

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The coronavirus disease 2019 (COVID-19) pandemic is ongoing. As of June 12, 2021, there have been 174,918,667 confirmed cases of COVID-19, including 3,782,490 deaths globally.1 The long-term success of the public health response to COVID-19 would depend on herd immunity.2 To establish herd immunity, the immunity generated by natural infection or vaccination must prevent onward transmission, not just clinical disease. The estimated herd immunity threshold was noted approximately 67% for COVID-19.2 However, several studies have shown that achieving herd immunity through natural infection might be difficult.345 Vaccination is necessary to reach herd immunity threshold for COVID-19.
As of June, 11, 2021, six vaccines were listed on the WHO's Emergency Use List and approved for use: BNT162b2, mRNA-1273, AZD1222, Ad26.COV2.S, BIBP/Sinopharm, and CoronaVac.67 Among these vaccines, BNT162b2 was approved for individuals aged 16 years and older.7 On May, 10, 2021, the US FDA expanded the emergency use authorization for BNT162b2 vaccine to include adolescents 12 to 15 years of age.8 On May 28, 2021, BNT162b2 vaccine was approved for use in children aged 12 to 15 in the EU.9 Since mass vaccination was launched in South Korea on February 26, 2021, 23.0% of the nation's population have received at least one dose of COVID-19 vaccine as of June, 12, 2021.10 In South Korea, COVID-19 vaccination for children (under the age of 18 years) has not yet been approved. It is likely to expand to this age group.11
The aim of this study was to investigate parental acceptability of COVID-19 vaccination for their children and factors affecting their acceptability. In addition, we evaluated perceptions of children (aged 10 to 18 years) regarding childhood COVID-19 vaccination.
METHODS
Study design and data collection
We conducted a questionnaire survey to investigate adolescents and parents' perceptions of COVID-19 vaccination for children and adolescents. The survey recruitment took place at the Pediatrics Outpatient Clinics of Pusan National University Hospital (Busan, Republic of Korea) and Pusan National University Children's Hospital (Yangsan, Republic of Korea) from May 25, 2021 to June 3, 2021. Subjects were parents having children under the age of 18 years and children or adolescents aged 10–18 years, who agreed to participate in the survey.
The questionnaire for parents had six sections (Supplementary Data 1): sociodemographic characteristics, family members and medical history, COVID-19 related history, attitudes toward COVID-19, attitudes toward COVID-19 vaccines, and acceptance of COVID-19 vaccination for their children. For children or adolescents, the questionnaire had four sections (Supplementary Data 2): age and gender, COVID-19 related history, attitudes toward COVID-19, and acceptance of COVID-19 vaccines. Responses to “attitudes” or “acceptance” were rated as follows: extremely likely, somewhat likely, neither likely nor unlikely, somewhat unlikely, and extremely likely.
The main outcome of the study was parents' willingness to vaccinate their children with COVID-19 vaccine. Predictor variables such as concerns about COVID-19, retrieval of COVID-19 vaccine information, trust in COVID-19 vaccine information, and confidence of effectiveness or safety of COVID-19 vaccines were analyzed.
Statistical analysis
Categorical variables were presented as counts and percentage. They were compared using Fisher's exact test. For parents' willingness to vaccinate their children, univariate analysis was performed to compare acceptance (responses of “extremely likely” or “somewhat likely”) and non-acceptance (responses of “neither likely nor unlikely,” “somewhat unlikely,” or “extremely unlikely”) groups of parents. A multiple logistic regression was performed to determine factors affecting parental intention to vaccinate their children using variables with P < 0.1 in the univariate analysis. Statistical significance was considered when a two-sided P value was less than 0.05. All statistical analyses were performed using Prism 9 (GraphPad Software Inc., San Diego, CA, USA).
