

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The coronavirus disease 2019 (COVID-19) pandemic has affected more than 161 million worldwide, and caused more than three million deaths.1 Children and adolescents are generally at low risk of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection, and if they become infected, the disease is likely to be mild.2345 However, some children and adolescents have had severe experiences with COVID-19, and a few have died.3678910 As of May 6, 2021, over 3.85 million children have tested positive for COVID-19 in the United States, representing 14% of all cases. In state-level reports, children accounted for 0.00–0.21% of all COVID-19 deaths.3 In South Korea during the same period, 14,341 children 0 to 19 years of age were confirmed with COVID-19. However, no COVID-19-related mortality among Korean children have been reported so far.11
Remdesivir is an antiviral drug with potent in vitro activity against a range of RNA viruses including SARS-CoV-2.12 Remdesivir is recommended for patients with severe COVID-19 but is not necessary for most pediatric COVID-19 patients.213 Here, we reported on a 9-year-old boy with COVID-19 pneumonia who developed respiratory distress and was successfully treated with remdesivir and dexamethasone.
CASE DESCRIPTION
On May 4, 2021, a 9-year-old boy confirmed with COVID-19 was referred to our hospital. Fig.1. shows the timeline before hospitalization to our hospital. Because his uncle, whom he had contact with at a family reunion, was confirmed with asymptomatic COVID-19, he had been in self-quarantine since 10 days earlier. He had a cough on the seventh day of self-quarantine (nine days after the last exposure) and developed a fever of ≥ 38°C the next evening. He was eventually confirmed with COVID-19 12 days after the last exposure and was hospitalized in a designated hospital. Upon admission to the outside hospital, the initial chest X-ray showed diffuse pneumonic consolidations in both lung fields and chest computer tomography was performed on the same day (Fig. 2). He had a fever of up to 40.5°C, cough, and sputum, but no dyspnea, and his saturation of percutaneous oxygen (SpO2) was maintained at ≥ 95% on room air. However, the next day, his fever and cough became worse, and he complained of respiratory difficulty.
Fig. 1
Timeline before hospitalization at our hospital. The index case was the patient's uncle, who was asymptomatic and tested for COVID-19 because there was a confirmed case at the workplace. The patient's mother was also confirmed with asymptomatic COVID-19 on the day of the patient's hospitalization.
COVID-19 = coronavirus disease 2019, HD = hospital day.

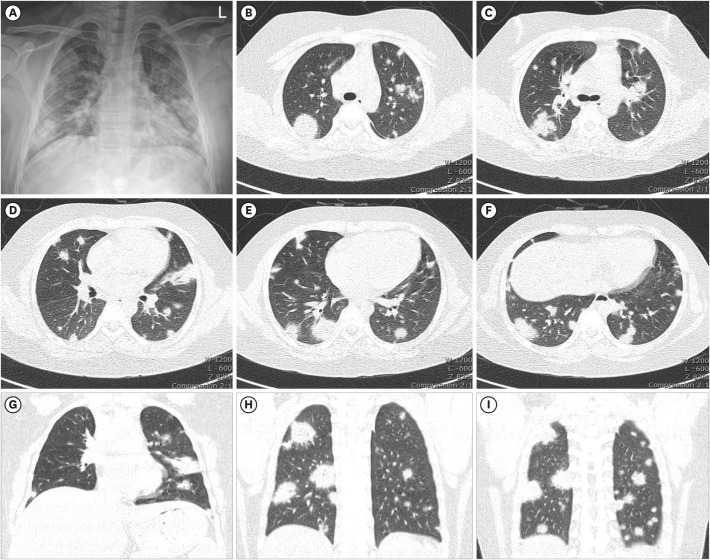
Fig. 2
Chest X-ray and CT images performed on the day coronavirus disease 2019 was confirmed. (A) The chest X-ray showed diffuse pneumonic consolidations in both lung fields. (B-I) The chest CT showed several small round and patchy consolidations diffusely scattered in the peripheral, subpleural, and peribronchial areas of both lungs.
CT = computed tomography.
