

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The prevalence of congenital anomalies in newborns in South Korea was 272.9 per 100,000 in 2005, and 314.7 per 100,000 in 2006.1 In other studies, the prevalence of congenital anomalies in South Korea was equivalent to 286.9 per 10,000 livebirths in 2006,2 while it was estimated 446.3 per 10,000 births during the period from 2008 to 2014.3 According to the 2010 Global Burden of Diseases, 510,400 deaths worldwide in 2010 were attributed to congenital anomalies. This equated to 1% of all deaths (6% of neonatal and postnatal infant deaths) and ranked 23rd as all causes of death.4 The European Surveillance of Congenital Anomalies (EUROCAT), a network of population-based registers of congenital anomalies in Europe covering 1.5 million births annually in 22 countries, reported a prevalence of congenital anomalies of 23.9 per 1,000 births during 2003–2007.5 Among them, 80% were livebirths, 17.6% underwent termination of pregnancy for fetal anomaly (TOPFA), and the remainder were stillbirths or died in the first week of birth. According to EUROCAT, during 2003–2007, while chromosomal anomalies accounted for 3.6 per 1,000 births, congenital heart defects (CHD) were the most common non-chromosomal anomalies (6.5 per 1,000 births), followed by limb defects (3.8 per 1,000 births), urinary system anomalies (3.1 per 1,000 births), and nervous system anomalies (2.3 per 1,000 births).5 In 11 EUROCAT countries, the average infant mortality with congenital anomalies was 1.1 per 1,000 births, and the average TOPFA prevalence was 4.6 per 1,000 births, which was more than 4 times the infant mortality related to congenital anomalies.4
Since prenatal medical intervention for the fetus is limited, and structural anomalies cannot be reversed during fetal development, primary prevention of congenital anomalies based on pre-conceptional care is critical at the population level. Identification of risk factors for congenital anomalies is fundamental for such primary prevention. To understand the causes of congenital anomalies, a more comprehensive literature review is required. A number of systematic reviews and meta-analyses have analyzed the association between environmental and genetic risk factors and various types of congenital anomalies; however, most articles have focused on a specific risk factor and a specific type of congenital anomaly. A few articles have covered risk factors in a comprehensive manner, but have focused on specific types of congenital anomalies, such as hip dysplasia67 or anorectal anomaly,8 while articles that comprehensively covered congenital anomalies focused on specific categories of risk factors, such as paternal risk factors,910 maternal smoking,11 secondhand smoking,12 maternal drug intake,1314 maternal influenza,15 or artificial reproductive technologies.1617 To the best of our knowledge, there has been no umbrella review of the available systematic reviews and meta-analyses regarding all reported non-genetic and genetic risk factors of all types of known congenital anomalies. The purpose of this article was to outline the spectrum of risk factors for congenital anomalies as comprehensively as possible, thereby providing not only a summary of currently available evidence, but also a suggestion for further study topics in the future.
Go to : 
METHODS
Databases and search strategy
We searched the PubMed, Google Scholar, Cochrane, and Embase databases up to July 1, 2019. Exposures included both environmental and genetic factors. The terms used in the searches were as follows: (“risk factors” [MeSH Terms] OR (“risk” [All Fields] AND “factors” [All Fields]) OR “risk factors” [All Fields] OR (“risk” [All Fields] AND “factor” [All Fields]) OR “risk factor” [All Fields]) AND (“congenital” [Subheading] OR “congenital” [All Fields]) AND (“meta-analysis” [Publication Type] OR “meta-analysis as topic” [MeSH Terms] OR “meta-analysis” [All Fields]).
We also manually searched the bibliography of identified papers for additional articles. The literature search, abstract screening, and full article review were independently performed by 2 researchers. Disagreements in the course of article searching were resolved by discussion until a consensus was reached.
Selection criteria
The following papers were selected: 1) systematic review and meta-analysis reports that analyzed the association between environmental or genetic risk factors and congenital anomalies, 2) papers written fully in English, and 3) papers that were peer-reviewed. Systematic reviews without meta-analyses were excluded. Studies published only as conference abstracts or case reports were also excluded.
