

 PDF
PDF Citation
Citation Print
Print



A 27-year-old male had a history of Kawasaki disease (KD) at 3 years of age, and had been continued on low dose aspirin due to a right coronary artery (RCA) aneurysm. At 8 years of age, he was referred for angiographic evaluation of coronary arteries due to intermittent chest tightness. A dipyridamole stress thallium 201 single-photon emission computed tomography (SPECT) showed a reversible perfusion defect in the inferior wall of the left ventricle (Figure 1A). Coronary angiography showed multiple aneurysms and severe stenosis at the proximal segment of RCA (Figure 2A and B, Supplementary Video 1). Initial balloon angioplasty was unsuccessful (Figure 2C). Intravenous ultrasound showed a severe luminal narrowing, aneurysms with calcifications, and intimal proliferations (Figure 3). Percutaneous transluminal coronary rotational ablation (PTCRA) was done with a 2.0 mm-sized burr, resulting in 30% residual narrowing in the target lesion (Figure 2D). Follow up SPECT at 6 months after PTCRA showed no perfusion defect (Figure 1B). At 20 years of age, coronary angiography demonstrated a restenosis of the target lesion (Figure 4A, Supplementary Video 2). Fractional flow reserve measurement was 0.66 (Figure 5), then a repeated PTCRA was done with a significant improvement (Figure 4B, Supplementary Videos 3 and 4). At present, the patient is 27 years old and doing well without any cardiovascular symptoms.
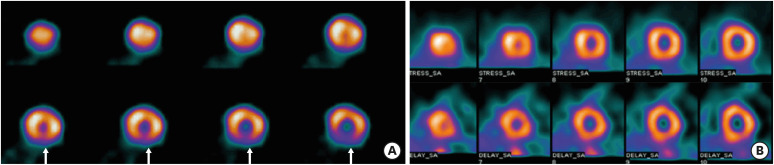 | Figure 1Dipyridamole stress thallium 201 SPECT at 8 years old showing a reversible perfusion defect (arrows) in the inferior wall of the left ventricle (A), and normal perfusion at 6 months after the PTCRA (B).PTCRA = percutaneous transluminal coronary rotational ablation; SPECT = single-photon emission computed tomography.
|
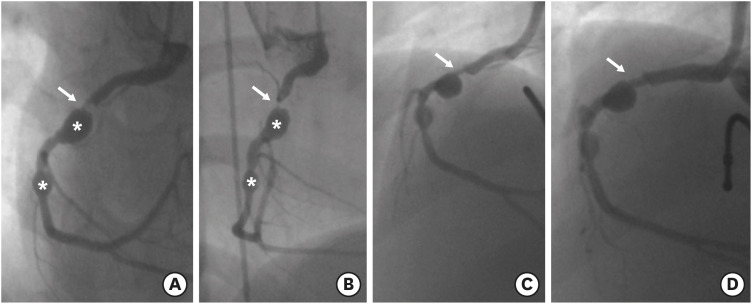 | Figure 2Coronary angiographies of RCA at 8 years of age, showing two coronary aneurysms (asterisks) and severe stenosis (>90% in diameter) at the proximal segment of the RCA (arrows) (A, B), a residual stenosis after coronary balloon angioplasty (C), and an improved coronary stenosis (arrow) after the PTCRA (D).PTCRA = percutaneous transluminal coronary rotational ablation; RCA = right coronary artery.
