

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The term nontuberculous mycobacteria refers to all mycobacterial species other than the Mycobacterium tuberculosis complex species and Mycobacterium leprae. Nontuberculous mycobacterial pulmonary disease (NTM-PD) is the most common NTM infection in humans.12 The incidence of NTM-PD has recently been increasing worldwide, and the resulting socioeconomic losses have been worsening.34567 Accurate diagnosis and appropriate treatment are pivotal in controlling NTM-PD.
The diagnostic criteria for NTM-PD comprise clinical, radiological, and microbiological elements.12 To satisfy the microbiological criteria, isolation of nontuberculous mycobacteria from at least two separately expectorated sputum samples is required. For patients whose sputum culture results are consistently negative or who are unable to produce adequate sputum, bronchoscopy is recommended for diagnosis.89
Collecting post-bronchoscopy sputum (PBS) in addition to bronchoscopic specimen contributes to improved diagnostic yield in patients with suspected pulmonary tuberculosis (PTB).10111213 Thus, PBS collection is recommended in patients with suspected TB who undergo bronchoscopy.1415 However, it remains unclear whether collecting PBS can increase the diagnostic yield of NTM-PD. In this study, we aimed to clarify whether PBS collection can improve diagnostic yield in patients with suspected NTM-PD whose sputum nontuberculous mycobacteria culture results are consistently negative or who are unable to produce adequate sputum.
Go to : 
METHODS
Study population
We performed a retrospective study including patients with suspected NTM-PD who underwent diagnostic bronchoscopy from January 1, 2017, to June 30, 2020, at the Seoul National University Hospital. Patients with suspected NTM-PD were defined as those who satisfied the clinical and radiographic criteria for NTM-PD12 but had consistently (≥ 2 times) negative sputum culture results or were unable to produce adequate sputum. Suspicion of NTM-PD was determined by board-certified duty physicians. Patients for whom nontuberculous mycobacteria were cultured from sputum collected before bronchoscopy or from whom PBS was not collected were excluded from the study. Patients included in the study were divided into the sputum culture-negative and scanty sputum groups because we assumed that these two groups could be different clinically. The sputum culture-negative group was defined as patients with negative sputum nontuberculous mycobacteria culture results obtained at least twice before bronchoscopy. The scanty sputum group was defined as patients who were unable to produce adequate sputum for nontuberculous mycobacteria culture.
Data collection
We retrospectively reviewed clinical records and collected patient data, including age, sex, body mass index (BMI), smoking status, symptoms of NTM-PD (e.g., cough, sputum expectoration, dyspnea, fever, hemoptysis, weight loss, night sweating), previous pulmonary TB treatment history, presence of underlying lung disease (chronic obstructive pulmonary disease, asthma, interstitial lung disease), acid-fast bacilli (AFB) smear results, and bronchial washing specimen and PBS mycobacterial culture results. Radiographic subtypes were classified by two board-certified pulmonologists as nodular bronchiectasis, upper lobe cavitary lesions, and unclassifiable.
Bronchoscopy and PBS collection
Bronchoscopy was performed by full-time faculty staff or fellows specializing in respiratory medicine. At least two well-trained nurses assisted in the procedure. A 6.0-mm-diameter bronchoscope (model BF-1T260; Olympus Optical Co, Tokyo, Japan) and a 4.9-mm-diameter bronchoscope (model BF-260, Olympus Optical Co) were used for the examination. Oral insertion was performed via a mouthpiece. All patients underwent bronchial washing at the clearest lesion suggestive of NTM-PD on chest computed tomography (CT). Sterile normal saline (20–40 mL) was injected into the target lesion and the specimen aspirated via bronchoscope. PBS was collected within 30 minutes of bronchoscopy.
