

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Predicting the probability of survival of preterm infants can be of great value in guiding management in high-risk pregnancies. Although survival is affected by numerous factors, birth weight (BW) and gestational age (GA), alone or in combination, are the most widely used.12 Recent advances in neonatal intensive care have remarkably improved the survival of premature infants born at periviable gestational ages.3 In Korea, the survival rate of infants born before 24 weeks of gestation increased from 3% in 2002 to 34% in 2013–2014.4 However, as a predictive factor for survival, GA is not always accurate, especially for mothers who do not undergo an early ultrasonographic assessment.5 BW, measured directly and immediately after birth, is an objective indicator that dictates survival.
BW < 500 g appears to be a lower limit for viability6; however, an evaluation of data from nationwide neonatal cohorts is necessary to provide data focused on changing the viability limit of preterm infants. Multicenter cohort studies that determined early outcomes in infants with BW < 500 g have been reported in several countries,789 including a recent study that used a nationwide cohort database in Japan.10 Nonetheless, wide variations in the viability of premature infants persist among countries.11
The Korean Neonatal Network (KNN) is a nationwide, prospective web-based cohort registry for very low birth weight infants (VLBWIs) in Korea.12 Although the survival rates in VLBWIs were provided in 2019 through the KNN,13 studies on the outcome of infants with BW < 500 g in Korea are limited to a single-center experience.14 Therefore, this study aimed to investigate the rates of survival and early morbidities of infants with BW < 500 g using the KNN database.
METHODS
Study population
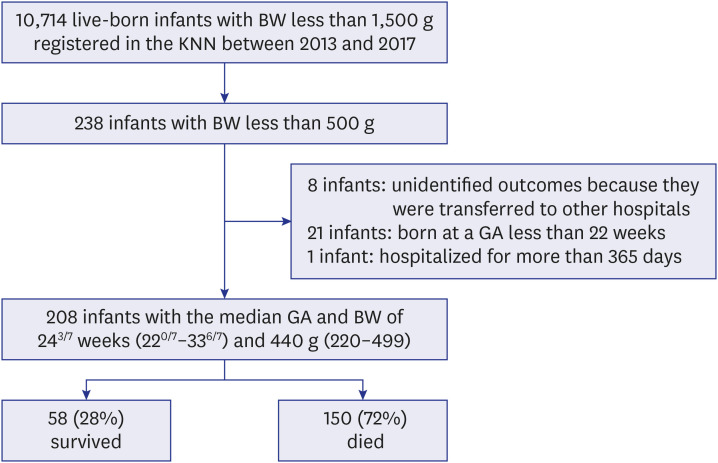
Patient data were obtained from the KNN, established by the Korean Society of Neonatology and Korea Centers for Disease Control and Prevention in 2013. This database prospectively registered all of the clinical information of VLBWIs admitted to the 69 voluntarily participating neonatal intensive care units (NICUs), covering greater than 80% of preterm infants. A total of 238 live-born infants with BW < 500 g born between January 1, 2013, and December 31, 2017, were eligible (Fig. 1). Data on stillbirth and intrapartum death were not registered in the KNN. The following infants were excluded: 8 infants who had unidentified outcomes because they were transferred to other hospitals; 21 infants born at a GA < 22 weeks; and 1 infant who was hospitalized for more than 365 days.
Variables and outcomes
Maternal data, such as mode of delivery, time of birth (categorized as daytime, from 7 am to 7 pm, and nighttime, from 7 pm to 7 am), any use of antenatal steroids, mode of conception, diabetes, preeclampsia, chorioamnionitis confirmed by histopathology, and ruptured membranes were collected. Infant characteristics, including gestational age, birth weight, sex, small for gestational age according to the Fenton preterm growth charts,15 multiple gestations, 1-minute and 5-minute Apgar scores, resuscitation information in the delivery room, body temperature at admission to the NICU, and laboratory values within 1 hour after birth, were also obtained to determine their association with survival to discharge in infants with BW < 500 g. Data on neonatal outcomes included respiratory distress syndrome (RDS), air leak syndrome, massive pulmonary hemorrhage, bronchopulmonary dysplasia (BPD) defined by the National Institute of Health (NIH) consensus definition,16 duration of invasive mechanical ventilation, patent ductus arteriosus (PDA), intraventricular hemorrhage (IVH) according to Papile et al.'s criteria,17 post hemorrhagic hydrocephalus, periventricular leukomalacia, sepsis, stage 2 or higher necrotizing enterocolitis (NEC) according to Walsh and Kliegman's criteria,18 idiopathic intestinal perforations, duration of total parenteral nutrition (TPN), any retinopathy of prematurity (ROP), brain stem auditory evoked potential abnormality, transfusion of packed red blood cells, duration of hospitalization, and mortality.