The patient was previously healthy and had no specific medical history other than obesity (body mass index, 27.6, 99.8th percentile; body weight, 62 kg, 99.8th percentile; height, 150 cm, 97.3rd percentile). The initial vital signs at our hospital showed a blood pressure of 124/106 mmHg, pulse rate of 133 beats per minute, respiratory rate of 29 breaths per minute, a body temperature of 38.6°C, and an SpO2 of 95–98% on room air. The initial laboratory results were as follows: white blood cell count 6,760/μL (13.9% lymphocytes), hemoglobin 11.7 g/dL, platelet count 238,000/μL, C-reactive protein 8.29 mg/dL (range, 0–0.5), procalcitonin 0.86 ng/mL (range, 0-0.05), and D-dimer 0.7 μg/mL (range, 0-0.5). The cardiac biomarkers were normal. The results of arterial blood gas analysis were pH 7.48, pCO2 31 mmHg, pO2 103 mmHg, and O2 saturation 98%. However, he gradually complained of respiratory difficulty starting on the night of hospitalization day and had oxygen desaturation. Oxygen supplementation was needed to maintain an SpO2 of ≥ 95%. He received supplemental oxygen via nasal prongs initially. The clinical course and selected relevant laboratory parameters are shown in Fig. 3.
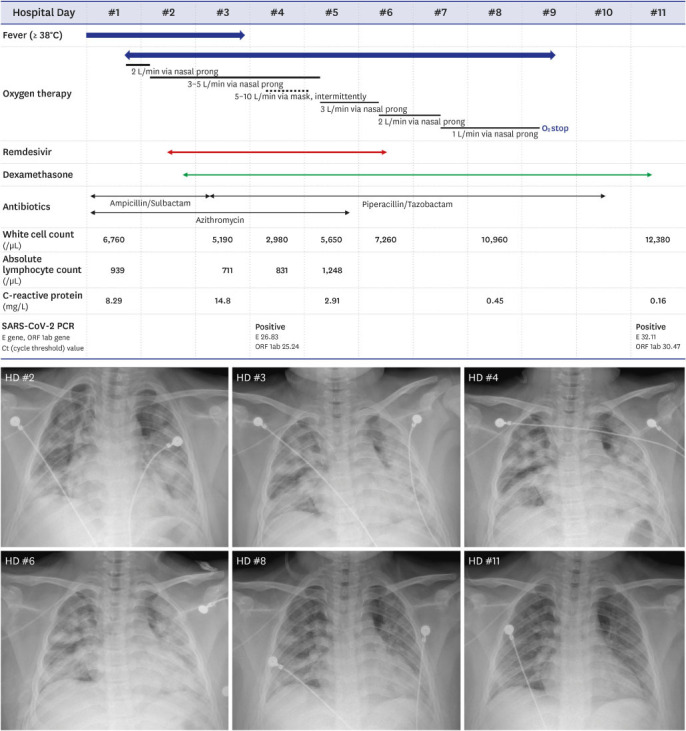
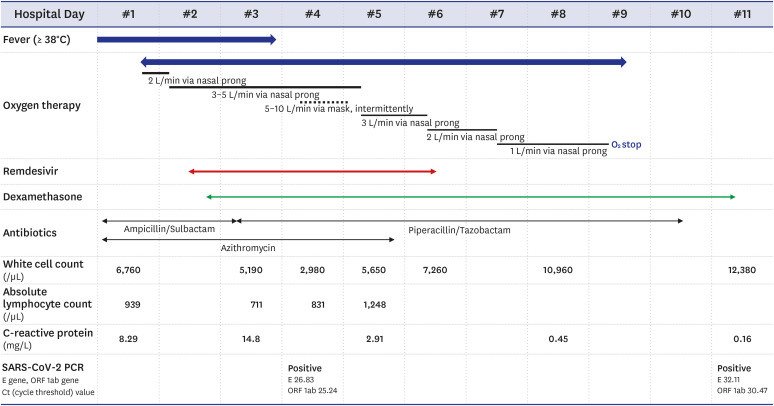
Fig. 3
Timeline of clinical course, treatment and laboratory findings.
SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2, PCR = polymerase chain reaction.
On hospital day 2, he developed markedly increased tachypnea (respiratory rate up to 48 breaths per minute) and decreasing SpO2, thus requiring oxygen enrichment (up to 5 L flow of 100% oxygen). The chest X-ray showed the progression of pneumonia (Fig. 4). We assessed the patient's COVID-19 severity based on clinical criteria,13 which was regarded as severe. Remdesivir is suggested for children with severe COVID-19, so remdesivir administration was initiated (body weight ≥ 40 kg: 200 mg loading dose on the first day, followed by 100 mg every 24 hours intravenously). Although hypotension was not noted, other vital signs remained unstable. He had sustained and recurrent fever with poor response to antipyretics, tachycardia, tachypnea, and repeated need for increase in oxygen. He complained of severe general aches, and the C-reactive protein level was high. We decided to administer corticosteroids. He received dexamethasone at 6 mg (0.15 mg/kg, maximum dose 6 mg) once daily for 10 days.
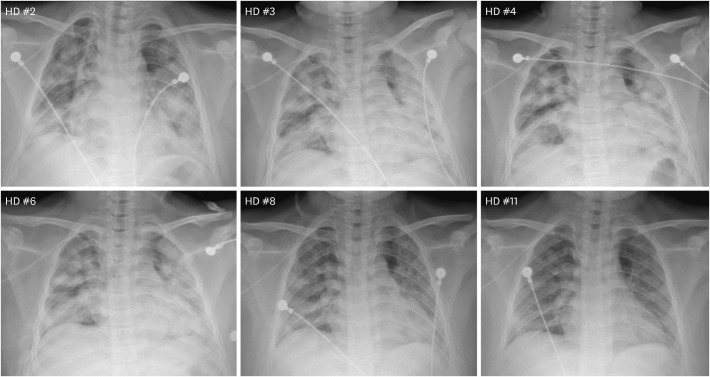
Fig. 4
Serial chest X-rays of the patient. The patient received remdesivir therapy from HD 2 to 6.
HD = hospital day.
The patient showed defervescence by hospital day 4. However, he complained of severe cough and had frequent desaturation of SpO2. In the episodes of deterioration, his oxygen requirement increased up to 10 L/min and slowly recovered. There were no significant findings in testing for additional bacterial and viral respiratory pathogens. The echocardiography results were unremarkable. The five days of remdesivir therapy were finished on hospital day 6. Hepatic and renal function tests were monitored daily during remdesivir therapy, and there were no adverse events. Although there was no significant improvement in the chest X-ray on hospital day 6, his oxygen requirements were gradually weaning. On hospital day 8, the chest X-ray showed a marked improvement in pneumonic consolidations in both lung fields (Fig. 4), and the C-reactive protein level was normal. Supplemental oxygen was stopped on hospital day 9.
The follow-up polymerase chain reaction (PCR) test for SARS-CoV-2 on hospital day 18 was equivocal (negative for E gene; positive for ORF 1ab; cycle threshold value, 35.11). However, no pneumonic consolidations were noted on the follow-up chest X-ray, and his symptoms had nearly resolved. The patient was discharged from the hospital on day 21.
DISCUSSION
We report a case of severe COVID-19 in a previously healthy 9-year-old boy in Korea. This child developed respiratory distress as his pneumonia progressed rapidly. He received remdesivir treatment and recovered successfully.
There is no international consensus on the classification of the disease severity of pediatric COVID-19. In the early phase of the COVID-19 pandemic, radiological criteria were considered an essential factor in the classification of disease severity. However, radiographic infiltrates are common, even among well-appearing, clinically stable children with COVID-19. Therefore, a severity classification that includes a radiological diagnosis of pneumonia is not appropriate for children.14 Several recent reports have used clinical criteria, particularly respiratory support requirements, to define illness severity categories.2121315 In multicenter interim guidance on the use of remdesivir for children with COVID-19, severe illness is defined as patients with new or increase from baseline supplemental oxygen requirement without need for new or increase in baseline noninvasive/invasive mechanical ventilation.13 Our patient's disease category was assessed as severe COVID-19 based on the guidance.
