

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Hypothalamus-pituitary-adrenal (HPA) axis regulation is associated with stress adaptation.1 Stress-induced HPA axis activation may result in cortisol elevation. Excessive cortisol levels are responsible for hypertension, reduced immunity, metabolic changes and, death.2 Many factors can modify the HPA axis, such as smoking, nutrition, sleep, and disease. Drinking alcohol is one of the most important lifestyle factors affecting the HPA axis.
Recent studies of various aspects of the HPA axis have suggested a relationship between HPA axis function and alcohol use. Hospitalized patients with alcohol-use disorders have higher cortisol levels than patients without such disorders.3 In a population of climacteric women, alcohol was also positively correlated with cortisol levels.4 In addition to studies examining serum cortisol concentrations, studies of healthy males using overnight urinary cortisol gave similar results.5 However, some studies failed to find a significant relationship.67 Alcohol consumption is associated with many factors, such as sex, age, and chronic disease status,8 making it difficult to control all confounders in observational studies. Previous studies have adjusted for different confounders and some studies failed to show a relationship between alcohol consumption and serum cortisol levels. Therefore, there is some difficulty establishing a causal relationship between alcohol consumption and cortisol levels.
Mendelian randomization (MR) is widely used to avoid problems such as confounding effects and reverse causation, which prevents relationship estimation and assessment of the true causality among variables.910 Germline variants are randomly distributed in the general population with respect to phenotype.11 By using a variable that satisfies the three conditions in Table 1 as an instrumental variable (IV),12 a population can be divided into randomized subgroups with various phenotype levels. Therefore, MR using genetic variants as a proxy for risk factors of interest affects the random allocation in a randomized controlled study.13 These features make the results of the MR study more reliable than the observational study.14

Table 1
Three assumptions about instrumental variable available for Mendelian randomization studies
![]()
A functional single nucleotide polymorphism (SNP) of the aldehyde dehydrogenase 2 (ALDH2) gene, rs671, is common in East Asians and rare or absent in other ethnicities.15 Minor allele frequency of ALDH2 has strong ethnic heterogeneity; a previous study reported the minor allele frequency of ALDH2 as 17.4% in East Asians and 0% in South Asians, Americans, and Europeans.16 The genetic variant results in the inability to eliminate acetaldehyde. Consequently, after alcohol consumption, the blood acetaldehyde level is higher in AG heterozygotes and AA homozygotes than in GG homozygotes.1718 The accumulation of aldehyde due to the nonfunctional ALDH2 variants causes facial flushing, nausea, headache, etc., a syndrome called ‘Oriental flushing.’ These symptoms prevent people with ALDH2 variants from drinking heavily.19 Therefore, ALDH2 rs671 may be a good instrumental variable for showing the causal relationship between alcohol consumption and serum cortisol. Consequently, we performed MR analysis using ALDH2 rs671 to examine the causal relationship between alcohol and serum cortisol concentrations in Korean adults (Fig. 1).
 | Fig. 1Framework of MR analysis of this study. ALDH2 genotypes affects the amount of alcohol consumption. To determine the causal relationship between alcohol consumption and serum cortisol levels while avoiding the effect of potential confounder, MR analysis was conducted using the ALDH2 genotypes as an instrumental variable for alcohol consumption.MR = Mendelian randomization, ALDH2 = aldehyde dehydrogenase 2.
|
Go to : 
METHODS
Subjects
The subjects were from the Dong-gu Study, which was conducted in Dong District, Gwangju, Republic of Korea. The baseline survey was conducted from May 2007 to July 2010.20 Although there were 9,260 cohort participants, 338 were excluded because of missing values for the ALDH2 rs671 genotype, alcohol consumption, age, physical activity, smoking status, hypertension, diabetes, and education status. This analysis included the 8,922 participants with no missing values.
