

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Breast cancer is considered one of the most common malignancies in women worldwide.1 Since 2002, cancer has been the leading cause of death in Korea,2 with breast cancer being the second most common cancer in women since 2004. The incidence of breast cancer in Korean women has increased steeply over the last decade, reaching up to 23.8% of all cancers affecting women in 2019.34
Breast reconstruction (BR) for mastectomy patients has more than just cosmetic benefits. Studies have demonstrated that women who undergo BR have a better quality of life compared with those who do not.56 Immediate BR (IBR), considered to be a widely accepted procedure, is used in an increasing number of breast cancer patients7 due to its aesthetic outcomes.89 In Korea, BR cases have increased significantly during the last 10 years.10 Previous research has shown that women with private insurance are much more likely to undergo IBR than the ones without private insurance.11
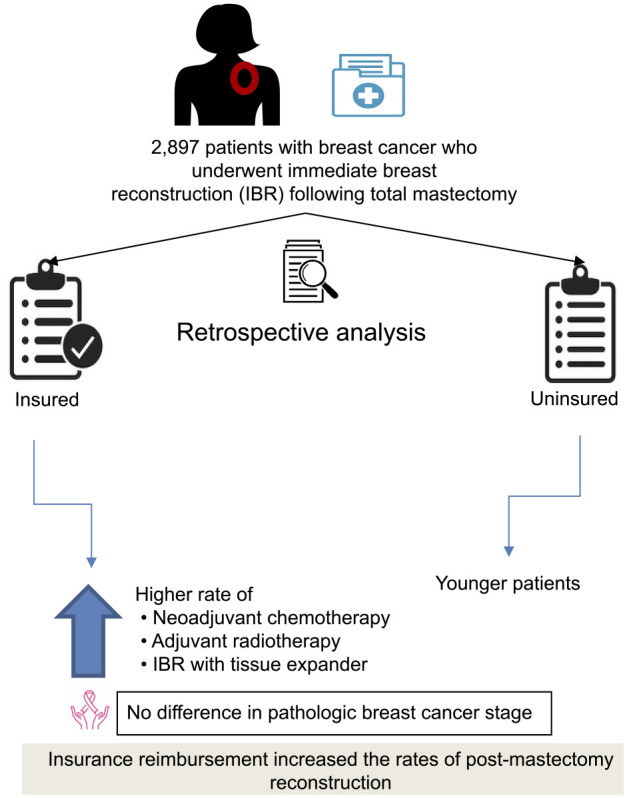
Since April 2015, the Korean National Health Insurance (NHI) has reimbursed breast cancer patients, approximately 50% of the cost of the BR procedure. This study aimed to evaluate how this policy change has affected the rates at which patients elect for IBR after total mastectomy for breast cancer.
Go to : 
METHODS
Study design
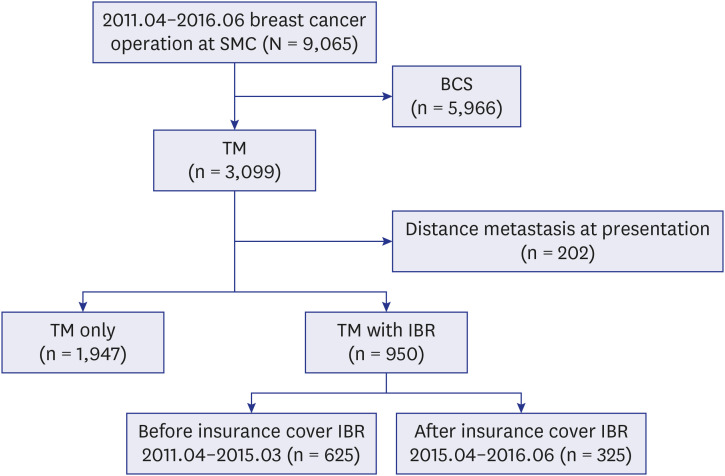
This single-centre retrospective study was conducted at the Samsung Medical Center in Korea. We reviewed the data of patients who underwent total mastectomy for primary breast cancer between April 2011 and June 2016. A total of 9,065 patients were operated for breast cancer. We excluded patients with breast conservative surgeries. A total of 3,099 patients had total mastectomy. We included 950 patients in the study who also underwent IBR and excluded 202 patients with distant metastases at presentation (Fig. 1). The patients were further classified as those that underwent IBR with either tissue expander insertion (TEI), deep inferior epigastric perforator flap (DIEP), or extended latissimus dorsi flap (ELD). The date when each mastectomy was performed and the patient's age at the time of surgery were collected, and age was categorized as < 35, 35–54, and ≥ 55 years. The patients were also classified according to whether their procedure was eligible for reimbursement before or after the April 2015 policy change in insurance coverage into “uninsured (before eligibility for NHI reimbursement)” and “insured (after eligibility for NHI reimbursement).” The primary outcome was the proportion of IBRs performed among the total mastectomy patients.
