

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The heart and kidneys maintain hemodynamic stability together by controlling cardiac output, volume status, and vascular tone.1) The relationship between these two organs is responsible for the bidirectional abnormalities of heart and kidney function, in which one organ may induce or perpetuate disease in the other.2) In the setting of acute heart failure (AHF), approximately 30% of patients were found to have a reduced glomerular filtration rate (GFR) at baseline, independent of their level of left ventricular function.3) Reduced renal function predicts considerably higher rates of mortality and hospitalization because of acute cardiac dysfunction. Furthermore, heart failure (HF) is frequently associated with patients who have chronic kidney disease, and this is associated with increased morbidity and mortality. The interaction between the kidneys and heart has been characterized as a clinical entity called cardiorenal syndrome (CRS).4)5)6)
At a consensus conference of the Acute Dialysis Quality Initiative, CRS was classified into five subtypes based on the time course and type of abnormality that first develops in the kidneys and heart (Table 1). Type 1 CRS is an abrupt deterioration of heart function inducing acute kidney injury (AKI), previously described as worsening renal function. In the literature, the criterion used most commonly for worsening renal function is an increase of serum creatinine of at least 0.3 mg/dL or at least 25% over the first 5 days of hospitalization, which differs from the current Kidney Disease Improving Global Outcomes definition for AKI.7)8) Type 2 CRS is frequently observed in the clinical setting as progressive renal dysfunction associated with chronic HF. Type 3 CRS is characterized by worsening kidney function, which induces acute cardiac dysfunction. Retention of uremic solutes and/or volume overload may contribute to heart injury in type 3 CRS.9) Type 4 CRS is found in approximately 70–80% of patients with end-stage renal disease who frequently experience cardiac dysfunction complications. CRS type 5 includes acute or chronic systemic conditions that cause simultaneous dysfunction of the heart and kidneys.

Table 1
Classification of cardiorenal syndrome
![]()
This review aimed to primarily focus on renal dysfunction and/or injury in the setting of decompensated HF. We will examine the pathophysiology related to hemodynamic interplay, including venous congestion, and hypoperfusion, diagnostic methods for detecting these hemodynamic changes, and therapeutic interventions such as diuretics or ultrafiltration for venous congestion.
Go to : 
PATHOPHYSIOLOGY OF CARDIORENAL SYNDROME
Possible mechanisms of CRS have traditionally been suggested as a consequence of insufficient renal perfusion, which decreases proportionately with declining cardiac output.10) Decreased renal perfusion results in the activation of the sympathetic nervous and renin-angiotensin-aldosterone systems, and secretion of arginine vasopressin, leading to a deterioration of cardiac function through systemic congestion. Clinical evidence for this mechanism is that a left ventricular assist device or cardiac resynchronization therapy has been shown to preserve or improve renal function in selected patients with end-stage heart disease until the implementation of more definitive therapy, such as heart transplantation.11)
However, mechanistic studies have been largely unable to find a correlation between deterioration in renal function, cardiac output, left-sided filling pressures, and reduced renal perfusion.12) In the Acute Decompensated Heart Failure National Registry, the incidence of AKI was similar between HF with reduced and preserved ejection fraction, indicating that the impairment of forward flow is not likely the primary culprit of renal dysfunction in many patients with CRS.13)14) Additionally, the decline of renal function during treatment for HF occurs more often in patients with preserved ejection fraction rather than in those with severely reduced ejection fraction. Although the impairment of forward flow (cardiac output) in the setting of decompensated HF can contribute to acute deterioration in kidney function, there has been increasing evidence that decreased kidney function in patients with HF may not be adequately explained by renal hypoperfusion alone.
Recent studies have recognized that increased renal backpressure caused by venous congestion is the major pathophysiological mechanism of renal dysfunction in CRS.2)7)8) Systemic venous congestion is conveyed back, generating increased renal venous pressure and reducing the arteriovenous gradient over renal circulation and thereby impairing renal blood flow. Moreover, independent from renal blood flow, increased renal venous pressure leads to renal parenchymal congestion within the stiff renal capsule, resulting in increased interstitial pressure that may compress the entire capillary and renal tubules, thereby reducing GFR.12) Experimental animal studies have demonstrated the effects of increased renal venous pressures on reduction in urine flow and alteration in glomerular and tubular function.15) A stepwise increase in renal venous pressure resulted in a decrease of the GFR with increased tubular pressure. Conversely, reduction in venous pressure reversed impaired diuresis.16) Furthermore, renal blood flow is decreased by increased venous pressure even more than an equivalent decrease in arterial pressure; thus, urine flow is decreased equal to the decrease in arterial pressure.