Assessment of methodological quality
Two researchers independently assessed the methodological quality of the included studies according to AMSTAR2 (Assessing the Methodological Quality of Systematic Reviews, cohort and case control studies, but not case series).18 We used the tools included in the AMSTAR2 checklist (https://amstar.ca/Amstar_Checklist.php). Disagreement in the assessment was resolved by discussion until consensus was reached. For certainty of evidence, we used the Grading of Recommendations Assessment, Development and Evaluation (GRADE) system.18 Supplementary Table 1 shows the completed AMSTAR checklist based on the studies involved.
Data retrieval
Two researchers independently retrieved information from selected articles, including authors; year of study; risk factors; congenital anomalies as outcomes; the number of studies included in each meta-analysis; the database used for each systematic review; the date of database searching; the total number of study participants included in each study; the risk ratio (RR) or odds ratio (OR) and 95% confidence interval (CI); the methods of meta-analysis (fixed effects vs. random effects model); the methods used for assessing publication bias; and the method of assessment of methodological quality of studies included in each meta-analysis. Disagreement of the data retrieval between the 2 researchers was resolved through discussion.
Statistical analysis
We categorized 8 subgroups of congenital anomalies according to the 10th revision of the International Statistical Classification of Diseases (ICD-10). We estimated the summary of evidence on the significance of the effect size for the associations according to non-genetic risk factors and genetic risk factors. In addition, we evaluated the evidence of the studies showing significant effects by assessing the beta estimate, its 95% CI, and I2 ranges, P values for heterogeneity, and the number of meta-analyses included. We also plotted the range of ORs or RRs for associations between genetic risk factors or non-genetic risk factors and each subgroup of congenital anomalies.
Go to :
RESULTS
Description of eligible meta-analyses
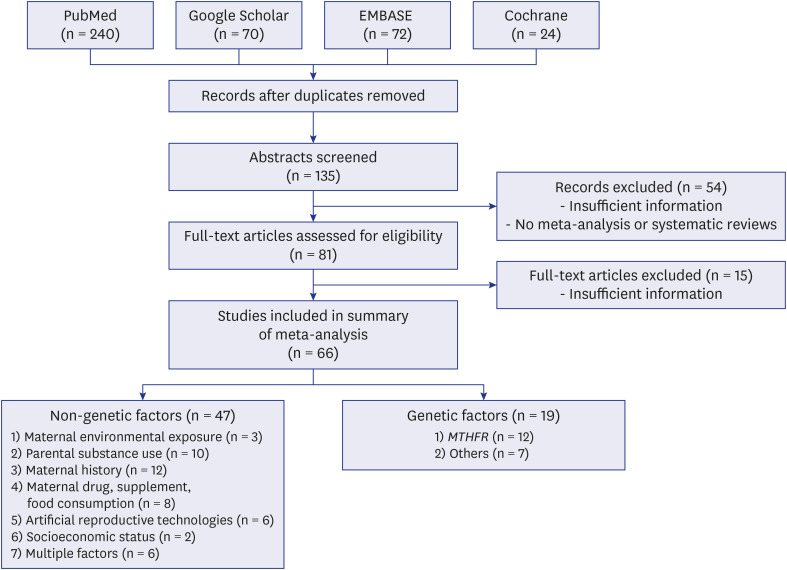
The detailed search procedures are summarized in Fig. 1. The search strategy identified 406 references. After excluding duplicated articles, we reviewed the titles and abstracts of all 135 identified studies, and further excluded 54 irrelevant studies. Then, the full texts of the remaining 81 articles were reviewed according to the inclusion and exclusion criteria. After examining these articles in more detail, further 15 studies were excluded due to irrelevance or insufficient data. Finally, 66 studies were included in the systematic review.
Non-genetic risk factors with evidence of association
Table 1 provides a summary of the association between non-genetic factors and congenital anomalies. We summarized the evidence of risk factors for congenital anomalies in the meta-analysis showing significant effects in Table 2 and Fig. 2, and describe the details below. We also listed the relevant studies and their characteristics in Supplementary Table 2.