Tumor staging and mastectomy
Tumor stage, axillary lymph node metastasis, estrogen receptor (ER) status, progesterone receptor (PR) status, human epidermal growth factor-2 (HER-2) status, and the type of primary treatment (surgery or neoadjuvant chemotherapy [NACT]) were reviewed using the patients' electronic medical records. Pathologic staging followed the seventh edition of the American Joint Committee on Cancer (AJCC) classification. Total mastectomy and IBR were performed for all the patients by a team of breast and plastic surgeons, respectively, at our institution. The mastectomy performed was either a skin-sparing mastectomy (SSM) or a nipple-sparing mastectomy (NSM). SSM includes breast parenchyma resection with the nipple-areola complex (NAC); the skin above the tumor is resected, and the healthy breast skin is retained. NSM has the benefit of sparing the nipple-areolar skin. It is performed when no evidence of NAC invasion is found either clinically or on breast imaging studies, including breast magnetic resonance imaging. Breast tissue re-excision under the nipple is carried out to obtain an intraoperative frozen biopsy to rule out atypical cells or tumor involvement. In this study, the percentage of skin removal in the IBR group was comparable to or smaller than that in the mastectomy-only group.
Statistical analyses
Quantitative data are presented in a histogram and reported as medians with ranges and means with standard deviations. The association between patient characteristics was analyzed using χ2 test or Fisher's exact test. All P values were two-tailed, and a P value < 0.05 was considered statistically significant. All statistical analyses were carried out using SAS version 9.4 (SAS Institute, Cary, NC, USA) and R 3.0.3 (Vienna, Austria; http://www.R-project.org).
Ethics statement
This study adhered to the ethical tenets of the Declaration of Helsinki and was approved by the Institutional Review Board (IRB) of Samsung Medical Center in Seoul, Korea (IRB approval No. 2016-10-082). Since this study utilized a retrospective chart review data, the IRB waived the requirement for informed consent.
Go to :
RESULTS
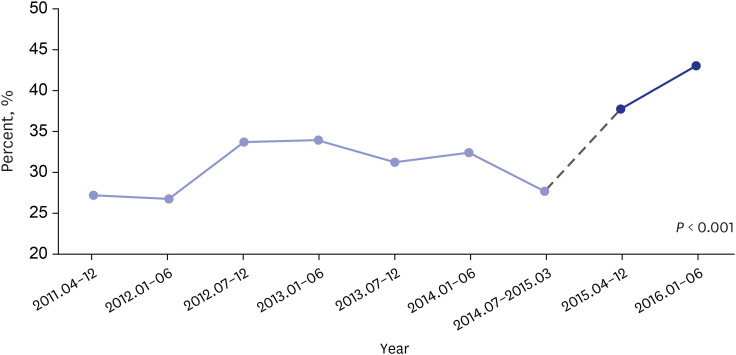
Table 1 displays the clinicopathological characteristics according to insurance reimbursement categories. Of the 2,897 women that underwent mastectomy between April 2011 and June 2016, 625 (30.1%) and 325 (40.4%) underwent IBR before (uninsured) and after (insured) NHI reimbursement eligibility (P < 0.001). Patients in the uninsured group tended to be younger compared with those in the insured group (median age [range], 43 [38–48] vs. 45 [40–50] years, respectively; P < 0.001).