Statistical analysis
Data were statistically analyzed using R (version 3.6.1; R Foundation for Statistical Computing, Vienna, Austria). We found the fixed variables among colinear variables after confirming multiple linearities. These variables were adjusted through multivariable Cox proportional hazards analysis, and multiple imputations were used to handle missing data in body temperature. The adjusted odds ratio and 95% confidence interval for each possible risk factor were calculated. P values < 0.05 were considered statistically significant. A comparison between the cumulative survival rate according to the BW groups was performed by Kaplan-Meier analysis.
RESULTS
A total of 208 infants were included in the study, with a median GA and BW of 243/7 weeks (range, 220/7–336/7) and 440 g (range, 220–499), respectively. Of the total infants, 58 (28%) survived to hospital discharge, and 150 died during the NICU stay (Fig. 1). The survival rates for these infants were as follows: 0% for < 300 g, 20% for 300–399 g, and 30% for 400–499 g.
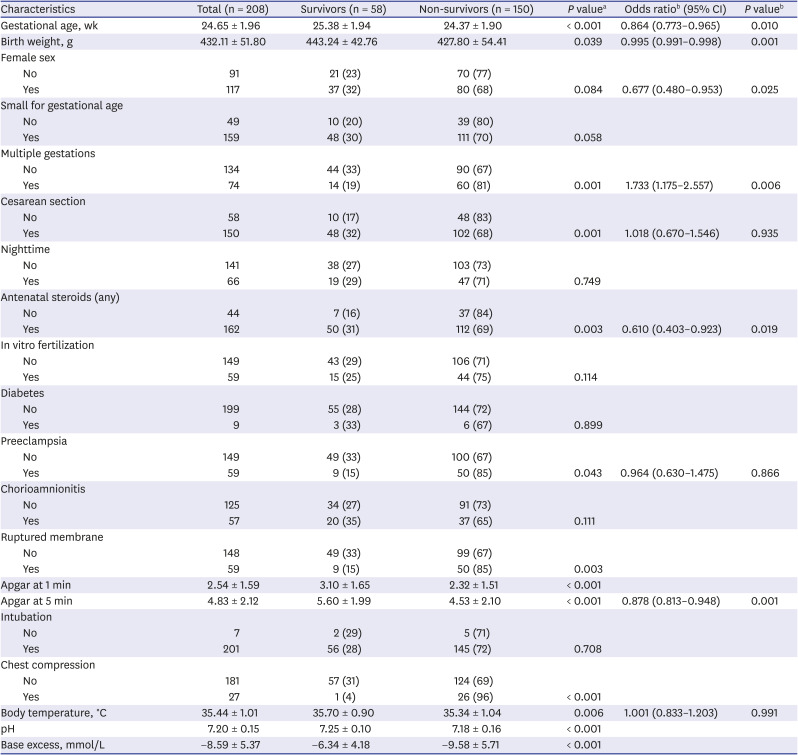
Table 1 presents the perinatal characteristics of the survivors and non-survivors. The mean GA and BW in the survivors were higher than those in the non-survivors. The proportions of multiple gestations, preeclampsia, and premature ruptured membrane were lower in the survivors. Surviving infants were delivered by cesarean delivery and exposed more frequently to antenatal steroids than non-surviving infants. The survivors had a higher Apgar score at 1 and 5 minutes, with lower proportions requiring chest compression in the delivery room. The mean body temperature of the surviving infants was higher, and the pH and base excess values in the surviving infants were higher than those in the non-surviving infants. After correction through multivariable Cox regression analysis, survival to discharge was associated with longer gestation, higher BW, female sex, singleton gestation, any use of antenatal corticosteroids, and higher Apgar score at 5 minutes.