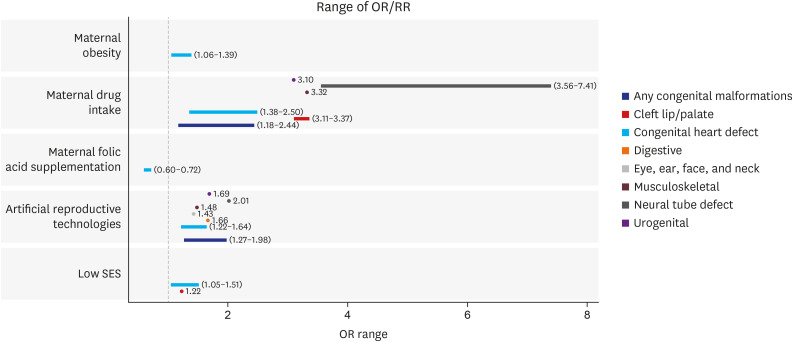 | Fig. 2The range of ORs or RRs in the association between non-genetic risk factor and congenital anomalies (significantly association only).OR = odds ratio, RR = risk ratio, SES = socioeconomic status.
|
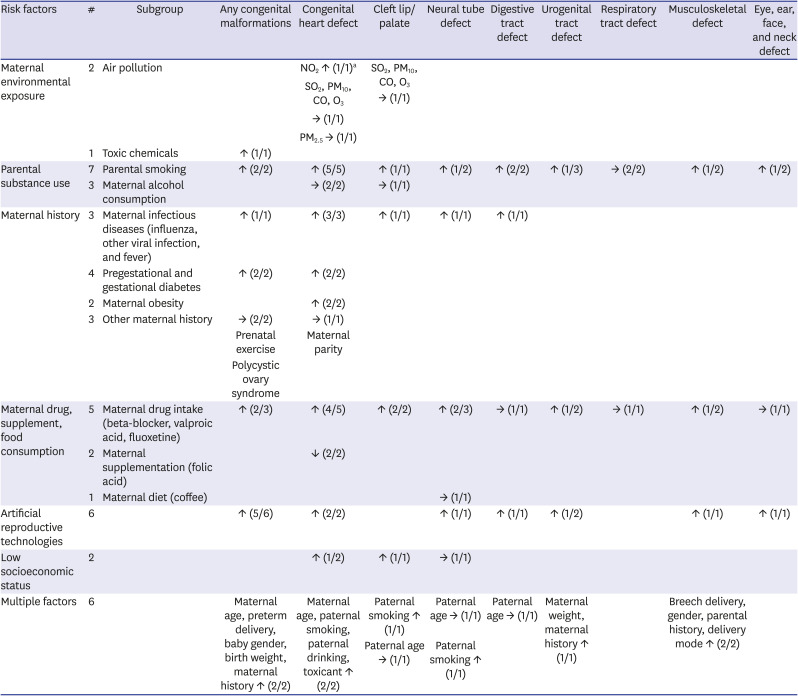
Table 1
The summary of evidence on significance with association between non-genetic risk factors for congenital diseases
↑ = positive pooled estimate association, → = no effect, ↓ = negative pooled estimate association, # = the numbers of meta-analysis studies.
a(numbers of meta-analyses studies with positive/negative/no effect pooled estimate/total numbers of meta-analysis).