Covariates
All variables in the dataset were obtained from the Dong-gu Study. Age, physical activity, drinks per day, smoking history, hypertension, diabetes, and education status were surveyed using a questionnaire. Physical activity was defined as moderate physical activity performed for at least 30 minutes, five times a week, or high-intensity physical activity performed for at least 20 minutes, three times a week. Drinks per day were calculated using the number of drinking days per week and the number of standard drinks per drinking day. Smoking history was classified into never, former, and current smokers. Hypertension was defined as taking antihypertensive drugs or when the blood pressure was 140/90 mmHg or higher. Diabetes was defined as taking diabetic medication or when the plasma glucose level was 126 mg/dL or higher. Education was categorized into middle school or lower and high school or higher. Height and weight were measured in light clothing, without shoes, and body mass index (BMI) was calculated from the measured height and weight. Cortisol was measured with an immunoassay (ARCHITECT i2000; Abbott Laboratories, Abbott Park, IL, USA). The coefficient of variation for the total analytic precision of this assay was less than ≤ 10%. The lower detection limits of this assay were 0.4 g/dL.
Genotyping the ALDH2 rs671 polymorphism
Genomic DNA was extracted from peripheral blood with the QIAamp DNA Blood Mini Kit (QIAGEN, Valencia, CA, USA), following the manufacturer's protocol. rs671 was genotyped by high-resolution melting (HRM) analysis using a Rotor-Gene 6000 (Corbett Research, Sydney, Australia), as previously described.21 The polymerase chain reaction (PCR) primers (forward, 5′ TTGGTGGCTACAAGATGTCG 3′; reverse, 5′ CAGGTCCCACACTCACAGTTT 3′) produced a 97-bp amplicon. The reaction mixture for HRM contained 200 nM PCR primer, 1 µM SYTO 9 fluorescent dye (Invitrogen, Carlsbad, CA, USA), 0.5 U F-Star Taq polymerase (BioFACT), and 40 ng genomic DNA in 10 µL reaction volumes. The PCR started at 95°C for 5 minutes, followed by 40 cycles of 95°C for 5 seconds and 58°C for 30 seconds.
Statistical analysis
All analyses were performed separately for each sex because the sex difference of alcohol consumption is significant.22 The subjects' characteristics are shown as the mean ± standard deviation or number (%). One-way analysis of variance or χ2 tests were used to show the statistical significance of the difference in variables between each ALDH2 genotype. In the observational analysis, multivariate linear regression analysis was performed to evaluate the association between drinks per day and serum cortisol levels after adjusting for age, physical activity, smoking status, BMI, hypertension, diabetes, and education status. The two-stage least squares method of MR analysis was performed to evaluate the relationship between the predicted daily alcohol consumption by ALDH2 genotypes and blood cortisol concentration. In the first stage, genetically predicted daily drinking was calculated for the ALDH2 genotypes. In the second stage, serum cortisol level was predicted from the genetically predicted alcohol consumption after adjusting for age, physical activity, smoking status, BMI, hypertension, diabetes, and education status. All analyses were performed using R (ver. 4.0.0; R Foundation for Statistical Computing, Vienna, Austria).
Ethics statement
This study was approved by the Institutional Review Board (IRB) of Chonnam National University Hospital (IRB No. I-2008-05-056). Informed consent was obtained from each participant.
Go to :
RESULTS
Table 2 presents the baseline characteristics of the study population according to the ALDH2 rs671 genotypes in each sex. The mean daily drinks in men were 1.95, 0.39, and 0.12 for the GG, GA, and AA genotypes, respectively, and 0.14, 0.03, and < 0.01 in women. In both sexes, GG genotypes had the highest daily alcohol consumption. However, the difference of drinks per day between GG genotype and GA genotype was higher than between GA genotype and AA genotype. The pattern of cortisol levels according to genotypes varied by sex. The GA group had the lowest levels in men, and the AA group had the lowest levels in women, but the difference between groups was not significant in women. The difference of distribution of age between the genotypes are significant and the GA genotype group were older than other genotypes in both sexes. And BMI differed according to the rs671 polymorphism significantly in men.