Ethics statement
The study protocol was reviewed and approved by the Institutional Review Board of Pusan National University Hospital (approval No. 2105-017-103) and Pusan National University Children's Hospital (approval No.05-2021-098). Informed consent was obtained from all subjects when they were enrolled.
RESULTS
Two hundred twenty-six parents and 117 children aged 10–18 years were included in the final analysis. Baseline characteristics of these participants are presented in Table 1. Most (79.6%) of parent participants were mothers. The age group having the most participants was 40–49 years. Among children of parent participants, 47.1% were 7–12 years old. About half (48.7%, 167/343) of total participants had been tested for COVID-19 by themselves or someone in their family. Among parent participants, 118 (52.2%) had household members having underlying diseases or belonging to risk groups and 77 (34.1%) had children who had underlying diseases (Table 2).
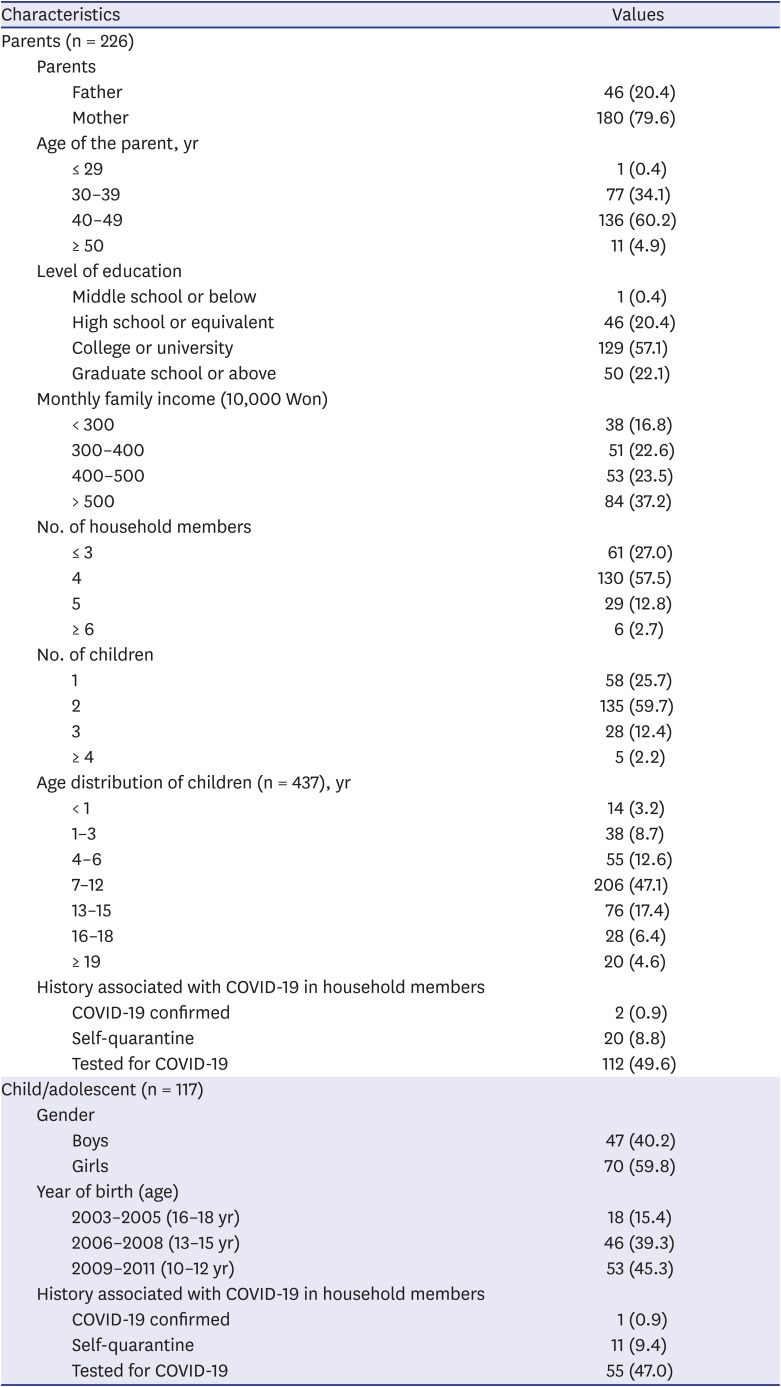
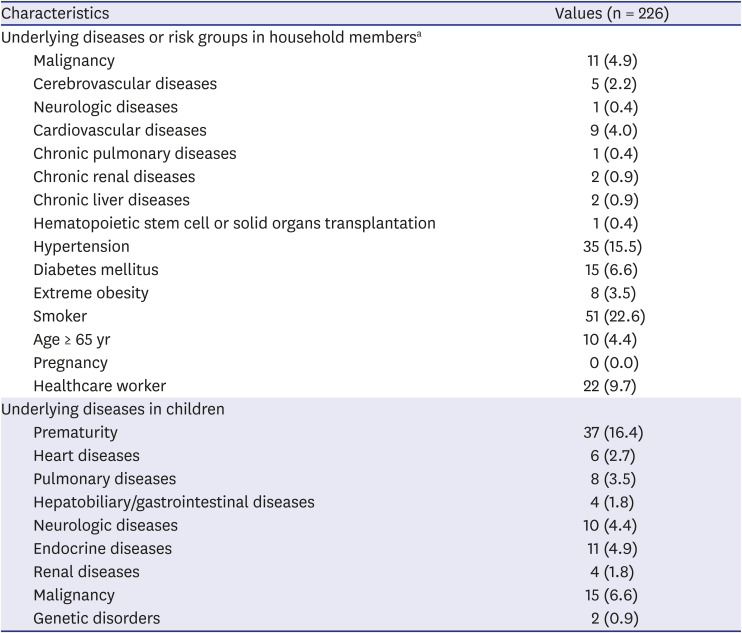
Table 1
Baseline characteristics of participants
![]()
Table 2
Underlying diseases or risk groups in family
![]()
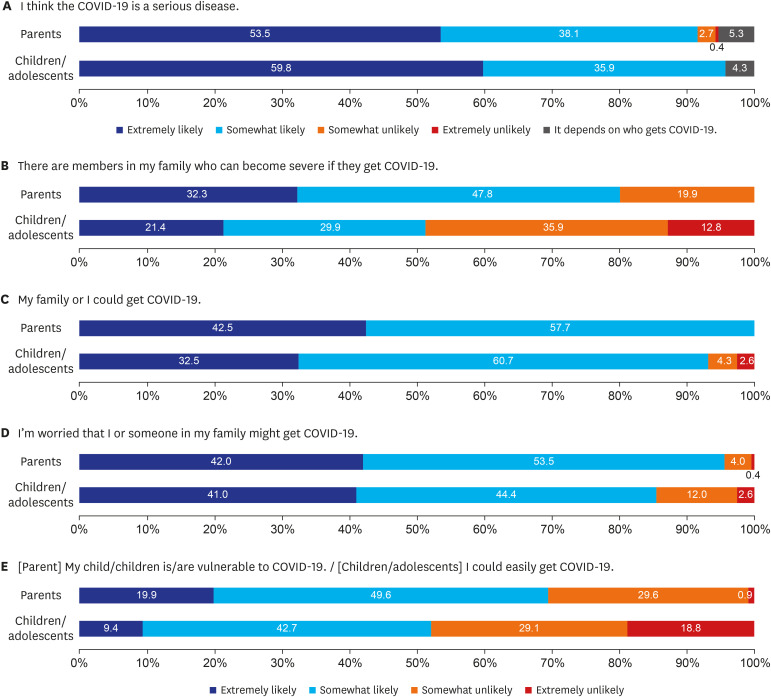
Participants' attitudes toward COVID-19 are shown in Fig. 1. More than 90% of participants expressed “serious disease” or “anxiety about SARS-CoV-2 infection.” Anxiety of vulnerability to COVID-19 in children was higher in parent participants than in child/adolescent participants (69.5% vs. 52.1%, P = 0.002).