Clinically, renal venous congestion secondary to increased systemic pressure is often reflected by high right atrial pressures (RAPs) and central venous pressures. Subgroup analysis of the Evaluation Study of Congestive Heart Failure and Pulmonary Artery Catheterization Effectiveness (ESCAPE) trial demonstrated improved heart function that was not associated with improved renal outcomes, but increased RAPs and central venous pressures were associated with decreased kidney function.17) Damman et al.18) also showed that increased venous pressure was an independent factor for glomerular filtration in patients with cardiac dysfunction,12) and the highest RAPs were observed in patients with the lowest GFR. Moreover, high central venous pressure was associated with HF rehospitalization and increased mortality.19) Finally, in patients who had congestion confirmed by echocardiography, reduction of congestion by treatment was associated with an improvement of renal function in HF with right ventricular dysfunction.16) Therefore, increased central venous pressure and renal venous congestion are now widely accepted as primary determinants of renal impairment in chronic and acute decompensated HF.
Although venous congestion is primarily driven by volume or fluid overload in CRS, many patients do not experience a change in weight before hospitalization for acute decompensated HF.20) In a post-hoc analysis of patients with acute decompensated HF in the Acute Study of Clinical Effectiveness of Nesiritide and Decompensated Heart Failure trial, 26% of patients showed no weight loss during hospitalization.21)22) Another study found that 34% of patients admitted for HF were either normovolemic or hypovolemic with often a normal plasma volume.23) A potential contributing mechanism could be blood volume redistribution from the veins of the abdomen, i.e., splanchnic veins, to the circulating blood volume.24)
The splanchnic veins contain between 20% and 50% of the total blood volume and regulate cardiac filling volume during changes in volume status, which is controlled by the sympathetic nervous system.23)24)25) As a result of sympathetic nerve overactivity in HF, vasoconstriction in this compartment forces movement of venous blood to the circulating compartment, which contributes to venous congestion and HF decompensation.26) Venous congestion resulting from volume redistribution in the absence of weight gain or total body volume was associated with impairment of renal function in patients with HF.
Additionally, elevated intraabdominal pressure elicited by systemic and abdominal congestion is increasingly recognized as a potential mechanism contributing to CRS.27)28) In patients with acute decompensated HF, increased intraabdominal pressure was also prevalent and correlated with the serum creatinine level in patients who had HF with reduced left ventricular ejection fraction.29) Another study reported that a persistent increase in intraabdominal pressure at 72 hours was associated with 1-year mortality and a longer length of hospital stay in patients who had acute HF with reduced ejection fraction and preserved ejection fraction. Furthermore, a strong correlation was observed between a reduction in the intraabdominal pressure at baseline and improvement in renal function, independent of hemodynamic changes.30)
Several studies have suggested that renal dysfunction associated with elevated intraabdominal pressure is not due to the direct parenchymal pressure on the kidneys, but impairment with the return of renal venous blood flow and consequent high renal venous pressure and renal venous congestion.23)24)29) In healthy volunteers, increased intraabdominal pressure through external abdominal compression results in increased renal venous pressure and central venous pressure and decreased renal blood flow, GFR, tubular function, and urine output. In another study, the increased intraabdominal pressure was transmitted directly to the level of the renal venous system, and when intraabdominal pressure reached values of about 20 mmHg, it quickly caused a reduction of renal blood flow and filtration by 24.4% and 27.5%, respectively.31) Conversely, reduction in increased intraabdominal pressure by ultrafiltration or paracentesis was associated with an improvement in renal function in some patients.31)
Go to :
DIAGNOSTIC STRATEGIES FOR CONGESTION IN CARDIORENAL SYNDROME
Serum and urine biomarkers
Serum creatinine is widely used as a biomarker of kidney function and to define AKI in CRS. However, GFR may decrease by more than 50% from normal before a significant increase in the serum creatinine level occurs, making creatinine insensitive to small but significant reductions in the GFR. As the early identification of worsening kidney function is the key element of CRS treatment, biomarkers that are highly sensitive to kidney injury may facilitate better outcomes of organ injury, including in the heart and kidneys. Biomarkers such as neutrophil gelatinase-associated lipocalin (NGAL) and kidney injury molecule-1 have been implicated in tubulointerstitial damage and have been used to identify AKI.16)32) The serum NGAL level is a marker of reduced glomerular filtration, which becomes elevated earlier than creatinine, and the presence of NGAL in the urine indicates proximal tubular injury.33) An elevated NGAL level was observed in HF with renal dysfunction,34) and increased serum and urine levels of NGAL could be useful predictors for dialysis and death in AKI, including CRS.35)
Besides kidney biomarkers, cardiac biomarkers including the B-type natriuretic peptide (BNP) and troponin also have value in the diagnosis and prognosis of HF and CRS. Elevation of BNP and cardiac troponin levels are associated directly with congestion in CRS. However, HF patients with impaired renal function have higher BNP levels than patients with normal renal function, which could be attributed to impaired renal function. ST2, an interleukin-1 receptor family member, is another useful biomarker. It is a new biomarker of congestion that is less affected by kidney function than N-terminal pro-BNP, and it may add to the diagnostic and prognostic information provided by N-terminal pro-BNP.7) However, it is not at present readily available for clinical use.