![]()
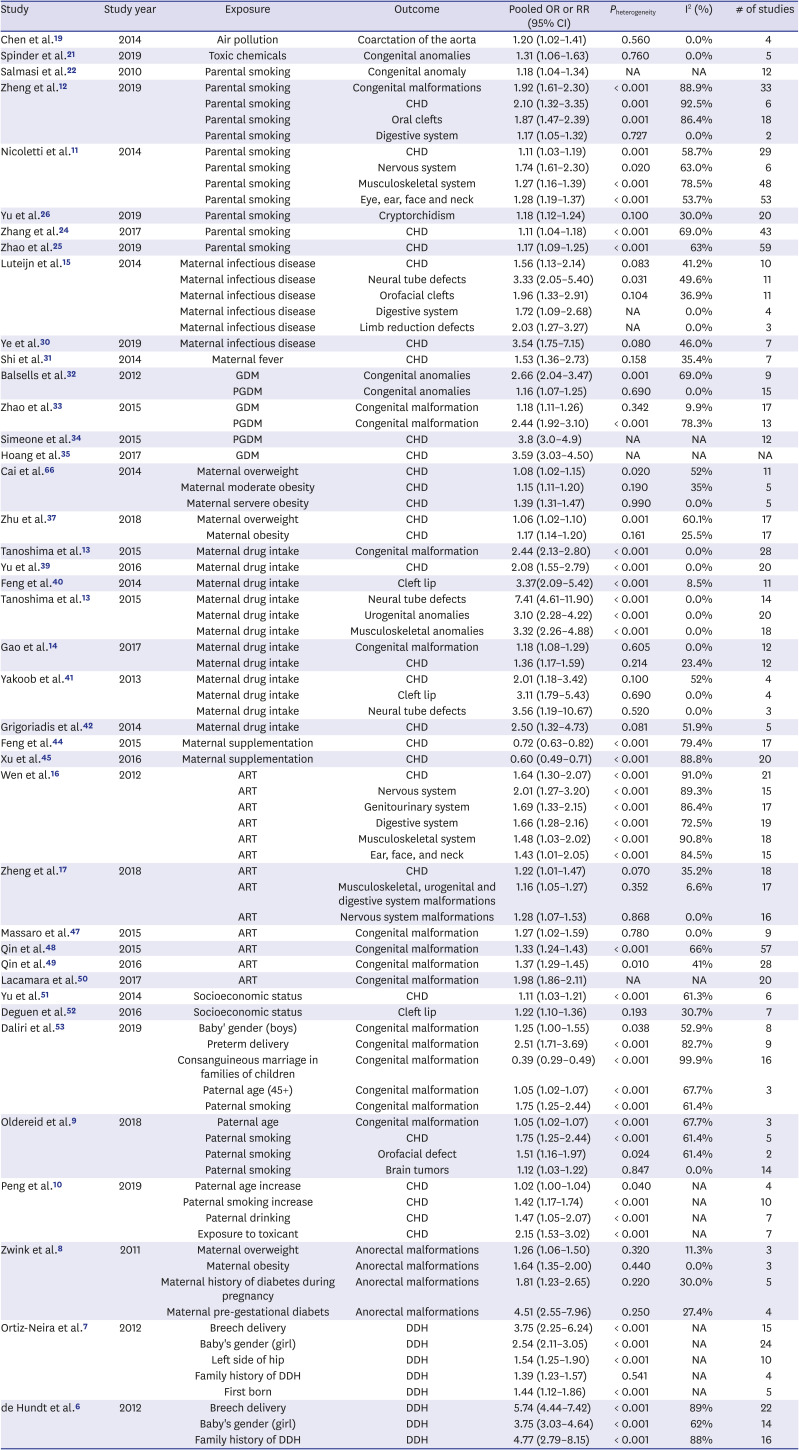
Table 2
Results of effectiveness of congenital anomalies in the significant studies of meta-analysis included for non-genetic risk factors
| Study | Study year | Exposure | Outcome | Pooled OR or RR (95% CI) | Pheterogeneity | I2 (%) | # of studies |
|---|---|---|---|---|---|---|---|
| Chen et al.19 | 2014 | Air pollution | Coarctation of the aorta | 1.20 (1.02–1.41) | 0.560 | 0.0% | 4 |
| Spinder et al.21 | 2019 | Toxic chemicals | Congenital anomalies | 1.31 (1.06–1.63) | 0.760 | 0.0% | 5 |
| Salmasi et al.22 | 2010 | Parental smoking | Congenital anomaly | 1.18 (1.04–1.34) | NA | NA | 12 |
| Zheng et al.12 | 2019 | Parental smoking | Congenital malformations | 1.92 (1.61–2.30) | < 0.001 | 88.9% | 33 |
| Parental smoking | CHD | 2.10 (1.32–3.35) | 0.001 | 92.5% | 6 | ||
| Parental smoking | Oral clefts | 1.87 (1.47–2.39) | 0.001 | 86.4% | 18 | ||
| Parental smoking | Digestive system | 1.17 (1.05–1.32) | 0.727 | 0.0% | 2 | ||
| Nicoletti et al.11 | 2014 | Parental smoking | CHD | 1.11 (1.03–1.19) | 0.001 | 58.7% | 29 |
| Parental smoking | Nervous system | 1.74 (1.61–2.30) | 0.020 | 63.0% | 6 | ||
| Parental smoking | Musculoskeletal system | 1.27 (1.16–1.39) | < 0.001 | 78.5% | 48 | ||
| Parental smoking | Eye, ear, face and neck | 1.28 (1.19–1.37) | < 0.001 | 53.7% | 53 | ||
| Yu et al.26 | 2019 | Parental smoking | Cryptorchidism | 1.18 (1.12–1.24) | 0.100 | 30.0% | 20 |
| Zhang et al.24 | 2017 | Parental smoking | CHD | 1.11 (1.04–1.18) | < 0.001 | 69.0% | 43 |
| Zhao et al.25 | 2019 | Parental smoking | CHD | 1.17 (1.09–1.25) | < 0.001 | 63% | 59 |
| Luteijn et al.15 | 2014 | Maternal infectious disease | CHD | 1.56 (1.13–2.14) | 0.083 | 41.2% | 10 |
| Maternal infectious disease | Neural tube defects | 3.33 (2.05–5.40) | 0.031 | 49.6% | 11 | ||
| Maternal infectious disease | Orofacial clefts | 1.96 (1.33–2.91) | 0.104 | 36.9% | 11 | ||
| Maternal infectious disease | Digestive system | 1.72 (1.09–2.68) | NA | 0.0% | 4 | ||
| Maternal infectious disease | Limb reduction defects | 2.03 (1.27–3.27) | NA | 0.0% | 3 | ||
| Ye et al.30 | 2019 | Maternal infectious disease | CHD | 3.54 (1.75–7.15) | 0.080 | 46.0% | 7 |