Microbiological evaluation
AFB staining as well as bronchial washing specimen and PBS mycobacterial cultures were performed according to the British Thoracic Society (BTS) and American Thoracic Society/Infectious Disease Society of America (ATS/IDSA) guidelines.116 Both the bronchial washing and sputum specimens were inoculated into BACTEC MGIT 960 liquid media (Becton, Dickinson and Company, Franklin Lakes, NJ, USA) and Ogawa solid media (Shinyang, Seoul, Korea) for mycobacterial culture. Culture-positive colonies were analyzed to identify the nontuberculous mycobacteria species using 16S ribosomal RNA1 and rpoB gene sequencing.17
Statistical analysis
Continuous variables are presented as medians with interquartile range (IQR) and analyzed using Mann-Whitney U test. Categorical variables are descripted as numbers with percentages and analyzed using χ2 or Fisher's exact test. AFB smear and mycobacterial culture positivities were calculated on the basis of the ratio of the number of positive results to the total number of results in each group. An “exclusively positive culture” was defined as only one culture being positive, with the other being negative, among the bronchial washing and PBS specimens. The difference in the positivity before and after performing PBS culture test (the additional yield of PBS) was examined for statistical significance using McNemar's test. A P value of < 0.05 was considered significant. SPSS ver.26 (IBM Corp., Armonk, NY, USA) was used for statistical analysis.
Ethics statement
The study protocol was approved by the Seoul National University Hospital Institutional Review Board (2003-070-1108), and the requirement for written informed consent was waived. This study was conducted in accordance with the amended Declaration of Helsinki.
Go to :
RESULTS
Patient characteristics
During the study period, a total of 151 patients with suspected NTM-PD underwent bronchoscopy for diagnosis. Among them, six patients for whom nontuberculous mycobacteria were cultured from sputum collected before bronchoscopy and four patients from whom PBS was not collected were excluded. Consequently, 141 patients were included in the final analysis (Fig. 1).

The median patient age was 63 years (IQR, 58–70); 95 patients (67.4%) were females, and 103 patients (73.0%) were never-smokers. The sputum culture-negative group included 39 patients (27.7%), and the scanty sputum group included 102 patients (72.3%) (Fig. 1). There were no significant between-group differences in sex, age, BMI, smoking status, and previous pulmonary TB treatment history. Nodular bronchiectasis was the most common radiographic subtype in both groups (Table 1).
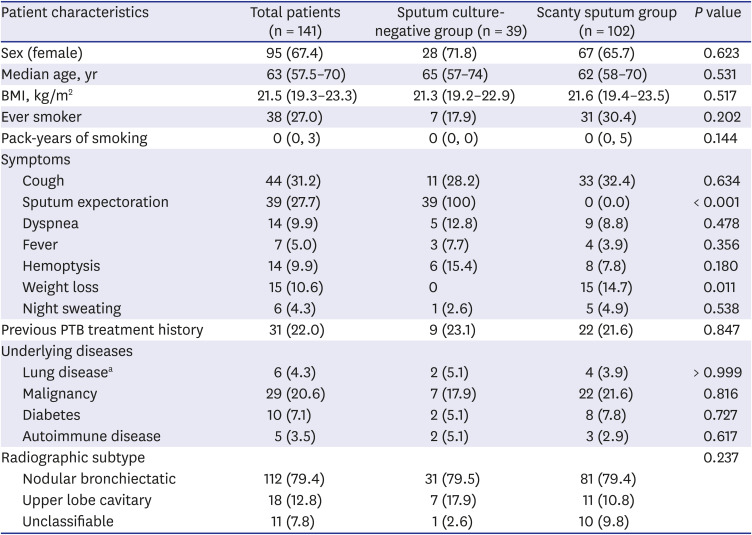
Table 1
Demographic and clinical characteristics of the 141 patients
Data are presented as number (%) or median (interquartile range).
PTB = pulmonary tuberculosis
aLung disease = 2 patients of Chronic obstructive pulmonary disease, 2 patients of idiopathic pulmonary fibrosis and 2 patients of bronchial asthma.
![]()
Bronchial washing diagnostic yield
Of the 141 patients, nontuberculous mycobacteria were cultured from bronchial washing specimens collected from 54 (38.3%) patients and M. tuberculosis was cultured from the specimens collected from 8 patients (5.7%). Furthermore, nontuberculous mycobacteria were cultured from bronchial washing specimens collected from 12 (30.7%) of the 39 patients in the sputum culture-negative group and 42 (41.2%) of the 102 patients in the scanty sputum group (P = 0.345). M. tuberculosis was cultured from the specimens collected from one patient (2.6%) in the sputum culture-negative group and seven patients (6.8%) in the scanty sputum group (P = 0.562) (Table 2).