Table 1
Perinatal characteristics associated with survival to discharge in infants with birth weight < 500 g
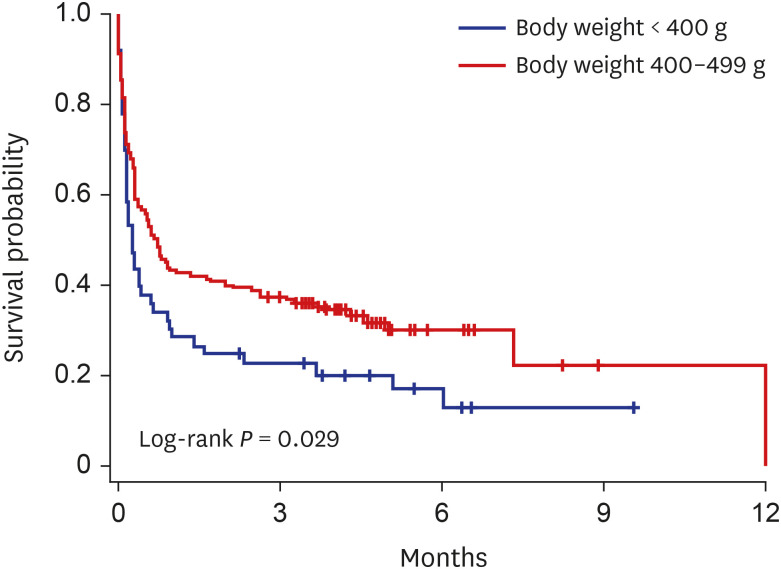
The survival curves were plotted by the Kaplan–Meier method in infants according to the BW categories of < 400 g and 400–499 g (Fig. 2). The overall survival rates were significantly different between the BW groups (log-rank P = 0.029), but there was no significant difference in the incidence of any morbidity between BW groups (Table 2).
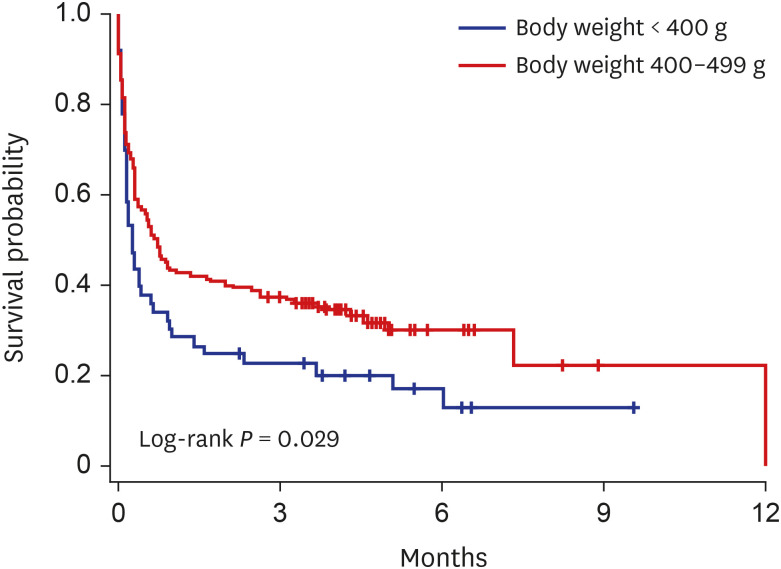
Table 2
Early outcomes of surviving infants with different birth weights
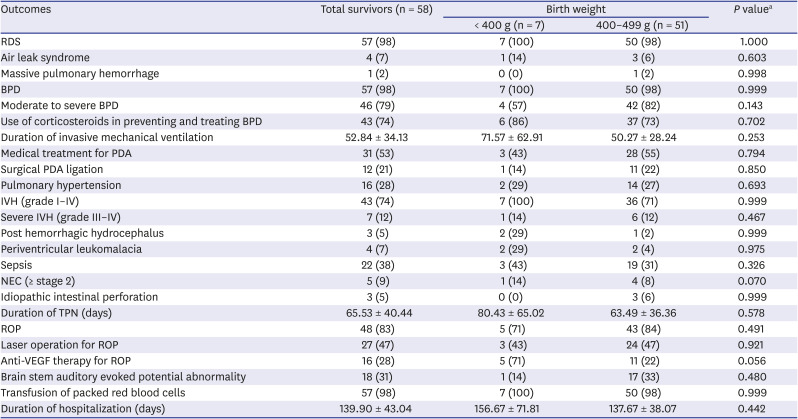
Data presented as the number (percentage) or as the mean ± standard deviation.
