

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cardiovascular diseases (CVDs), principally coronary heart disease and stroke, are by far the leading cause of morbidity and mortality worldwide.1) Throughout the previous 3 decades, the prevalent cases of CVD almost doubled from 271 million in 1990 to 523 million in 2019 while related mortality increased during the same period from 12.1 to 18.6 million.2) Although age-standardized CVD mortality rates declined globally during previous decades, the number of CVD deaths is expected to increase continually due to population aging.2)
The above-mentioned temporal trends in CVD morbidity and mortality have also been observed in South Korea (hereafter Korea)3)4) and Japan.5) Since Korea is the fastest aging country in the world6) and Japan is the most aged one,7) it is not unexpected that CVDs will remain the chief contributor to morbidity and mortality in both countries. However, the process of CVD development in later years is never inevitable, because over 75% of CVDs can be prevented by ameliorating their risk factors.8) Hence, we believe that identifying modifiable risk factors for CVD and estimating their prevalences are important steps toward adopting risk prevention programs to reduce the burden of CVD in Korea and Japan.
Precedently, the American Heart Association announced in 2010 a strategic goal to reduce total CVD mortality by 20% within 10 years.9) After a careful review of the available epidemiological evidence, 7 major CVD modifiable risk factors were selected and termed as the “Life's Simple 7.”9) Later, it seemed that the goal was, to a great extent, achieved.10) Considering the difference in demographic characteristics, lifestyle, and cardiovascular risk between the East Asian and US population, building our cardiovascular health metrics based on the identified modifiable risk factors should be the key process to tackle the growing burden of CVDs in Korea and Japan.
As a primary step, this review article aims to discuss major modifiable risk factors for CVD, using epidemiological evidence from cohort studies and nationally representative data of both countries.
MODIFIABLE CARDIOVASCULAR RISK FACTORS IN KOREA AND JAPAN IN THE LITERATURE
Methods for current literature review
Articles were collected from PubMed scientific database using the search terms (“cardiovascular diseases” OR “coronary heart disease” OR “stroke”) AND (“risk factors” OR “hypertension” OR “obesity” OR “diabetes” OR “dyslipidemia” OR “Smoking” OR “physical activity” OR “diet” OR “food”) AND (“South Korea” OR “Japan”). Only cohort studies showing human evidence and published in English were considered. No limit regarding publication year was set.
Hypertension
The Korean Society of Hypertension and the Japanese Society of Hypertension define adult hypertension as systolic blood pressure ≥140 mmHg or diastolic blood pressure ≥90 mmHg.11)12) In 2018, the Korean and Japanese total population was estimated to be 51.6 and 126.8 million people, respectively13); of them, about 12 and 43 million people were estimated to have hypertension, respectively.12)14)
Hypertension is associated with the most solid evidence for CVD causation worldwide15) and also in East Asian populations.16)17) In a study conducted on 30,258 prehypertensive Korean adults, every increase in systolic blood pressure by 10 mmHg was associated with a 12% elevation in CVD mortality.18) A prospective study conducted on 10,558 individuals aged ≥30 years from the NIPPON DATA 80 showed that Japanese people with blood pressure ≥180/105 mmHg had a higher risk of CVD mortality by 37% in men and 18% in women than those with blood pressure <120/80 mmHg.19)
Of note, the control of hypertension is thought to be the most effective way to prevent the development of CVDs.15)17) In a cohort study using data of 1,402,975 adults aged 40–79 years from the National Health Information Database in Korea, the intensive control of blood pressure in hypertensive patients with several CVD risk factors led to a significant reduction in CVD events.20) Another study using the same database found that blood pressure lowering was beneficial for CVD prevention even in patients with uncomplicated, low-risk, stage-I hypertension.21) A cohort study investigating 33,372 Japanese men and women aged 40–69 years from the Japan Public Health Center-based Prospective Study (JPHC study) showed that adequate control of hypertension was estimated to prevent 64% and 50% of stroke incidence, 67% and 29% of stroke mortality, and 38% and 36% of total CVD mortality in men and women, respectively.22)