| Shi et al.31 | 2014 | Maternal fever | CHD | 1.53 (1.36–2.73) | 0.158 | 35.4% | 7 |
| Balsells et al.32 | 2012 | GDM | Congenital anomalies | 2.66 (2.04–3.47) | 0.001 | 69.0% | 9 |
| PGDM | Congenital anomalies | 1.16 (1.07–1.25) | 0.690 | 0.0% | 15 | ||
| Zhao et al.33 | 2015 | GDM | Congenital malformation | 1.18 (1.11–1.26) | 0.342 | 9.9% | 17 |
| PGDM | Congenital malformation | 2.44 (1.92–3.10) | < 0.001 | 78.3% | 13 | ||
| Simeone et al.34 | 2015 | PGDM | CHD | 3.8 (3.0–4.9) | NA | NA | 12 |
| Hoang et al.35 | 2017 | GDM | CHD | 3.59 (3.03–4.50) | NA | NA | NA |
| Cai et al.66 | 2014 | Maternal overweight | CHD | 1.08 (1.02–1.15) | 0.020 | 52% | 11 |
| Maternal moderate obesity | CHD | 1.15 (1.11–1.20) | 0.190 | 35% | 5 | ||
| Maternal servere obesity | CHD | 1.39 (1.31–1.47) | 0.990 | 0.0% | 5 | ||
| Zhu et al.37 | 2018 | Maternal overweight | CHD | 1.06 (1.02–1.10) | 0.001 | 60.1% | 17 |
| Maternal obesity | CHD | 1.17 (1.14–1.20) | 0.161 | 25.5% | 17 | ||
| Tanoshima et al.13 | 2015 | Maternal drug intake | Congenital malformation | 2.44 (2.13–2.80) | < 0.001 | 0.0% | 28 |
| Yu et al.39 | 2016 | Maternal drug intake | CHD | 2.08 (1.55–2.79) | < 0.001 | 0.0% | 20 |
| Feng et al.40 | 2014 | Maternal drug intake | Cleft lip | 3.37(2.09–5.42) | < 0.001 | 8.5% | 11 |
| Tanoshima et al.13 | 2015 | Maternal drug intake | Neural tube defects | 7.41 (4.61–11.90) | < 0.001 | 0.0% | 14 |
| Maternal drug intake | Urogenital anomalies | 3.10 (2.28–4.22) | < 0.001 | 0.0% | 20 | ||
| Maternal drug intake | Musculoskeletal anomalies | 3.32 (2.26–4.88) | < 0.001 | 0.0% | 18 | ||
| Gao et al.14 | 2017 | Maternal drug intake | Congenital malformation | 1.18 (1.08–1.29) | 0.605 | 0.0% | 12 |
| Maternal drug intake | CHD | 1.36 (1.17–1.59) | 0.214 | 23.4% | 12 | ||
| Yakoob et al.41 | 2013 | Maternal drug intake | CHD | 2.01 (1.18–3.42) | 0.100 | 52% | 4 |
| Maternal drug intake | Cleft lip | 3.11 (1.79–5.43) | 0.690 | 0.0% | 4 | ||
| Maternal drug intake | Neural tube defects | 3.56 (1.19–10.67) | 0.520 | 0.0% | 3 | ||
| Grigoriadis et al.42 | 2014 | Maternal drug intake | CHD | 2.50 (1.32–4.73) | 0.081 | 51.9% | 5 |
| Feng et al.44 | 2015 | Maternal supplementation | CHD | 0.72 (0.63–0.82) | < 0.001 | 79.4% | 17 |