Renal Doppler ultrasonography
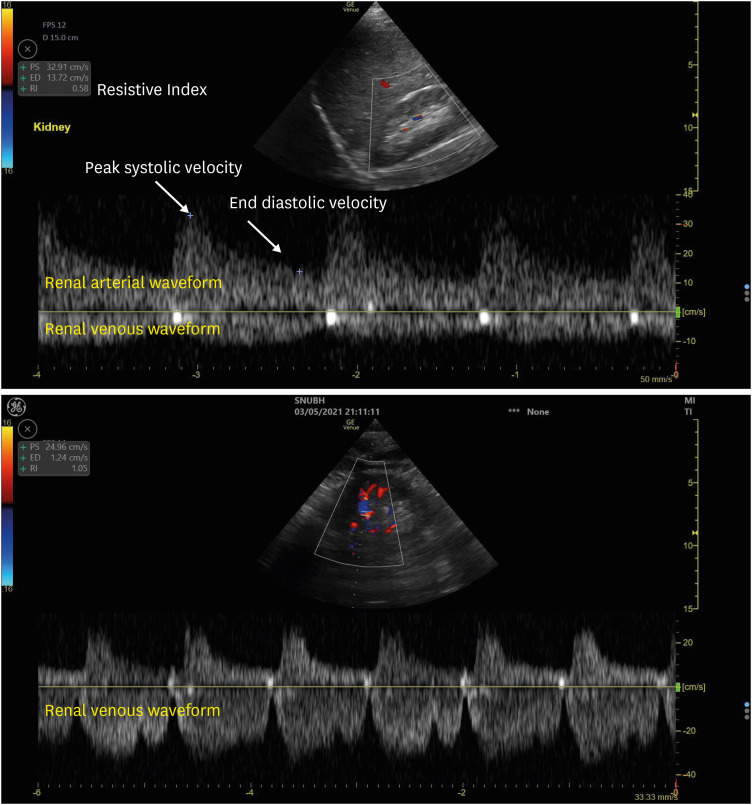
The role of increased central venous pressure and subsequent renal venous congestion is now widely accepted as one of the principal mechanisms in renal dysfunction in chronic and acute decompensated HF.36) However, renal venous congestion remains difficult to identify. Recently, the renal vein flow pattern has been studied using Doppler ultrasonography to evaluate renal congestion in patients with HF or those undergoing cardiac surgery. A normal intrarenal venous waveform is relatively continuous with gentle undulation, however, as the RAP increases, it becomes more of a pulsatile pattern with systolic flow reversal due to the backward pressure from the RAP transmitted to renal veins, particularly in patients with a congested inferior vena cava, as in HF (Figure 1).