Diabetes mellitus
The diagnostic criteria for diabetes in Korea and Japan are fasting plasma glucose ≥126 mg/dL, 2-hour oral glucose tolerance test ≥200 mg/dL, hemoglobin A1c (HbA1c) ≥6.5%, or random plasma glucose ≥200 mg/dL with symptoms of diabetes (increased thirst, increased urination, and unexplained weight loss).23)24) According to the International Diabetes Federation Atlas 2019, the prevalence of diabetes among adults aged 20–79 is 9.2% in Korea and 7.9% in Japan, with the number of people with diabetes reaching 3.6 million in Korea and 7.4 million in Japan.25)
Diabetes is among the most significant risk factors for CVDs,26) even among Asian populations.16)27) In one study conducted on data of 76,434 Korean adults from the Health Screening and Promotion Center, diabetes was associated with increased risks of total CVD by 70%, coronary heart disease by 67%, and stroke by 58%.28) In the Korean Genome and Epidemiology Study (KoGES) Ansung‐Ansan cohort, diabetes almost doubled the risk of CVD mortality among 10,038 Korean adults aged 40–69 years.29) The Circulatory Risk in Communities Study investigated 3 cohorts of Japanese adults aged 40–69 years for the burden of diabetes on CVD. The results revealed that diabetes was associated with increased risk of total CVDs by 40%, 93%, and 159% in the 3 cohorts and the population attributable fraction of total CVDs due to diabetes was 2.8%, 5.6%, and 12.4%, respectively; suggesting that diabetes control can have a significant role in preventing CVDs.30) In the JPHC study, diabetes was shown to be associated with elevations in the risk of CVD events: 205% in coronary heart disease among Japanese men and women (n=31,192)31) and 64% in stroke among men (n=13,129) and 119% among women (n=22,528).32)
Dyslipidemia
According to the Korean Society of Lipid and Atherosclerosis, dyslipidemia is defined as having one or more of the following: 1) total cholesterol ≥240 mg/dL, 2) low-density lipoprotein (LDL)-cholesterol ≥160 mg/dL, 3) high-density lipoprotein (HDL)-cholesterol <40 mg/dL, or 4) triglyceride ≥200 mg/dL.33) The diagnosis of dyslipidemia, according to the Japanese Atherosclerosis Society, is slightly different with one of the following conditions that should be met: 1) LDL-cholesterol ≥140 mg/dL, 2) HDL-cholesterol <40 mg/dL, 3) triglyceride ≥150 mg/dL, or 4) non-HDL-cholesterol ≥170 mg/dL.34) More than 40% of Korean adults aged ≥30 years were shown to have dyslipidemia; 47.9% among men and 34.3% among women; significantly higher than that of Japanese adults aged ≥20 years.35) The prevalences of different biological abnormalities characterizing dyslipidemia in both countries were as follows: 1) total cholesterol ≥240 mg/dL: 19.3% of Korean men, 20.2% of Korean women, 11.0% of Japanese men, 19.9% of Japanese women, 2) LDL-cholesterol ≥160 mg/dL: 15.3% of Korean men, 19.7% of Korean women, 9.0% of Japanese men, 12.5% of Japanese women, 3) HDL-cholesterol <40 mg/dL: 27.2% of Korean men, 11.8% of Korean women, 12.0% of Japanese men, 13.2% of Japanese women, and 4) triglyceride ≥200 mg/dL: 24.8% of Korean men, 11.0% of Korean women, 11.0% of Japanese men, 19.9% of Japanese women.35)36)
Dyslipidemia is one of the major risk factors for CVDs in Asia and worldwide.16)37) In a nationwide cohort study conducted on 5,688,055 statin-naïve Koreans aged 20–39 years, comparing the highest versus the lowest quartiles of dyslipidemia elements according to their CVD events showed the following: 1) total cholesterol: increased CVD mortality by 17%, myocardial infarction by 101%, and stroke by 63%, 2) LDL-cholesterol: increased myocardial infarction by 47% and stroke by 27%, and 3) HDL-cholesterol: decreased CVD mortality by 22%, myocardial infarction by 51%, and stroke by 41%.38) In a cohort study using the NIPPON DATA 80 (n=10,546), Japanese adults aged ≥30 years with total cholesterol ≥260 mg/dL showed a 281% increase in coronary heart disease risk compared with those with total cholesterol between 160 and 180 mg/dL.39)
Smoking
Cigarette smoking is a global public health concern. In 2016, the smoking rate among people aged ≥15 years was comparable in Korea and Japan (22.8% and 20.0%, respectively). Although the smoking rate among men was higher in Korea (40.1% compared to 31.7% in Japan), that among women was higher in Japan (9.1% compared to 5.9% in Korea).40)