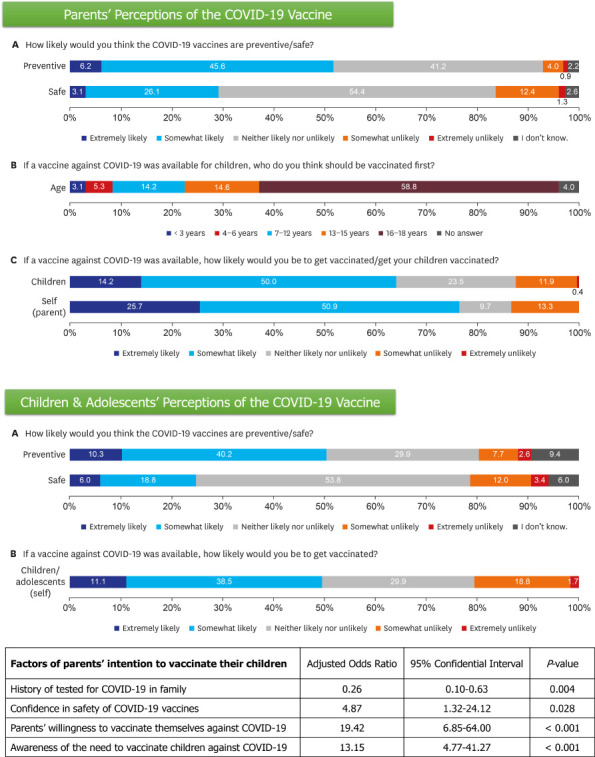
Awareness of COVID-19 vaccines in participants is summarized in Table 3. The proportion of respondents who actively searched for COVID-19 vaccine information was significantly higher in parent participants than in child/adolescent participants (54.9% vs. 17.9%, P < 0.001). Regarding the effectiveness and safety of COVID-19 vaccines, 51.3% (176/343) responded with “preventive,” while only 27.7% (95/343) responded with “safe.” Among parent participants, 179 (79.2%) responded that children and adolescents needed COVID-19 vaccination. If COVID-19 vaccination is available for children under 18 years old, 58.8% of parent participants selected ‘16–18 years' as the prior age group for vaccination (Fig. 2). Overall, 76.5% of parents intended to get vaccinated against COVID-19 and 64.2% intended to let their children get vaccinated. The agreement rate of intention to vaccinate themselves and their children was the highest in “neither likely nor unlikely” (Fig. 3). One hundred thirty-seven parent participants were divided into three groups of < 7 years (45/137), 7–12 years (63/137), and 13–18 years (29/137) according to their children's age subgroups. Among these, there was no significant difference in parents' willingness to vaccinate their children by children's age subgroups (55.5% in < 7 years; 63.5% in 7–12 years; 62.1% in 13–18 years; P = 0.695). In child/adolescent participants, 49.6% responded they would get COVID-19 vaccination (Fig. 4). There was no significant difference in acceptance rate by age subgroups (50.9% in 10–12 years; 50.0% in 13–15 years; 44.4% in 16–18 years; P = 0.890).