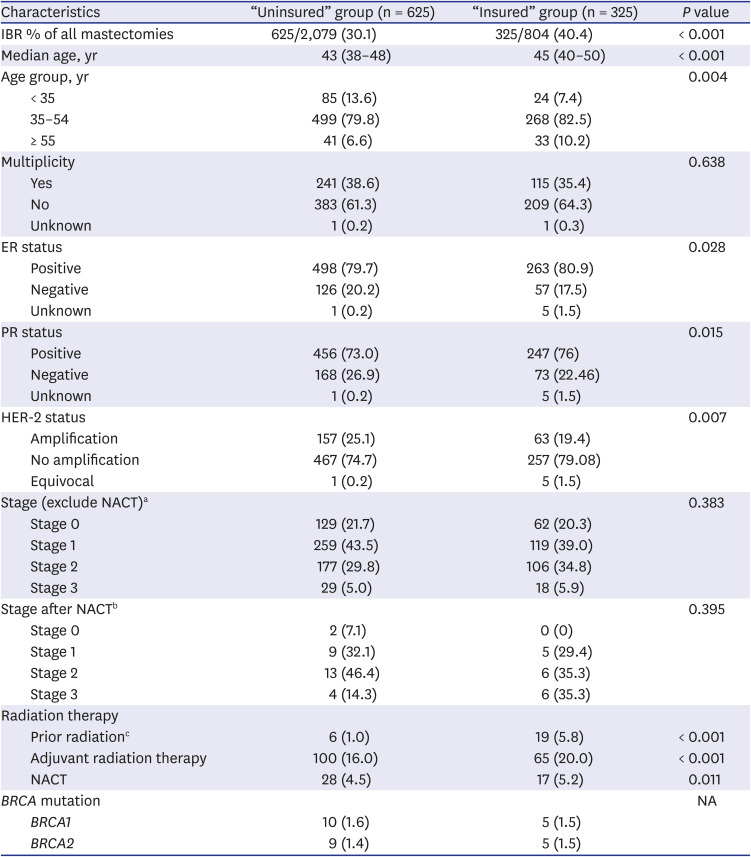
Table 1
Patient characteristics and trend by categorization according to insurance system policy change
Values are presented as median (interquartile range) or number (%).
IBR = immediate breast reconstruction, ER = estrogen receptor, PR = progesterone receptor, HER-2 = human epidermal growth factor receptor-2, NACT = neoadjuvant chemotherapy, NA = not applicable.
aStage (exclude NACT): “Uninsured” group (n = 595), “Insured” group (n = 305); bStage after NACT: “Uninsured” group (n = 30), “Insured” group (n = 20); cPatients with recurrence after adjuvant radiotherapy following breast-conserving surgery.
![]()
The pathologic stage did not differ significantly between the uninsured and insured groups. Most patients in both groups underwent surgery for AJCC stage I disease, followed by stage II, stage 0, and stage III, respectively. In the uninsured and insured groups, respectively, NACT was performed as the primary therapy in 28 (4.5%) and 17 (5.2%) patients (P = 0.011); adjuvant chemotherapy was administered to 265 (42.4%) and 146 (44.9%) patients (P = 0.681); and adjuvant radiation therapy was performed in 100 (16.0%) and 65 (20.0%) patients (P < 0.001). Compared to the uninsured group, more patients underwent IBR following mastectomy (for local recurrence after breast-conserving surgery) and radiotherapy (6 [1.0%] vs. 19 [5.8%], P < 0.001) or were ER/PR positive with HER-2 amplification (P = 0.028, P = 0.015, and P = 0.007) in the insured group. In the uninsured and insured groups, respectively, BRCA1 mutation was observed in 10 (1.6%) and 5 (1.5%) patients, while BRCA2 mutation was present in 9 (1.4%) and 5 (1.5%) patients. There were no significant differences between the two groups regarding their multiplicity or histopathological tumor type, although the invasive ductal carcinoma was the dominant breast cancer type in both groups.