Smoking represents the second major modifiable risk factor for CVDs occurring globally and in Asia.16)41) In an analysis of the KoGES Ansung‐Ansan cohort comprised of middle-aged (40–69 years) Korean adults, current smoking increased CVD events by 32% and CVD mortality by 109%.29) A prospective study conducted on 19,782 men and 21,500 women aged 40–59 years from the JPHC study showed that current smokers, compared to never smokers, had significantly higher risk of coronary heart disease incidence: 185% in men and 207% in women. The same study showed that the population-attributable risk of coronary heart disease was 46% in men and 9% in women and smoking cessation led to a rapid risk reduction of coronary heart disease within 2 years.42) In a pooled analysis of 3 Japanese cohort studies (n=296,836), current smoking compared with never smoking resulted in higher risks of total CVDs by 51% in men and 85% in women, coronary heart disease by 119% in men and 184% in women, and stroke by 24% in men and 70% in women. Smoking cessation among men and women led to comparable decreases in the risks of total CVDs, coronary heart disease, and stroke after 10 years.43)
Physical inactivity
Per the World Health Organization guidelines on physical activity (≥150 minutes/week of moderate activity or ≥75 minutes/week of vigorous activity),44) approximately two-thirds of the Korean and Japanese adults did not comply with physical activity guidelines.45)46)
Substantial evidence, however, has shown that physical activity can result in significant risk reductions of CVD morbidity and mortality.16)47) A retrospective study of a total of 131,558 Korean adults from the National Health Insurance Services assessed the impact of physical activity on CVD mortality. The results showed that a 500 metabolic equivalent task-minutes/week increase in physical activity was associated with a 14% risk reduction in CVD mortality.48) A study of 74,913 Japanese adults from the JPHC study showed a 30% decline in both CVD and stroke risks from the lowest to 5–10 metabolic equivalent task-hours/day.49) In another study using data from the Japan Collaborative Cohort Study (JACC study) (n=77,676), walking ≥1 hour/day compared with 0.5 hours/day was associated with a decreased risk of total CVD by 16% while walking <0.5 hours/day compared with 0.5 hours/day was associated with an increased risk of total CVD by 35%.50)
Obesity
Obesity is a global public health problem. Worldwide, a body mass index >25 kg/m2 is considered overweight, and ≥30 kg/m2 is obese51); however, obesity for the Korean and Japanese population is defined as a body mass index ≥25 kg/m2.52)53) The prevalence of obesity in Korea and Japan has been increasing during the last decades.54)55)
Obesity is an established modifiable risk factor for CVD morbidity and mortality among Asian and non-Asian populations.16)56) In one Korean cohort study using the National Health Insurance Service data (n=209,598), obesity was associated with an increased risk of coronary heart disease among adults aged ≥20 years by 31%, and the population-attributable risk was 8.1%.57) In another study using the same data (n=2,611,450), weight gain from <23.0 to ≥25 kg/m2 was associated with increased risk of myocardial infarction by 67% in men and 50% in women and coronary heart disease by 35% in men and 31% in women.58) Further, in Japanese data of 42,343 men and 46,413 women aged 40–69 years from the JPHC, obesity resulted in an increased risk of cardioembolic strokes in men and women and lacunar and large-artery occlusive strokes in women only. Cumulative average body mass index was positively associated with lacunar, large-artery occlusive, and cardioembolic strokes in men and with lacunar and large-artery occlusive strokes in women.59)
However, weight reduction to the normal range can lower the risk of CVD. In a Korean study of young adults,58) weight reduction from ≥25 kg/m2 to <23.0 kg/m2 was associated with decreased risk of myocardial infarction by 33% in men and coronary heart disease by 23% in men and 33% in women. It should be noted that being underweight and excessive weight loss were shown in East Asian and Japanese literature to be associated with an increased risk of CVD mortality60)61)62); suggesting the importance of health expert consultation before planning to lose weight.