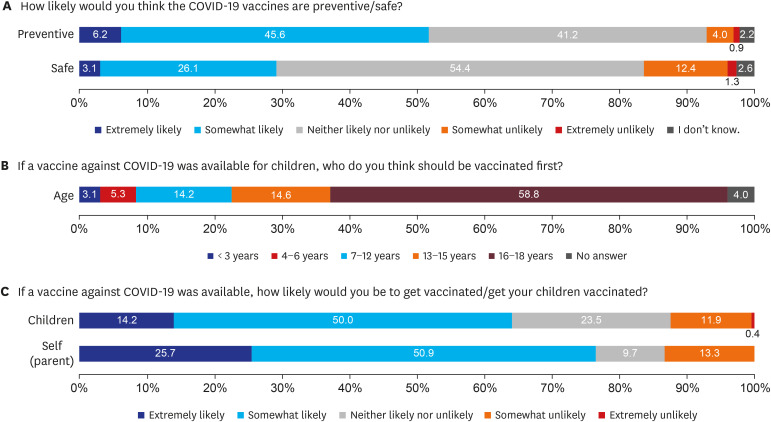
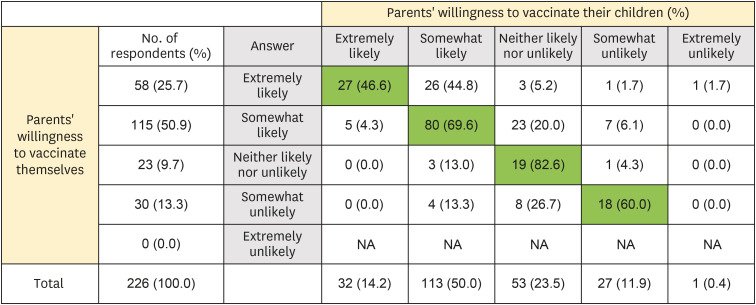
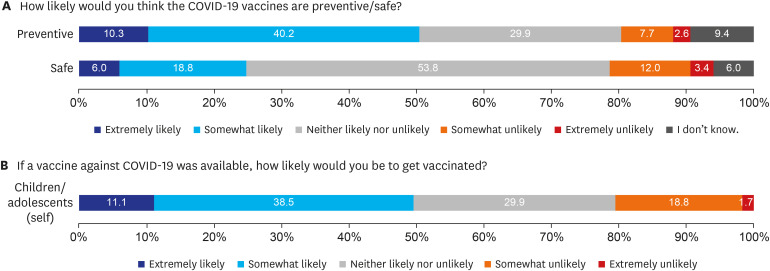
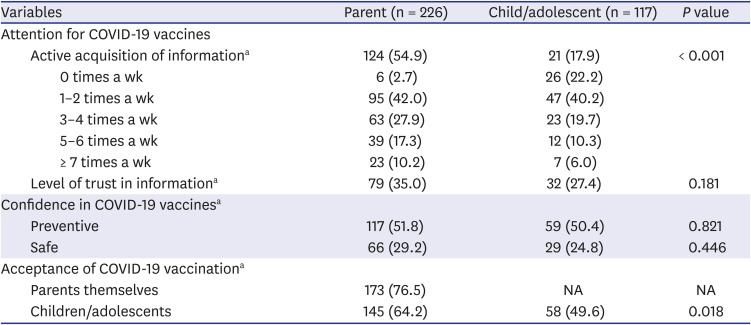
Fig. 2
Parental awareness and potential acceptability of COVID-19 vaccination for their children. (A) Confidence in the effectiveness and safety of COVID-19 vaccines. (B) The prior age group of COVID-19 vaccination for children. (C) Intention to vaccinate themselves and their children.
COVID-19 = coronavirus disease 2019.
![]()
Fig. 3
The agreement rate of intention to vaccinate parents themselves and their children.
NA = non-available.
![]()
Fig. 4
Children and adolescents' awareness and potential acceptability of COVID-19 vaccination. (A) Confidence in the effectiveness and safety of COVID-19 vaccines. (B) Intention to get COVID-19 vaccination.
COVID-19 = coronavirus disease 2019.
![]()
Table 3
Awareness of COVID-19 vaccines in participants
Values are presented as number (%).
COVID-19 = coronavirus disease 2019, NA = non-applicable.
aAnswer ‘extremely likely’ or ‘likely’ in the questionnaire.