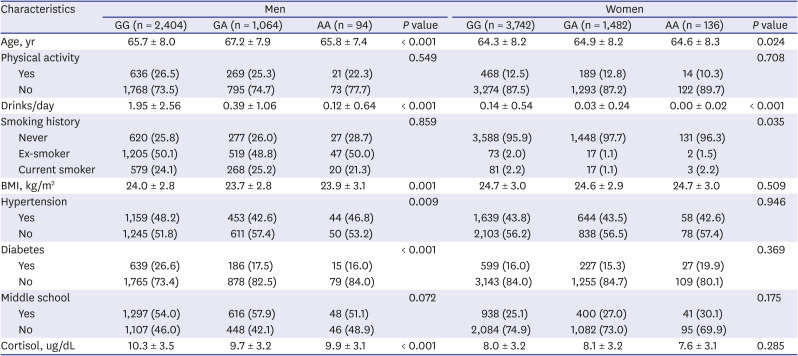
Table 2
Baseline characteristics of study population according to sex and ALDH2 rs671 genotypes
All values are presented as mean ± standard deviation or number (%). One-way analysis of variance and χ2 test are conducted in continuous and categorical variables respectively.
ALDH2 = aldehyde dehydrogenase 2, BMI = body mass index.
![]()
Table 3 presents the results of the univariate and multivariate linear regression models in each sex. Daily alcohol consumption was positively associated with blood cortisol levels in the univariate model in both sexes. After adjusting for age, physical activity, smoking status, hypertension, diabetes, and education status, the strength of the association between daily alcohol consumption and blood cortisol level was similar to the results of the univariate analysis in men but was higher in women.
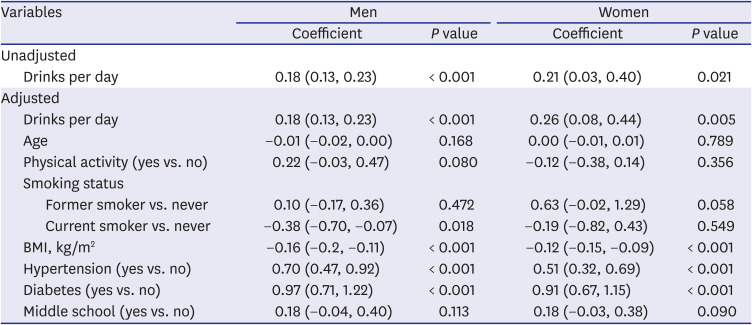
Table 3
Associations of alcohol (drinks per day) with cortisol (ug/dL) in observational study
All values were presented as regression coefficient (95% confidence interval). Age, physical activity, smoking status, BMI, hypertension, diabetes, education status were adjusted in adjusted linear regression models.
BMI = body mass index.
![]()
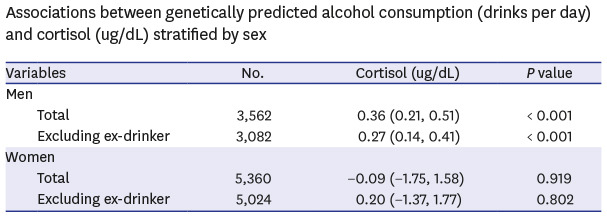
Table 4 shows the association between the genetically predicted alcohol consumption and blood cortisol level in each sex. The MR results except for ex-drinkers, are presented as a sensitivity analysis. In men, all models showed a positive association of genetically predicted daily alcohol consumption and blood cortisol level. In the MR analysis, the genetically predicted one standard drink/day increases cortisol by 0.36 (95% confidence interval [CI], 0.21–0.51). In sensitivity analysis genetically predicted one standard drink/day elevates cortisol by 0.27 (95% CI, 0.14–0.41). However, there was no significant association between alcohol and cortisol in all models for women.
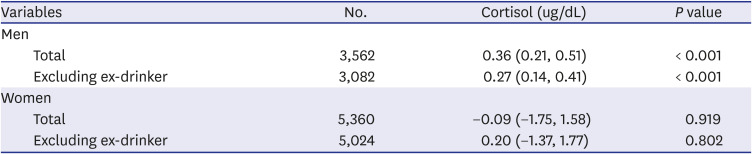
Table 4
Associations between genetically predicted alcohol consumption (drinks per day) and cortisol (ug/dL) stratified by sex
All values were presented as beta coefficient (95% confidence interval). Alcohol consumption was estimated through ALDH2 rs671 polymorphism and sex. All models were adjusted for age, physical activity, smoking, BMI hypertension, diabetes, and education status.
ALDH2 = aldehyde dehydrogenase 2, BMI = body mass index.