| Xu et al.45 | 2016 | Maternal supplementation | CHD | 0.60 (0.49–0.71) | < 0.001 | 88.8% | 20 |
| Wen et al.16 | 2012 | ART | CHD | 1.64 (1.30–2.07) | < 0.001 | 91.0% | 21 |
| ART | Nervous system | 2.01 (1.27–3.20) | < 0.001 | 89.3% | 15 | ||
| ART | Genitourinary system | 1.69 (1.33–2.15) | < 0.001 | 86.4% | 17 | ||
| ART | Digestive system | 1.66 (1.28–2.16) | < 0.001 | 72.5% | 19 | ||
| ART | Musculoskeletal system | 1.48 (1.03–2.02) | < 0.001 | 90.8% | 18 | ||
| ART | Ear, face, and neck | 1.43 (1.01–2.05) | < 0.001 | 84.5% | 15 | ||
| Zheng et al.17 | 2018 | ART | CHD | 1.22 (1.01–1.47) | 0.070 | 35.2% | 18 |
| ART | Musculoskeletal, urogenital and digestive system malformations | 1.16 (1.05–1.27) | 0.352 | 6.6% | 17 | ||
| ART | Nervous system malformations | 1.28 (1.07–1.53) | 0.868 | 0.0% | 16 | ||
| Massaro et al.47 | 2015 | ART | Congenital malformation | 1.27 (1.02–1.59) | 0.780 | 0.0% | 9 |
| Qin et al.48 | 2015 | ART | Congenital malformation | 1.33 (1.24–1.43) | < 0.001 | 66% | 57 |
| Qin et al.49 | 2016 | ART | Congenital malformation | 1.37 (1.29–1.45) | 0.010 | 41% | 28 |
| Lacamara et al.50 | 2017 | ART | Congenital malformation | 1.98 (1.86–2.11) | NA | NA | 20 |
| Yu et al.51 | 2014 | Socioeconomic status | CHD | 1.11 (1.03–1.21) | < 0.001 | 61.3% | 6 |
| Deguen et al.52 | 2016 | Socioeconomic status | Cleft lip | 1.22 (1.10–1.36) | 0.193 | 30.7% | 7 |
| Daliri et al.53 | 2019 | Baby' gender (boys) | Congenital malformation | 1.25 (1.00–1.55) | 0.038 | 52.9% | 8 |
| Preterm delivery | Congenital malformation | 2.51 (1.71–3.69) | < 0.001 | 82.7% | 9 | ||
| Consanguineous marriage in families of children | Congenital malformation | 0.39 (0.29–0.49) | < 0.001 | 99.9% | 16 | ||
| Paternal age (45+) | Congenital malformation | 1.05 (1.02–1.07) | < 0.001 | 67.7% | 3 | ||
| Paternal smoking | Congenital malformation | 1.75 (1.25–2.44) | < 0.001 | 61.4% | |||
| Oldereid et al.9 | 2018 | Paternal age | Congenital malformation | 1.05 (1.02–1.07) | < 0.001 | 67.7% | 3 |
| Paternal smoking | CHD | 1.75 (1.25–2.44) | < 0.001 | 61.4% | 5 | ||
| Paternal smoking | Orofacial defect | 1.51 (1.16–1.97) | 0.024 | 61.4% | 2 | ||
| Paternal smoking | Brain tumors | 1.12 (1.03–1.22) | 0.847 | 0.0% | 14 | ||