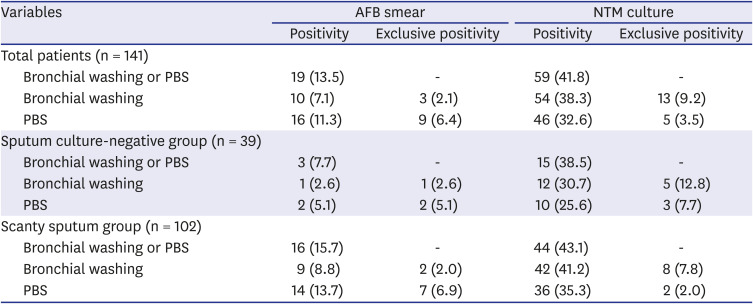
Table 2
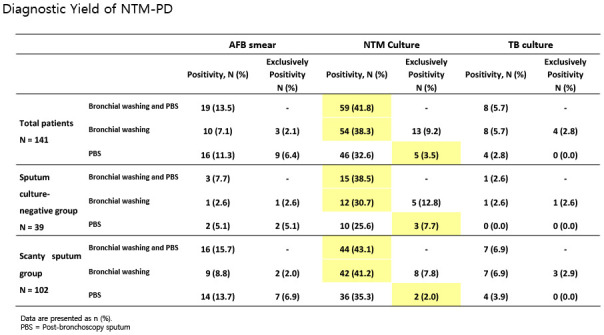
Yield of AFB smear and bronchial washing and PBS culture for the diagnosis of NTM pulmonary disease
Data are presented as number (%).
AFB = acid-fast bacilli, NTM = nontuberculous mycobacterial, PBS = post-bronchoscopy sputum.
![]()
PBS culture diagnostic yield
Of the 141 patients, nontuberculous mycobacteria were cultured from PBS collected from 46 patients (32.6%). Furthermore, nontuberculous mycobacteria were cultured from PBS collected from 10 (25.6%) of the 39 patients in the sputum culture-negative group and 36 (35.3%) of the 102 patients in the scanty sputum group (P = 0.327).
Among the 141 patients, nontuberculous mycobacteria were exclusively cultured from PBS collected from 5 (3.5%) patients: 3 (7.7%) of the 39 patients in the sputum culture-negative group and 2 (2.0%) of the 102 patients in the scanty sputum group (P = 0.255). Exclusively culture positive rates of PBS between patients with nodular bronchiectatic pattern and those with upper lobe cavitary type were not different. (3.6% vs. 5.6%, P = 0.531).
The combined yield of nontuberculous mycobacteria culture from bronchial washing and PBS specimens was 41.8% (59/141 patients): 38.5% (15/39 patients) in the sputum culture-negative group and 43.1% (44/102 patients) in the scanty sputum group (P = 0.755) (Table 2).
Nontuberculous mycobacteria species
The nontuberculous mycobacteria species identification results were available for 54 of the 59 patients with positive nontuberculous mycobacteria culture results. M. avium was the most common species in both groups; it was detected at rates of 17.9% (7/39) in the sputum culture-negative group and 17.6% (18/102) in the scanty sputum group. M. intracellulare was the second most common species in both groups. In one patient, a mixed infection by M. kansasii and M. abscessus subsp. massiliense was identified. There were no significant between-group differences in nontuberculous mycobacteria species distribution (Table 3).
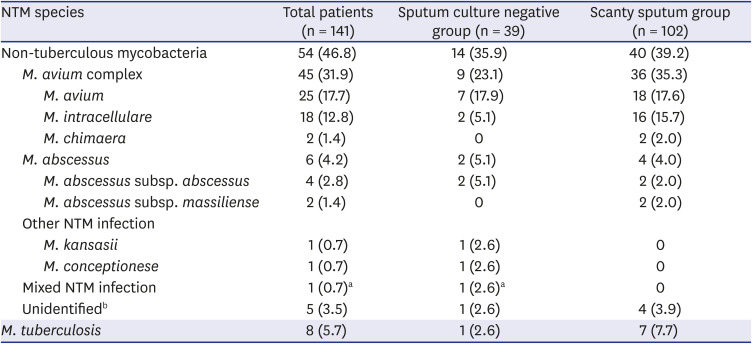
Table 3
Nontuberculous mycobacteria species isolated from bronchial washing or PBS
Data are presented as number (%).