The surgical treatment types are summarized in Table 2. Compared to the uninsured group, the insured group had significantly higher SSM rate (82.2% vs. 62.6%) and lower NSM rate (17.8% vs. 37.4; P < 0.001). Of the 623 patients in the uninsured group, 453 (72.5%) underwent IBR with TEI, 152 (24.3%) received DIEP, and 5 (0.8%) underwent ELD. Of the 325 patients in the insured group, 261 (80.3%) underwent IBR with TEI, and 63 (19.4%) underwent IBR with DIEP. In the uninsured vs. insured groups, 69.7% vs. 76.0% and 29.8% vs. 24.0% underwent sentinel lymph node biopsy and axillary lymph node dissection, respectively, with no significant differences between groups. Prophylactic contralateral mastectomy was performed in 8 (1.3%) and 8 (2.5%) patients in the uninsured and insured groups, respectively.
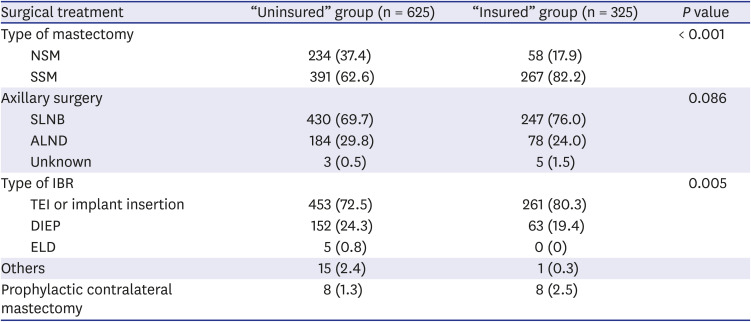
Table 2
Surgical treatment by categorization according to insurance system policy change
Values are presented as number (%).
NSM = nipple-sparing mastectomy, SSM = skin-sparing mastectomy, SLNB = sentinel lymph node biopsy, ALND = axillary lymph node dissection, IBR = immediate breast reconstruction, TEI = tissue expander insertion, DIEP = deep inferior epigastric perforator flap, ELD = extended latissimus dorsi flap.
![]()
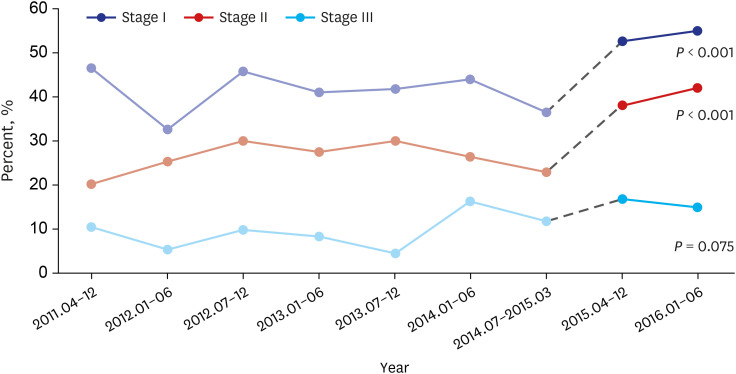
After the Korean NHI began reimbursing breast cancer patients for IBR, IBR rates increased by 10%, especially in patients with AJCC stages I and II breast cancer, which were statistically significant (P < 0.001) (Figs. 2 and 3). The relative increase in IBR rates was greatest among patients aged ≥ 35 years. More patients who underwent NACT and radiotherapy also received IBR.