In HF, intrarenal venous flow patterns depend on the RAP; normal continuous flow patterns were correlated with a normal RAP (RAP <8 mmHg), and discontinuous flow was associated with an increased RAP. A discontinuous renal flow pattern has been associated with renal congestion and poor diuretic response in patients with HF.37) In particular, a monophasic pattern had the highest RAP, suggesting severe renal congestion. Moreover, a significant improvement of venous flow patterns following decongestive treatment was observed in patients with acute HF.38) Another study also showed that a congestive pattern based on the venous pattern was associated with a worse prognosis in acute and chronic HF.39)
Besides the renal venous flow profile, the renal arterial waveform also has an incremental prognostic value that could reflect the mechanisms underlying the progression of renal disease in HF. The renal arterial resistive index (RI) is calculated from the intrarenal arterial waveform at the level of the segmental arteries using the Pourcelot formula, i.e., peak systolic velocity minus enddiastolic velocity, divided by peak systolic velocity.40) In healthy adults, normal renal RI values are approximately 0.60, whereas an RI of 0.70 or higher is considered abnormal and generally predictive of a poor outcome.41)
Compared to the GFR, the renal RI has an incremental role in the evaluation of renal function and the prognosis of patients with HF. In the setting of HF, the RI was independently associated with renal dysfunction at 1 year irrespective of the GFR values, and it was associated with poor prognosis in HF patients with preserved ejection fraction.42) The role of the RI in predicting worse outcomes was also studied in the setting of HF with reduced ejection fraction, and the RI was independently associated with composite endpoints including progression, hospitalization, and death due to acute decompensated HF.43) A higher RI value was also associated with the use of high doses of loop diuretics; additionally, higher values of the RI could predict poor diuretic response and identify patients prone to diuretic resistance, possibly because increased renal resistances lead to reduced delivery of diuretic drugs to the site of action. However, the Doppler technique for assessing the renal venous and arterial waveforms requires expertise, and validation is necessary to ensure consistency of Doppler waveform sampling by operators. Furthermore, it may not always be possible to obtain adequate tracings, particularly in critically ill patients.44)
Go to :
OPTIONS FOR DECONGESTIVE TREATMENT IN CARDIORENAL SYNDROME
Diuretics
Since venous congestion is the major pathophysiological mechanism of CRS, diuretics are expected to have beneficial effects. Although decongestion with diuretics is the mainstay of the initial treatment of HF, the impact of diuretics as decongestive therapy on outcomes is not constant. Post-hoc analysis of the Determining Optimal Dose and Duration of Diuretic Treatment in People With Acute Heart Failure (DOSE-AHF) study45) to evaluate diuretic dosing in AHF showed improved renal function during decongestion therapy, which was associated with a worse outcome. However, in the ESCAPE study17) and the Efficacy of Vasopressin Antagonism in Heart Failure Outcome Study with Tolvaptan study,46) diuretic therapy was correlated with renal function deterioration, but the death rate was lower in the group that received aggressive diuretic therapy than in the group that did not.
Worsening renal function, defined by the elevation of the serum creatinine level during decongestion therapy, has less prognostic impact than other biomarkers reflecting the GFR or tubular injury.47) An increased serum creatinine level may result from mechanisms independent of a decreased GFR such as hemoconcentration. This mostly transient renal dysfunction in the context of clinical improvement has also been called “pseudo-worsening renal function”.7) A recent study showed that during aggressive decongestion, the serum creatinine level increased in 22% of patients with decompensated HF without an increase in biomarkers of tubular injury.48) Unless renal perfusion is decreased during decongestion therapy, diuretic therapy should be maintained regardless of an increase in the serum creatinine level.
Loop diuretics, furosemide, torsemide, and bumetanide, are the most common diuretics used in HF.49) Loop diuretics cause natriuresis by blocking the Na+, K+, and Cl2- symport on the thick ascending limb of the loop of Henle, thereby causing reduced volume overload and renal venous congestion. However, their effectiveness is limited in certain patients with CRS for several reasons. Most loop diuretics bind to plasma proteins to reach their site of action; thus, hypoalbuminemia, which is common in decompensated HF, could reduce the delivery of diuretics to the site of action.5)6) Moreover, diuretics compete with exogenous or endogenous anions, such as nonsteroidal anti-inflammatory drugs, and uremic toxin for plasma protein binding, resulting in reduced diuretic efficacy. Lastly, renal dysfunction in the setting of CRS reduces the excretion of the diuretic into the tubular lumen and decreases sodium filtration through the glomerulus, which could attenuate natriuresis by diuretics. Therefore, a higher dose of diuretics is needed to achieve the same therapeutic effect in HF.
When high doses of diuretic agents are required or when the effect is suboptimal, increased frequency or continuous use of a loop diuretic could be considered. However, compared with a bolus infusion, continuous infusion of loop diuretics showed no difference in symptom relief or change in renal function according to the DOSE-AHF trial, and was associated with more hyponatremia, the need for vasopressors, and rehospitalization.50) The addition of a non-loop diuretic in combination with a loop diuretic is often required among patients with severe HF who are receiving long-term and/or high-dose therapy with loop diuretics and may overcome diuretic resistance. The combination of thiazide and loop diuretics presented increased distal sodium reabsorption due to the loop diuretics, thereby augmenting natriuresis.5)6) Additionally, mineralocorticoid receptor antagonists could diminish renin-angiotensin activation, which increases sodium reabsorption at proximal tubules with favorable outcomes in patients with HF.