RDS = respiratory distress syndrome, BPD = bronchopulmonary dysplasia, PDA = patent ductus arteriosus, IVH = intraventricular hemorrhage, NEC = necrotizing enterocolitis, TPN = total parenteral nutrition, ROP = retinopathy of prematurity, VEGF = vascular endothelial growth factor.
aMultivariate analysis adjusted for gestational age, sex, multiple gestations, any use of antenatal steroids, and Apgar at 5 minutes.
Half of the deaths of infants with BW < 500 g occurred within a week of life, mainly due to cardiopulmonary and neurologic causes (Fig. 3). After 1 week of age, the proportion of infection and gastrointestinal disease has increased among the causes of death.
Fig. 3
Causes of death in infants with birth weight less than 500 g according to the timing of death.
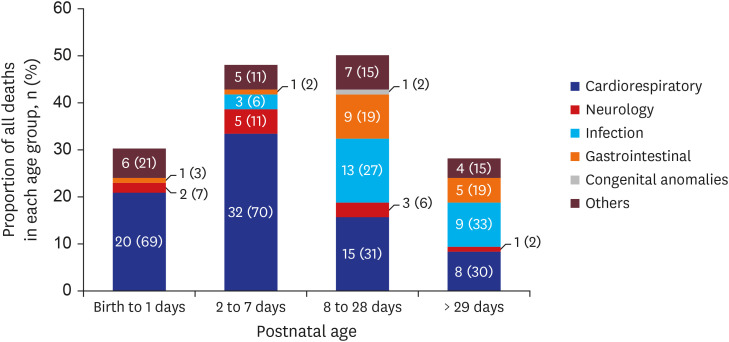
Table 2 shows the early outcomes in the surviving infants. Surfactant was used to treat RDS in most of the surviving infants and was administered prophylactically in the delivery room in most cases. BPD occurred in most of the surviving infants, and postnatal corticosteroids were administered systemically in 74% of all surviving infants to prevent and treat BPD. Intravenous ibuprofen was given in 53% of infants for treatment of PDA; 19% of administrations were prophylactic before the symptoms of PDA appeared. Additionally, 17% received medical treatment but did not respond, and 3% did not receive medical treatment despite symptoms of PDA and underwent surgical ligation. IVH occurred in 74% infants; 12% with grade III–IV, of which 42% had post hemorrhagic hydrocephalus. Stage 2 or more NEC was present in 9% of infants, and 5% had idiopathic intestinal perforation. The median duration of TPN was 59 days (range, 10–214) in surviving infants. In the infants diagnosed with ROP (83%), 33% received only laser photocoagulation, 10% received only anti-vascular endothelial growth factor therapy, and 23% received both.
The median length of hospital stay was 132 days (range, 69–291), and 53% of the discharged infants required assistive devices. Among the assistive devices, continuous pulse oximetry was used in 90%, continuous home oxygen therapy in 48%, tube feeding in 19%, stomas in 6%, and treprostinil sodium (Remodulin®) infusion pump for the treatment of pulmonary arterial hypertension in 3% of infants.