Diet
Solid evidence relating poor-quality diet to the risk of CVD has been emerging. Despite being debated, poor-quality diets have, in general, high salt, added sugars, and animal-source fats but low fish, fruits and vegetables, and whole grains.63) Herein, we will focus on 2 staple foods, fish and salt, that characterize the East Asian diet64) and were previously suggested as risk factors for CVDs.65)66) On the other hand, consuming red meat,67)68) rice,69)70) and alcohol71)72) showed no or faint associations with the risk of CVDs among Korean and Japanese populations, and thus were not discussed in depth.
Fish is a recommended source of omega-3 fatty acids that confer benefits for reducing CVD risk.65) In a study conducted on 41,578 Japanese people aged 40–59 years from the JPHC study, the intake of 180 g/day vs. 23 g/day of fish was associated with a 37% decrease in coronary heart disease risk, and the intake of omega-3 fatty acids was inversely associated with the risk of myocardial infarction.73) Another study using data from the JACC study (n=57,972) showed inverse associations between fish and omega-3 fatty acids intake and the risk of CVD mortality.74) A case-control study carried out in Korea (n=120) also revealed that every 1% increase in the omega-3 index was associated with 60.3% and 26.6% lower odds of hemorrhagic stroke and ischemic stroke, respectively.75)
Dietary sodium intake is a potential risk factor for CVD.66) In a case-control study of 304 cases with stroke and 249 age-matched controls conducted in Korea, high sodium intake was associated with 40% and 50% higher odds of stroke in men and women, respectively.76) Another case-control study from Korea (n=146) revealed that a substantially higher proportion of stroke cases (60.3%) preferred salty foods than their counterparts (20.5%).77) In the Japanese cohort Study (JPHC; n=77,500), the highest compared with the lowest quintile of sodium and salted food intake was associated with a 19% increase in the total CVD risk.78) In the NIPPON DATA 80 (n=8,879), adherence to a reduced-salt Japanese diet led to a decrease in the risk of CVD mortality by 20%.79) Another study using the same data (n=8,702) showed that an increment of 2 g/1,000 kcal in household salt intake was associated with the increased risk of total CVD, coronary heart disease, and stroke mortality by 11%, 25%, and 12%, respectively.80) Alike, the JACC study (n=58,730) showed that the highest versus the lowest quintile of sodium intake was associated with increased risk of total CVD and stroke mortality by 42% and 55%, respectively.81) In another study using the JACC study data (n=84,720), salt preference was associated with a 23% increase in stroke mortality.82)
NATIONAL PREVALENCE OF MODIFIABLE CARDIOVASCULAR RISK FACTORS IN KOREA AND JAPAN
Data sources
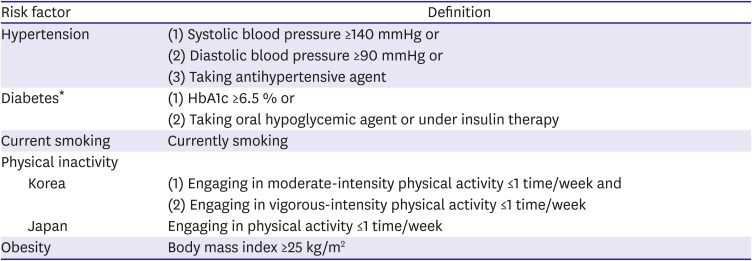
We compared the prevalence of major modifiable CVD risk factors in Korea and Japan using the Korea National Health and Nutrition Examination Survey (KNHANES; 2016–2018)83) and Japan National Health and Nutrition Survey (JNHNS; 2017–2019).84) Detailed definitions of the assessed risk factors are described in Table 1. All analyses of the KNHANES data accounted for its complex multi-stage sampling design and were weighted to generate nationally representative estimates of the Korean population. Sex- and age-specific prevalence of risk factors in each country were calculated and compared. To adjust for the difference in population structures between Korea and Japan, age-standardization was performed by direct method with the population structure of Korea in 2017 as a reference, separately by sex. The prevalence of dyslipidemia was not calculated because fasting lipid levels had not been measured in the JNHNS.