Go to :
DISCUSSION
Mastectomy remains the primary treatment modality for breast cancer patients. Currently, the proportion of patients who prefer mastectomy to breast-conserving surgery has increased, and patients are also advised mastectomy to control local recurrence.1213 The peak incidence age for breast cancer of Asian women is much younger compared with that of Western women, and this has led to increased interest in IBR among Asian patients and their surgeons.10 Many studies have reported the oncologic safety of IBR for invasive breast cancer after curative surgery.14151617 Moreover, in advanced-stage disease or following NACT, most studies have found no increase in recurrence rates.181920 In terms of patient satisfaction, those who did not undergo IBR reported a significantly more distorted body image and sexuality compared with IBR patients.21 Furthermore, studies have demonstrated superior postoperative psychosocial benefits following IBR compared with those of delayed BR.212223 Consistent with these findings, Metcalfe et al.24 found that the prevalence of body dysmorphic disorder was significantly higher (34%) in a delayed BR group than in the IBR group (13%).
In the United States, the Women's Health and Cancer Rights Act, which was signed in October 1998, mandated the health insurance companies to cover BR costs. In the mid-1990s the rates of post-mastectomy reconstructions ranged 3–8%,25 while investigations in women diagnosed in the early 2000s revealed an increased rate of 25%.26 Hershman et al.11 reported that IBR rates following mastectomy for breast cancer remained low in women, for both invasive breast cancer (28%) and ductal carcinoma in situ (44%). Before 2010's, in Asian countries, BR rate never surpassed 18.0% among breast cancer patients.2728 Simultanously, in 2005, Son et al.29 reported that 12% of Korean breast cancer patients underwent IBR. However, after NHI reimbursement, in 2019, Song et al.30 reported that the IBR rate after total mastectomy increased from 19.4% in 2015 to 53.4% in 2018. In our patients, the rate of IBR among total mastectomy patients was 30% in uninsured patients and 39% in insured patients, with an increased IBR rate of 10%, especially in patients with AJCC stages I and II breast cancer. Furthermore, we demonstrated that the indication of IBR expanded to underwent NACT or underwent radiotherapy patients.
We found that NHI reimbursement had seemed to have had an impact on the rates of IBR. However, the dangers of excessive out-of-pocket economic burdens are extensively more for Korean patients than for patients with health insurance in the US; this may affect treatment choices and deter patients from undergoing IBR. For example, in patients with BRCA mutation, prophylactic contralateral prophylactic mastectomy (CPM) with IBR is not covered by Korean insurance. In our study population, BRCA mutation was present in approximately 1.5% of the patients. Of these, 42% and 80% underwent CPM with IBR before and after April 2015, respectively. The policy change in insurance coverage seemed to have had an impact in this population.
Our study also showed that IBR increased among patients aged ≥ 35 years after the insurance policy change. This result may be because patients diagnosed at a young age are less influenced (from the socio-economic perspective) and are likely to be more concerned with their appearance. Thus, the patients aged ≥ 35 years were more likely to be influenced by NHI coverage, which resulted in the increased rate of IBR. Interestingly, the proportion of patients undergoing NSM decreased in the insured group. Despite the expanded indications for NSM, it is still a controversial procedure in many situations, including close tumor-nipple distance, advanced breast cancer, and NACT. Furthermore, NSM is time-consuming, technically difficult, and requires a nipple-areolar complex frozen biopsy. Similarly, in the insured group, the proportion of patients undergoing TEI increased after the insurance policy change because DIEP is technically difficult and time-consuming.
Our study’s retrospective design was a limitation. We also did not evaluate the incidence of delayed BR. It is possible that patients who required postoperative radiation are more likely to choose delayed reconstruction, given the correlation between tumor stage and delayed reconstruction in patients. Historically, patients with advanced-stage tumors had low probability of undergoing BR, probably due to the anxiety of suspending chemotherapy or the undesired effects of post-mastectomy radiation. Additionally, our study lacked data regarding the effect of private insurance, which perhaps strongly influences post-mastectomy reconstruction. Nevertheless, this is the first report after the Korean NHI began providing 50% reimbursement cover for BR in breast cancer patients.
In conclusion, we noticed a significant increase in IBR rates after a change in the Korean insurance reimbursement policy. Future studies employing methods such as a nationwide survey are needed to determine the outcomes of health insurance coverage on IBR rates and on delayed reconstruction.
Go to :
 XML Download
XML Download