to play an important role in determining patient preferences for gout management. In a study assessing patients' perspectives regarding gout and gout management, patients favored more active ULT after an in-depth panel discussion that informed about the 2020 ACR treatment guideline.21 We also found that the majority of patients treated by rheumatologists in Korea preferred ULT either alone or in combination with practicing lifestyle modification (82.0%) for the management of their disease. Treating rheumatologists' perspectives may have affected the patient preferences for ULT in this study. Rheumatologists are specialists who have expertise in treatment of gout. Rheumatologists view gout as a disease that should be managed by achieving treatment target, and reduction of urate below a treatment target is important for optimal outcome.6 This is in contrast to the result of a cross-sectional internet-based patient survey performed in the USA reporting that 40% of patients with gout preferred non-pharmacological interventions such as cherry extract and diet modification for gout management.29
Several factors have been suggested to influence ULT adherence. A Meta-analysis of 19 studies on medication adherence in patients with gout showed that older age, more comorbidities, and the presence of diabetes or hypertension were associated with better adherence.12 Older age may be associated with longer duration of the disease and more associated with comorbidities, thus, this may alert patients to better adhere to therapy to prevent further damage and complications related to the disease. In accordance with previous reports, we identified older age, longer disease duration, better knowledge of management strategies, practice of dietary modification, and preference for ULT as factors associated with better adherence to ULT. In the multivariate analysis, patients who had knowledge about management strategies and those who had preference for ULT were 3.6 times and 2.1 times more likely to have better adherence to ULT, respectively. This observation suggests that patients' perceptions and preferences regarding gout and gout management have great impacts on adherence to ULT.
Our study has some limitations. As it was based on patient-reported data, it was not possible to determine whether the patients in the good adherence group reached the actual target serum uric acid level. Education and economic levels could affect patients' perspectives and preferences, and also on adherence to ULT, but these variables were not considered in this study. Although the quality and quantity of provided education may vary among the participating centers, this difference was not accounted. Nevertheless, this is the first Korean study on patients' perspectives and preferences regarding gout and gout management, which can provide important evidence for therapeutic decision-making and development of regional clinical practice guidelines. As this study was performed in patients with gout receiving rheumatology care at tertiary hospitals, further research evaluating the perspectives and preferences of patients in other clinical settings is needed to fully understand the values of the patients.
In conclusion, a high number of patients with gout treated at rheumatology clinics perceived gout as a life-long disease and preferred treatment based on ULT. Perspectives and preferences of the patients had high impacts on adherence to ULT. Understanding patients' perspectives and preferences about gout and gout management appears to be valuable for achieving desired clinical outcomes in gout.
Go to :
 XML Download
XML Download