Table 1
Definition of cardiovascular risk factors for Korean and Japanese data analyses
The estimated prevalence of risk factors
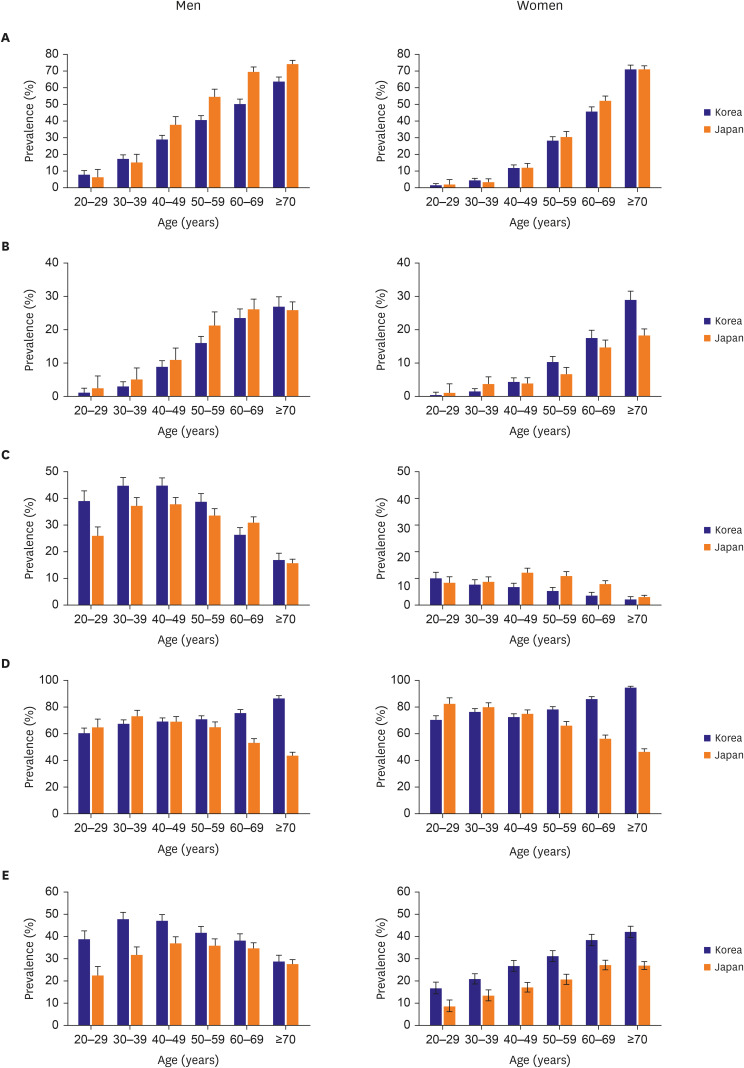
Figure 1 depicts sex- and age-specific prevalence of risk factors in Korea and Japan. In both countries, the prevalence of hypertension was proportionately higher with age regardless of sex, reaching 63.7% and 74.2% at age ≥70 among Korean and Japanese men, respectively; 71.0% at age ≥70 among both Korean and Japanese women. Among men, the prevalence of hypertension was marginally higher in Korea under age 39, whereafter the prevalence was higher in Japan. Among women, the prevalence of hypertension was generally comparable across all ages, except for the 60s at which the prevalence was higher in Japan (45.7% and 52.1% in Korea and Japan, respectively) (Figure 1A). In both countries, the prevalence of diabetes was higher with older age regardless of sex. Among men, the prevalence of diabetes was higher in Japan across all ages, except for the age ≥70 group. Among women, the prevalence of diabetes was higher in Japan under age 39, whereafter the prevalence was higher in Korea (Figure 1B). In both countries, men smoked more in their 30s and 40s (44.7% and 44.8% in Korea and 37.2% and 37.8% in japan, respectively); however, the proportion of smoking fell sharply after that, reaching <20% at age ≥70 years. Japanese women smoked more in their 40s and 50s (12.1% and 10.9%, respectively), whereas Korean women smoked more in their 20s and 30s (10.0% and 7.7%, respectively) (Figure 1C). In Korea, the proportions of physically inactive men and women were generally higher with older age, whereas those in Japan were lower with age after the 30s (Figure 1D). However, since the definitions of physical inactivity in KNHANES and JNHNS are different, a direct comparison between Korea and Japan with regard to the proportion of physical inactivity should be