PBS = post-bronchoscopy sputum, NTM = nontuberculous mycobacterial.
aOne case of mixed infection, M.kansasii and M. abscessus subsp. massiliense; b5 cases of not checked NTM-identification test.
![]()
Bronchoscopy-associated complications
Among the 141 patients, 5 experienced bronchoscopy-associated complications (fever in 3 patients, bloody sputum in 1 patient, and jaw dislocation in another patient). Patients' condition improved the same day.
Go to :
DISCUSSION
In this retrospective cohort study, we investigated the additional yield of PBS culture for the diagnosis of suspected NTM-PD in patients with consistently negative sputum nontuberculous mycobacteria culture or inadequate sputum production. In the 141 patients with suspected NTM-PD, bronchial washing specimen nontuberculous mycobacteria culture positivity was 38.3%, and the additional PBS collection improved this rate to 41.8%.
The role of bronchoscopy in the diagnosis of NTM-PD has been previously documented.12 In a retrospective study conducted in Japan, nontuberculous mycobacteria culture positivity of bronchoalveolar lavage was 93.7% in 16 patients with suspected NTM-PD with negative sputum smears or scanty sputum.18 Two other studies reported nontuberculous mycobacteria culture positivity rates of 50%8 and 54%19 for bronchoscopic specimens collected from patients with suspected NTM-PD and multiple nodules with bronchiectasis identified on chest CT. Although the culture positivity of bronchial washing specimen was lower (38.3%) in our study, the results confirmed the usefulness of bronchoscopy in patients with suspected NTM-PD. The lower nontuberculous mycobacteria culture positivity of bronchial washing in our study could be due to the different indications for bronchoscopy. In previous studies, bronchoscopy was adopted for patients with suspected NTM-PD with negative sputum smears or with typical NTM-PD CT findings81819; however, we performed bronchoscopy in patients with at least two negative sputum culture results or inadequate sputum production.
In patients with suspected pulmonary TB, the diagnostic yield of PBS has been reported.20 In one study, the PBS culture positivity was 75.4% and the rate of exclusively positive post-bronchoscopy nontuberculous mycobacteria culture was 7.0%10; in another study, these rates were 34% and 10%, respectively.13 Based on these data, the BTS guidelines recommend PBS collection among patients with suspected TB with scanty sputum production or consistently negative sputum AFB smears.14
PBS culture increased nontuberculous mycobacteria culture positivity from 30.7% to 38.5% in the sputum culture-negative group and from 41.2% to 43.1% in the scanty sputum group. These data suggest that additional PBS collection is useful among patients with suspected NTM-PD. Although the rate of exclusively positive culture for additional PBS was low, it is worthwhile to collect the additional specimen as minimal additional cost is incurred. In fact, a recent prospective study reported that additional bronchial brushing increased the NTM culture positivity by 4.3% than bronchial washing alone.21
Our study included patients with clinically and radiologically suspected NTM-PD; however, the final diagnosis was pulmonary TB rather than NTM-PD in 5.7% patients. It can be difficult to distinguish between NTM-PD and pulmonary TB based on clinical and radiological findings.2223 Moreover, we have previously reported that the accuracy of NTM-PD diagnosis based on chest CT findings is unsatisfactory.20 On the basis of these data, we suggest that clinicians should be aware of the possibility of pulmonary TB among patients originally suspected as having NTM-PD in South Korea, where the TB burden is intermediate.
For the correct interpretation of our results, we should acknowledge the limitations of our study. The study was performed in a single center, and the number of patients was limited. Elucidation of the predictors for PBS culture positivity through multivariable logistic regression was impossible due to weak statistical power.
In conclusion, we identified additional PBS collection can increase diagnostic yield marginally in patients with suspected NTM-PD who undergo bronchoscopy.
Go to :
 XML Download
XML Download