![]()
Between parents who were willing to vaccinate their children and those who were not, there were no statistical differences in age of parents, level of education, family income, or numbers of their children. In the multivariate analysis, high confidence of COVID-19 vaccines safety (adjusted odds ratio [AOR], 4.87; 95% confidential interval [CI], 1.32–24.12), parents' willingness to vaccinate themselves (AOR, 19.42; 95% CI, 6.85–64.00), and awareness of the need for children's COVID-19 vaccination (AOR, 13.15; 95% CI, 4.77–41.27) were associated with determining factors intention to vaccinate their children (Table 4). However, history of tested for COVID-19 in themselves or family members was a negative factor associated with the intention to vaccinate their children (AOR, 0.26; 95% CI, 0.10–0.63).
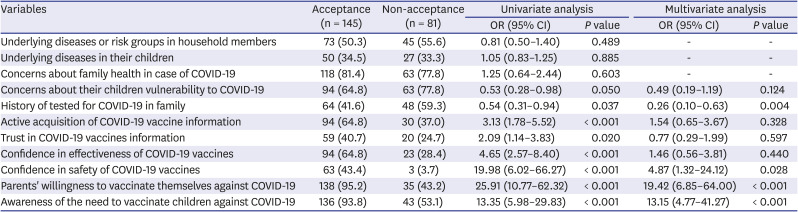
Table 4
Factors of parents' intention to vaccinate their children
Values are presented as number (%).
OR = odds ratio, CI = confidential interval, COVID-19 = coronavirus disease 2019.
![]()
DISCUSSION
This study determined the potential acceptance of COVID-19 vaccination for children in 226 parents and 117 children/adolescents using a questionnaire survey. Overall, 59.2% (64.2% of parents and 49.6% of children/adolescents) responded with “acceptable” regarding COVID-19 vaccination for children. There was a statistically significant difference in the intention to have COVID-19 vaccination for children between children/adolescents and parents (P = 0.018). Our study showed that parents' willingness to vaccinate themselves was the most significant factor in accepting COVID-19 vaccination for their children (AOR, 19.42; 95% CI, 6.85–64.0). In addition, high confidence in the safety of COVID-19 vaccines and the necessity of vaccinating children were significantly associated with the intention to vaccinate their children. To the best of our knowledge, survey regarding acceptance and attitudes towards children and adolescents' COVID-19 vaccination in South Korea has not been reported yet.
According to a recent survey on 1,000 adults over age 18 years that was performed from April 27 to April 29, 2021, commissioned by Korean government, 61.4% of 943 unvaccinated respondents said they were willing to be vaccinated.12 The main reason for vaccination was COVID-19 prevention for the family (80.8%) and the main reason for hesitancy was concern about adverse events after vaccination (84.1%). These respondents obtained COVID-19 vaccines-related information through media reports (79.1%) or government announcement (66.8%). The majority (69.4%) responded that harmful effects of vaccines-related false information were serious. A recent report regarding global attitudes towards a COVID-19 vaccines showed that concerns about side effects and insufficient testing of vaccines were main barriers to vaccine uptake.13 Of respondents from different countries included in that report, trust in vaccines (47%) and confidence in health authorities (42%) were the lowest in Korean respondents as of mid-May of 2021. Results of our study were consistent with those of these surveys. Based on parents' responses, trust in COVID-19 vaccines-related information was low (35.0%), and 70% of parents had concerns about vaccine safety. However, acceptance of COVID-19 vaccination for themselves was higher (76.5%) than in the recent government survey.12
In an online survey research performed in July 2020, COVID-19 vaccine refusal rate was predicted to be 29.4% in the French working-age population.14 COVID-19 vaccine refusal and hesitancy were significantly associated with female gender, age with an inverted U-shaped relationship, lower educational level, poor compliance with recommended vaccinations in the past, and no report of specified chronic conditions.14 El-Elimat et al.15 conducted a study in November 2020 and reported that the public acceptability of COVID-19 vaccines was 37.4% in Jordan. Participants who believed that vaccines are generally safe were more likely to accept COVID-19 vaccines (AOR, 9.258; 95% CI, 6.020–14.237).