made with caution. Obesity was more prevalent in Korea across all ages regardless of sex. Men were found to be more obese in their middle years (47.1% and 36.9% at age 40–49 in Korea and Japan, respectively), whereas women tended to be more obese with increasing age (42.1% and 26.9% at age ≥70 in Korea and Japan, respectively) (Figure 1E).
Figure 1
Prevalence of cardiovascular risk factors in Korea and Japan. (A) Hypertension, (B) diabetes, (C) current smoking, (D) physical inactivity, (E) obesity. Error bars indicate 95% confidence intervals.
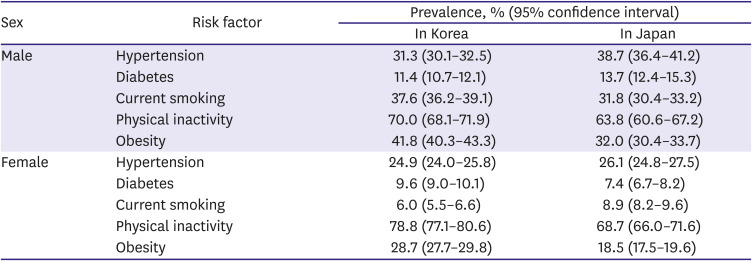
The age-standardized prevalence of risk factors in Korea and Japan are presented in Table 2. Japanese men had a higher prevalence of hypertension and diabetes than Korean men. However, the proportion of current smokers and obese adults were higher among Korean men than among Japanese men. Contrariwise, Japanese women were more likely to have hypertension or be current smoker than Korean women, while the greater prevalence of diabetes and obesity were observed among Korean women.
Table 2
Age-standardized prevalence of risk factors in Korea and Japan
CONCLUSION
This review article introduced solid epidemiological evidence of the associations between major modifiable cardiovascular risk factors, including hypertension, diabetes, dyslipidemia, cigarette smoking, physical inactivity, obesity, and poor-quality diet, and CVD in the Korean and Japanese population. We also estimated the prevalence of risk factors in Korea and Japan, and compared them to provide an overview of the burden of CVD risk factors in both countries. Since a substantial proportion of CVD events are preventable, the implementation of primordial prevention strategies focused on the above-mentioned risk factors should be the priority of the health policymakers and public health leaders to curb the increasing burden of CVD in Korea and Japan.
 XML Download
XML Download