DISCUSSION
This study is the first to evaluate the survival rates along with the rates of major morbidities of infants with BW < 500 g using a population-based study in Korea. The results revealed that the overall survival of infants with BW < 500 g born from 2013 to 2017 in Korea was 28%, with high rates of severe morbidities observed. In addition, we found that higher survival rates were associated with longer gestation, higher BW, female sex, singleton gestation, any use of antenatal corticosteroids, and higher Apgar scores at 5 minutes.
The viability of premature infants has been shown to vary widely between different countries, although such relevant publications are based on different investigation periods.11 Therefore, it is necessary to recognize that the results of this study were derived from a 5-year data of infants with BW < 500 g, born in Korea from 2013 to 2017. In Korea, surfactants have been used since the 1990s, and new techniques, such as high-frequency oscillatory ventilation and inhaled nitric oxide therapy, were introduced in the 2000s.19 A previous study on the survival rate of VLBWIs born in Korea over 50 years shows that the survival rate continuously increased over time.4 Given the recent advances in neonatal care in Korea over the years, the results of this study are likely to change in the future. However, due to the short study period of 5 years in the present study, it was difficult to expect changes in the survival rate within this period.
In this study, the Cox model was used to adjust for imbalance in variables influencing survival to discharge in the infants with BW < 500 g. Survival to discharge was found to be significantly associated with longer gestation, higher BW, female sex, singleton gestation, any use of antenatal corticosteroids, and higher Apgar scores at 5 minutes. These associations are generally consistent with the findings of previous studies.1202122232425 It is well known that females exhibit a survival advantage compared to males.20 O'Driscoll et al.21 found that the female advantage is multifactorial, with hormonal, genetic, and immunological differences. Moreover, twins have been shown to have higher rates of mortality compared with singletons in the study group. Although the etiology of these differences has not been fully determined, it likely involves growth restriction as a key risk factor for respiratory morbidity in preterm infants.22 The use of antenatal corticosteroids is one of the most effective perinatal care for improving neonatal outcomes of preterm infants.23 In the study by Carlo et al.,24 as in this study, the benefits of antenatal corticosteroids therapy across the ranges of gestational ages around the limits of viability were observed. The Apgar score was developed primarily to assess term infants, and the American Academy of Pediatrics recommended that the Apgar score should not be used in preterm infants to predict individual neonatal mortality.25 However, in a recent study, Apgar scores at 5 minutes provided prognostic information about neonatal survival among preterm infants across gestational age strata.26
The Neonatal Research Network of Japan, which has the highest survival in infants with BW < 500 g, showed high rates of serious morbidities in the NICU, including moderate to severe BPD in 58%, PDA ligation in 13%, severe IVH in 8%, sepsis in 20%, stage 2 or higher NEC in 8%, and laser coagulation for ROP in 48%.10 In the present study, the incidence of morbidities in early infancy were higher than those obtained in that report, and more than half of the infants required assistive devices at discharge. Although advances in perinatal-neonatal medicine can help to overcome the biological limitations of premature infants, further support is needed to improve survival and morbidity rates in Korea. Among the survival factors identified through this study, the Apgar score at 5 minutes is considered as a task to be challenged as a neonatologist. In the neonatal resuscitation program, more specialized efforts will be needed for preterm infants and even tiny infants with BW < 500 g.
There are several limitations to our study. First, the long-term outcome for each infant was not analyzed, and a follow-up study is crucial as the long-term records accumulate. Second, we were unable to identify the institutional variations in intensive care for periviable infants.27 Even in one hospital, NICU staffing varies depending on the time of birth. Taking this into account, the time of birth was evaluated among the risk factors related to survival, but there was no significant difference by day/night.28 Lastly, given the study of periviable infants, stillborn infants should also be considered.
The strength of this study lies in evaluating the infants with BW < 500 g using a multicenter cohort study in Korea. In addition, a more detailed analysis was demonstrated than has been reported by previous studies in several countries.
In conclusion, despite advances in perinatal-neonatal care, infants with BW < 500 g are still at the limit of survival and have high morbidities. Thus, it is necessary to make more effort to further improve neonatal outcomes of infants with BW < 500 g.
 XML Download
XML Download