| Peng et al.10 | 2019 | Paternal age increase | CHD | 1.02 (1.00–1.04) | 0.040 | NA | 4 |
| Paternal smoking increase | CHD | 1.42 (1.17–1.74) | < 0.001 | NA | 10 | ||
| Paternal drinking | CHD | 1.47 (1.05–2.07) | < 0.001 | NA | 7 | ||
| Exposure to toxicant | CHD | 2.15 (1.53–3.02) | < 0.001 | NA | 7 | ||
| Zwink et al.8 | 2011 | Maternal overweight | Anorectal malformations | 1.26 (1.06–1.50) | 0.320 | 11.3% | 3 |
| Maternal obesity | Anorectal malformations | 1.64 (1.35–2.00) | 0.440 | 0.0% | 3 | ||
| Maternal history of diabetes during pregnancy | Anorectal malformations | 1.81 (1.23–2.65) | 0.220 | 30.0% | 5 | ||
| Maternal pre-gestational diabets | Anorectal malformations | 4.51 (2.55–7.96) | 0.250 | 27.4% | 4 | ||
| Ortiz-Neira et al.7 | 2012 | Breech delivery | DDH | 3.75 (2.25–6.24) | < 0.001 | NA | 15 |
| Baby's gender (girl) | DDH | 2.54 (2.11–3.05) | < 0.001 | NA | 24 | ||
| Left side of hip | DDH | 1.54 (1.25–1.90) | < 0.001 | NA | 10 | ||
| Family history of DDH | DDH | 1.39 (1.23–1.57) | 0.541 | NA | 4 | ||
| First born | DDH | 1.44 (1.12–1.86) | < 0.001 | NA | 5 | ||
| de Hundt et al.6 | 2012 | Breech delivery | DDH | 5.74 (4.44–7.42) | < 0.001 | 89% | 22 |
| Baby's gender (girl) | DDH | 3.75 (3.03–4.64) | < 0.001 | 62% | 14 | ||
| Family history of DDH | DDH | 4.77 (2.79–8.15) | < 0.001 | 88% | 16 |
OR = odds ratio, RR = risk ratio, CI = confidence interval, ART = artificial reproductive technologies, CHD = congenital heart defect, DDH = developmental dysplasia of the hip, NA = not applicable, GDM = gestational diabetes mellitus, PGDM = pre-gestational diabetes mellitus.
![]()
Maternal environmental exposure
1) Air pollution
We identified 2 meta-analysis studies reporting the association between air pollution and congenital anomalies. Chen et al.19 showed that nitrate dioxide (NO2) concentration was significantly associated with coarctation of the aorta based on 2 case-control studies and 2 cohort studies (pooled OR, 1.20; 95% CI, 1.02–1.41 per 10 ppb). However, there was no evidence of an association of SO2, PM10, CO, and O3 with congenital anomalies. Hall and Robinson20 showed that there was no significant association between PM2.5 and congenital heart defects.