Ultrafiltration
Ultrafiltration is an invasive fluid removal technique used in patients with decompensated HF and diuretic resistance.51) The proposed benefits of ultrafiltration are the controlled rates of fluid and sodium removal and minimal serum electrolyte depletion compared to diuretics. Thus, ultrafiltration in CRS may have an early role by rapidly reducing venous pressure, which may supplement the need for diuretic therapy.5)
In two trials of ultrafiltration in patients with acute decompensated HF, the Relief for Acutely Fluid-Overloaded Patients with Decompensated Congestive Heart Failure study52) and the Ultrafiltration versus Intravenous Diuretics for Patients Hospitalized for Acute Decompensated (UNLOAD) study,53) there was greater fluid removal without hemodynamic instability and relief of HF symptoms but no improvement in kidney function. These findings support the potential advantage of ultrafiltration because the removal of isotonic fluids by ultrafiltration may be better than the removal of hypotonic fluids with diuretics.
Following the two aforementioned studies, 188 patients with type I CRS were randomized to stepped pharmacologic care or ultrafiltration in the Cardiorenal Rescue Study in Acute Decompensated Heart Failure (CARESS-HF) study.54) The primary endpoint was a change in the serum creatinine level and change in weight at 96 hours. Although similar weight loss (reflecting fluid removal) occurred with the two strategies, ultrafiltration resulted in increased serum creatinine levels and side effects mainly due to bleeding and intravenous catheter-related complications. Unexpectedly, in the CARESS-HF trial, ultrafiltration was inferior to pharmacological therapy in maintaining renal function and was associated with a higher rate of adverse events. However, several criticisms have been raised in response to this trial because the serum creatinine level does not represent renal parenchymal damage and transient GFR reductions and a more aggressive decongestive approach may be needed to achieve better long-term renal outcomes. Additionally, in the design of the CARESS-HF study, the rate of ultrafiltration was fixed at 200 mL/h without any adjustment, contrary to efficiently stepped pharmacologic therapy.
In the subsequent Continuous Ultrafiltration for Congestive Heart Failure trial, Marenzi et al.55) compared the efficacy between diuretics and ultrafiltration over the longest follow-up period ever reported. Consistent with the results of the UNLOAD trial,53) in the ultrafiltration group there was a significantly lower incidence of HF rehospitalization together with the stability of renal function. In the most recent AVOID-HF trial, the time before the first HF event and rehospitalization rates were compared between the diuretics and ultrafiltration groups in 810 patients with HF.56) Compared to the diuretics group, in the ultrafiltration group there was a longer time before the first HF event but more serious adverse events due to ultrafiltration. Unfortunately, this trial had serious problems with premature termination and recruitment issues, so the results of this study cannot be considered conclusive.
Although ultrafiltration may be helpful for fluid removal in CRS, particularly in patients unresponsive to diuretic therapy, the available evidence does not establish ultrafiltration as primary therapy for effective decongestion in CRS. The relative failure of ultrafiltration compared to diuretic therapy might have resulted from the fixed rates of fluid removal rather than adaptive control of ultrafiltration guided with volume assessment. Careful clinical assessment of the degree of volume overload or venous congestion is paramount when ultrafiltration therapy is administered. The ongoing Volume Management under Body Composition Monitoring in Critically Ill Patients on Continuous Renal Replacement Therapy trial will help shed light on the effect of modifying the ultrafiltration rate according to the volume status of individual patients assessed with bioimpedance analysis.57)
Go to :
CONCLUSION
Although various clinical studies have confirmed that decongestive therapy has a definite role in decreasing volume overload and providing consequent symptom improvement in patients with CRS, the impact of diuretics or ultrafiltration on the improvement of kidney function or mortality remains uncertain. A precise assessment of volume status is required to determine the adequacy of decongestion. Objective measures of renal venous congestion may be a future metric that can be followed to assess the adequacy of patients' diuretic response and to guide therapeutic decision making. The role of renal Doppler ultrasonography in assessing renal venous congestion should be made in further prospective investigations to optimize decongestive therapy.
Go to :
 XML Download
XML Download