|
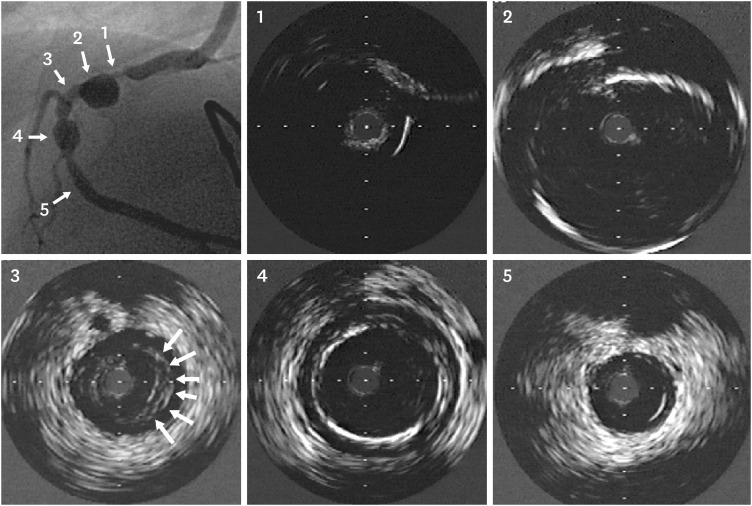 | Figure 3Intravenous ultrasound images before PTCRA at 8 years of age. Each numbered image corresponds to the sites indicated by numbers and arrows in the angiography image (far left and upper image). Severe stenosis and calcification (360°) (1), a huge aneurysm (about 7 mm in diameter), wall thickening, and calcifications (2), an intimal proliferation and thickening (arrows) (3), another aneurysm with calcification (4), and a nearly normal coronary artery (5) are demonstrated, all of which are unique characteristics of coronary artery lesions associated with Kawasaki disease.PTCRA = percutaneous transluminal coronary rotational ablation.
|
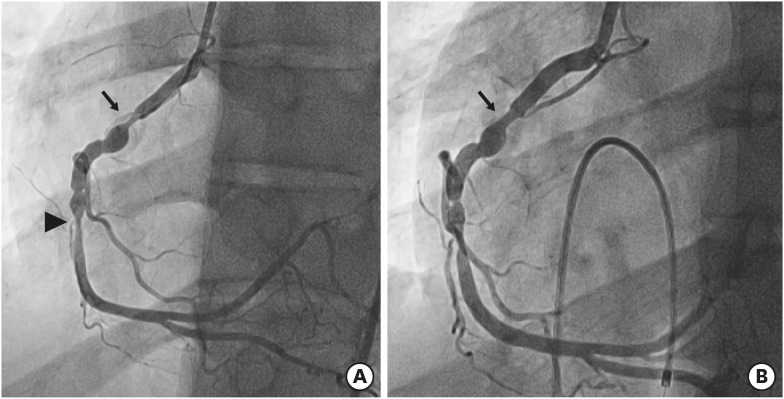 | Figure 4Coronary angiographies at 20 years of age (12 years after the first PTCRA), showing a restenosis of the target lesion (arrow) and another stenosis at the mid RCA (arrowhead) (A), and an improved target lesion stenosis after the second PTCRA (arrow) (B).PTCRA = percutaneous transluminal coronary rotational ablation; RCA = right coronary artery.
|
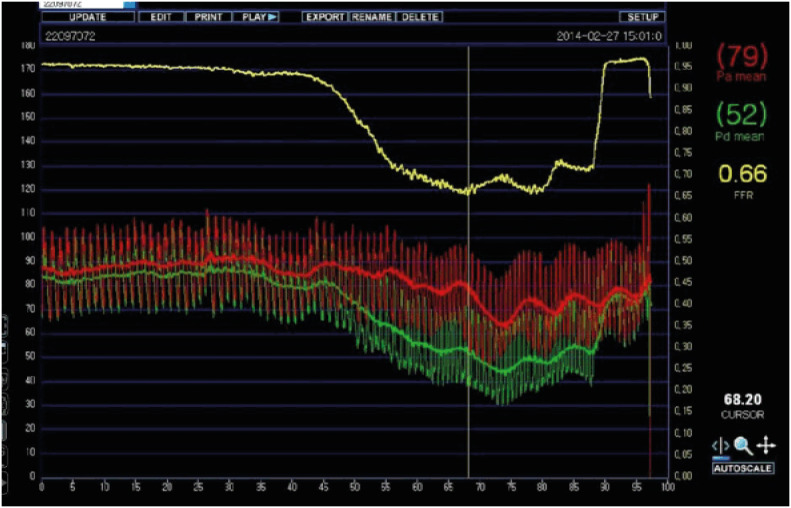 | Figure 5FFR measurement image after intracoronary adenosine administration at 20 years of age (12 years after the first PTCRA). Measured FFR was 0.66 at the time of the lowest FFR (vertical line). The yellow line, red line, and green line indicate FFR, a mean aortic pressure, and a mean coronary artery pressure distal to the target lesion stenosis in the Figure 4A (arrow), respectively.FFR = fractional flow reserve; PTCRA = percutaneous transluminal coronary rotational ablation.
|
Coronary artery lesions in KD are characterized by marked intimal thickenings and multiple calcifications caused by arteritis.1) Therefore, PTCRA may be a good alternative therapeutic option for severely calcified coronary stenosis in KD.2)3)
The Institutional Review Board of Seoul Saint Mary's Hospital approved this study and the patient's informed consent was waived (IRB number KC21ZISI0349).

 XML Download
XML Download