There are a few studies regarding COVID-vaccine hesitancy or resistance among parents.161718192021222324 Results of reported studies were similar to those of the present study. Among parents surveyed in the US, 40-60% planned to get their children vaccinated.25 Main reasons for not vaccinating were as followings: “not sure it will be safe (59%),” “vaccine developed too quickly (59%),” and “don't trust information being published about the vaccine (48%).” Parents reported similar or slightly lower intent to vaccinate their children compared to intent to vaccinate themselves. A survey of 971 members of a national parents organization conducted between March 7 and March 12, 2021 showed that while 70% of parents planned to get or have already received the vaccine, only 58% of parents said they would probably or definitely vaccinate their children.23 Parents' willingness to vaccinate their children closely matched their willingness to get vaccinated themselves.21 A Turkish study conducted in February 2021 showed that 36.3% and 59.9% of parents were willing to vaccinate their children and themselves, respectively.26 Parents' willingness (AOR, 24.8; 95% CI, 10.9–56.6) and positive attitudes towards COVID-19 vaccine were factors that increased the acceptance of COVID-19 vaccine for their children. In a German study using data collected in May 2020, 58% of parents intended to get COVID-19 vaccination and 51% intended to have their children vaccinated.20 Significant predictors for the intention to vaccinate their children included higher educational level (AOR, 1.99; 95% CI, 1.26–3.34), stronger confidence in one's knowledge about safety measures (AOR, 1.23; 95% CI, 1.07–1.41), and regular information seeking about COVID-19 pandemic (AOR, 1.22; 95% CI, 1.00–1.48). Presence of family member in risk group (AOR, 0.59; 95% CI, 0.36–0.99) and stronger beliefs that policy measures were exaggerated (AOR, 0.60; 95% CI, 0.49–0.76) were associated with a lower intention to vaccinate their children.
The study of BNT162b2 vaccine in 12–15 year-old recipients reported that the observed vaccine efficacy was 100% (95% CI, 75.3–100) with a favorable safety profile.27 The manufacture of mRNA-1273 vaccine announced on 6 May 2021 that the vaccine was 96% effective for adolescents ages 12–17 years after at least one dose without having serious safety concerns.28 The American Academy of Pediatrics recommends COVID-19 vaccination for all children and adolescents 12 years of age and older who do not have contraindications for using a COVID-19 vaccine authorized for use for this age group.29 The technical report of EU/EEA has noted that because COVID-19 is typically milder in healthy children and adolescents, vaccine uptake in older age groups should continue to be given a priority before targeting adolescents as a whole.9 Vaccination of adolescents who are at high risk of severe COVID-19 should be prioritized in the same way as vaccination for people in other age groups who are at a high risk of having a severe disease. The decision-making process for allocation and distribution of the limited number of COVID-19 vaccines is imperative and flexibility in adapting to strategies is essential as new information is constantly emerging.30
Our study has some limitations. Since this survey was performed in one region of South Korea, it has limitations in reflecting the nationwide situation. In addition, selection bias could not be ruled out because the recruitment targeted survey subjects at tertiary university hospitals. The participants are likely to be associated with high risks for severe COVID-19, which may affect the intention to vaccinate against COVID-19. However, our study results were quite consistent with a recent national survey and previously reported studies. In addition, this study included children and adolescents aged 10–18 years in the survey subjects to investigate their intention to vaccinate themselves. There has been no report to explore children and adolescents' intention to vaccinate themselves.
In conclusion, this study provides insight into how parents are thinking about COVID-19 vaccine for their children in South Korea. Our findings could be referenced in establishing policies for COVID-19 vaccination for children in the future.
 XML Download
XML Download