![]()
Go to :
DISCUSSION
This MR study examined the causal relationship between alcohol consumption and cortisol levels. In the observational analysis, alcohol consumption was associated with increased cortisol levels in both sexes. In the MR analysis, the genetically predicted alcohol consumption was associated with increased serum cortisol levels in men.
Several observational studies have examined the association between alcohol consumption and cortisol levels. In hospitalized patients, an alcohol use disorder group had higher cortisol levels than a non-alcoholic group.3 There was a positive correlation between alcohol consumption and the serum cortisol levels in climacteric women.4 In male workers at an airplane manufacturing plant in southern Germany, the group who consumed more than 20 g of alcohol per day had higher cortisol levels than those who did not.5 By contrast, in retail workers, alcohol consumption had no effects on the salivary cortisol concentration.7 In college students, binge drinkers had lower cortisol levels than the control group.6 This inconsistency may be due to the difference in how alcohol consumption was measured and the difference in the adjusted confounders in each study.
In this study, MR analysis in men showed a positive relationship between alcohol consumption and the serum cortisol level. The effect size of drinks per day on serum cortisol was greater in the MR analysis than in the observational analysis. This difference in effect size between the MR analysis and the observational analysis may be due to unknown confounding factors that affect the cortisol level and alcohol consumption. In the MR analysis of women, there was no significant association between genetically predicted alcohol consumption and the serum cortisol level. The sex difference may be due to the strength of the instrumental variable in each sex. In men, there was a difference of more than two drinks per day according to the ALDH2 rs671 genotypes, while in women the difference was lower than 0.2 drinks per day. Therefore, the rs671 polymorphism may be a weak instrumental variable for MR in women.23 The ‘weak instrument’ problem must be considered when interpreting the results. This problem occurs when the association of the instrumental variable and phenotype is not strong statistically.24 The generally used criterion for a weak instrument is an F statistic less than 10 in the regression model of phenotype on genotype.25 Although the F statistics was 207.5 in men and 32.79 in women, the satisfaction of criteria means that the study results are less biased below a certain level and does not mean that there is no bias.26 To assess potential bias, the sensitivity analysis was conducted of the population excluding ex-drinkers.27
It is not fully known how drinking affects the HPA axis in humans, but some biological explanations have been based on preclinical experiments. When an organism is exposed to stressful situations, the paraventricular nucleus (PVN) secretes corticotropin-releasing factor (CRF), which stimulates the anterior pituitary gland to release adrenocorticotropic hormone. Finally, cells in adrenal gland release glucocorticoids.28 Acute alcohol administration directly elevates PVN cellular activity, the onset of the stress hormone response in a rodent model,29 and in vitro.30 In an acute alcohol administration experimental study of healthy people, HPA axis activation occurs when the blood alcohol concentration is ≥ 0.1 µg/dL.3132 When this stressful-like situation due to alcohol ingestion has become chronic, the responsiveness of organs included in the stress hormone response changes. As a result, a blunted HPA axis response to stress challenge and upregulation of the central CRF pathway occur, suggesting elevated HPA axis hormone concentrations.283334 In an experimental study that investigated the interaction between acute alcohol administration and chronic alcohol use, short-term ethanol administration increased the cortisol level in the non-alcoholic population, but not in heavy drinkers or alcoholics.31 HPA axis responses are prominent when the blood alcohol concentration exceeds a certain level, although the threshold is influenced by chronic drinking, genetic factors, and so on. Some chronic drinkers develop the clinical features of Cushing's syndrome.35
There are some limitations to this study. First, the serum cortisol level changes with the circadian rhythm. In the observation study, the cortisol level had a nadir around midnight and peaked at around 8:30 am.3637 In this study, serum was obtained between 8:00 and 9:00 am, so the peak cortisol level was measured. Second, the alcohol intake may not have been measured accurately because alcohol consumption was measured using a standard glass and by roughly converting it according to beverage type.
In conclusion, the MR study showed that the genetically predicted alcohol consumption was positively associated with elevated serum cortisol levels in Korean men. This suggests a causal relationship between alcohol consumption and cortisol levels.
Go to :
 XML Download
XML Download