While most pediatric COVID-19 patients experience mild illness, a small proportion develops severe illness associated with adverse clinical outcomes. A multinational European cohort of 582 pediatric COVID-19 cases showed that 48 cases (8%) required pediatric intensive care unit (PICU) admission and four children died.4 In a retrospective cohort study of 12,306 pediatric COVID-19 patients in the United States, the frequency of hospitalization was 5.5% (672 cases). Among those who were hospitalized, 17.6% required PICU admission and 4.1% required mechanical ventilation. There were ≤ 10 deaths.5 In data on 3,836 Italian pediatric COVID-19 cases from the national case-based surveillance system, the overall hospitalization rate and PICU admission rate were 13.3% and 3.5%, respectively.16 As of June 18, according to the Korea Disease Control and Prevention Agency report, there was a patient aged 10–19 years old with severe-critical status.17
Data to clearly establish the risk factors for severe COVID-19 in children are limited.679101819 In a European cohort study, the significant risk factors for ICU admission were age younger than one month, male gender, pre-existing medical conditions, and the presence of lower respiratory tract infection signs or symptoms at presentation.4 In a study of children with COVID-19 admitted to North American PICUs, most had underlying conditions, with obesity, chronic lung disease, and prematurity the most prevalent.19 Our patient had no underlying medical conditions other than obesity. Data from several studies suggested that overweight or obesity was an independent risk factor for severe COVID-19 in adults.202122 There is insufficient evidence to definitively support isolated overweight or obesity as a risk factor for severe COVID-19 in children. However, current reports indicated that obesity was prevalent among hospitalized pediatric COVID-19 patients, particularly in a critically ill cohort.101923
Most children with COVID-19 will not require any specific therapy. Children with mild or moderate COVID-19 can be managed with supportive care alone. The established optimal therapy for children with severe COVID-19 is unknown. In the absence of adequate data, guidance for the treatment of pediatric COVID-19 is mostly extrapolated from recommendations for adults with COVID-19.212 WHO recommends against the use of remdesivir in COVID-19 patients.24 However, remdesivir is recommended in other guidelines for children with severe COVID-19.213 In the guidelines from the U.S National Institutes of Health, remdesivir is recommended for hospitalized children aged ≥ 12 years with COVID-19 who have risk factors for severe diseases and have an emergent or increasing need for supplemental oxygen. In consultation with a pediatric infectious disease specialist, remdesivir can be considered for hospitalized children of all ages with COVID-19 who have an emergent or increasing need for supplemental oxygen.2 Remdesivir has not been evaluated in clinical trials for children, and there have been no results from systemic evaluations of pharmacokinetics, efficacy, or toxicity in younger children, although studies are ongoing (NCT04431453).2 Recently, a report of the compassionate use of remdesivir in children with severe COVID-19 was published by Goldman et al.25 The report showed that among 77 children treated with remdesivir for severe COVID-19, most recovered and the rate of serious adverse events was low.25 Remdesivir may cause adverse events such as transaminase elevations, hypersensitivity reactions and bradycardia.12 Except the report by Goldman et al.,25 there are only a few case reports of children with COVID-19 treated with remdesivir.26272829 Remdesivir became available for use in July 2020 in Korea. To our knowledge, no pediatric case of severe COVID-19 treated with remdesivir has been reported in Korea.
Our patient received dexamethasone for 10 days as well as remdesivir therapy. We gave significant consideration to decision-making regarding dexamethasone therapy for this patient. In current guidelines, dexamethasone is recommended for children in critical COVID-19 with evidence of hyperinflammation.15 However, we assessed the status of our patient who was rapidly progressing toward “critical” category. Eventually, the patient was successfully treated with remdesivir and dexamethasone.
The proportion of severe or critical disease is small in children with COVID-19. However, a small proportion of children with COVID-19 also develop progressive respiratory disease, like our patient. Further research is needed to establish the optimal treatment for children with severe or critical COVID-19.
 XML Download
XML Download