2) Toxic chemicals
We identified 1 systematic review that meta-analyzed the association between toxic chemicals and congenital anomalies. The study showed a positive association of toxic chemicals, such as solvents, pesticides, and heavy metals, with congenital anomalies, based on 5 case-control studies and 1 prospective cohort study (pooled OR, 1.31; 95% CI, 1.06–1.63).21
3) Parental substance use
① Parental smoking
We identified 7 systematic reviews and meta-analyses reporting an association between parental smoking exposure and congenital anomalies. Results from 2 studies suggested a positive association between parental smoking and the risk of any type of congenital anomalies. Salmasi et al.22 found that the overall estimate of the RR for congenital anomalies by fetal exposure to maternal smoking during pregnancy was 1.18, based on 12 studies (95% CI, 1.04–1.34). Zheng et al.12 found that fetal exposure to secondhand smoking was associated with an increased risk of congenital malformations in a meta-analysis of 33 case-control studies (pooled OR, 1.92; 95% CI, 1.61–2.30). The results of 4 of the remaining 5 meta-analyses included in our umbrella review suggested a positive association between parental smoking and the risk of CHD.1112232425 Zheng et al.12 showed a significant association between fetal exposure to secondhand smoking and various types of congenital anomalies, such as oral clefts, based on 18 case-control studies (pooled OR, 1.87; 95% CI, 1.47–2.39), and digestive system defects (pooled OR, 1.17; 95% CI, 1.05–1.32) in 2 case-control studies. Similarly, Nicoletti et al.12 showed that prenatal exposure to secondhand smoke resulted in a significantly increased risk of congenital anomalies, such as nervous system defects (pooled OR, 1.74; 95% CI, 1.61–2.30) in 6 case-control studies, musculoskeletal system defects (pooled OR, 1.27; 95% CI, 1.16–1.39) in 48 case-control studies, and eye, ear, face, and neck defects (pooled OR, 1.28; 95% CI, 1.19–1.37) in 53 case-control studies. Yu et al.26 reported that maternal smoking was positively associated with cryptorchidism, based on 5 cohort studies and 15 case-control studies (pooled OR, 1.18; 95% CI, 1.12–1.24).
② Maternal alcohol consumption.
We identified 3 meta-analyses reporting associations between maternal alcohol consumption and congenital anomalies. Sun et al.27 conducted meta-analyses of CHD and maternal alcohol consumption before and during pregnancy, using 23 case-control or cohort studies, and found no significant association between maternal alcohol consumption and congenital anomalies. Likewise, according to Wen et al.,28 who included 23 case-control or cohort studies in their meta-analysis, no statistically significant association was found between alcohol consumption and CHD. Bell et al.29 performed a meta-analysis (33 case-control or cohort studies) to evaluate the risk of orofacial clefts associated with maternal alcohol consumption, and found no statistically significant association.
Maternal history
1) Maternal infectious disease
We identified 3 meta-analyses analyzing the association between maternal infectious diseases and congenital anomalies, such as CHD, cleft lip/palate, neural tube defect, digestive tract defects, and hydrocephaly. Luteijn et al.15 reported an association between maternal influenza and congenital heart diseases from a meta-analysis of 4 case-control and 6 cohort studies (pooled OR, 1.56; 95% CI, 1.13–2.14). A study by Ye et al.30 supported this conclusion by showing the association between maternal viral infection, such as rubella virus and CHD, based on 7 case-control studies (pooled OR, 3.54; 95% CI, 1.75–7.15). The association between maternal infectious diseases and other congenital diseases was further reported; neural tube defects (pooled OR, 3.33; 95% CI, 2.05–5.40), orofacial clefts (pooled OR, 1.96; 95% CI, 1.33, 2.91), digestive system defects (pooled OR, 1.72; 95% CI, 1.09–2.68), and limb reduction defects (pooled OR, 2.03; 95% CI, 1.27–3.27).15 Shi et al.31 showed an association between maternal fever in the first trimester and CHD in a meta-analysis of 7 case-control studies (pooled OR, 1.53; 95% CI, 1.36–2.73).
2) Pre-gestational and gestational diabetes mellitus
We identified 4 systematic reviews and meta-analyses on pre-gestational and gestational diabetes mellitus (PGDM and GDM) as risk factors for congenital anomalies. Balsells et al.32 and Zhao et al.33 showed associations between maternal diabetes mellitus and congenital anomalies. They divided maternal diabetes into PGDM and GDM and found that GDM, based on 9 cohort studies (pooled RR, 2.66; 95% CI, 2.04–3.47), and PGDM, based on 15 cohort studies (pooled RR, 1.16; 95% CI, 1.07–1.25), were significantly associated with congenital anomalies. Zhao et al.33 also found significantly positive associations between GDM and congenital malformation, based on 17 cohort studies (pooled RR, 1.18; 95% CI, 1.11–1.26), and PGDM and congenital malformation, based on 13 cohort studies (pooled RR, 2.44; 95% CI, 1.92–3.10). Simeone et al.34 found a significantly positive association of PGDM and GDM with CHD (pooled OR, 3.8; 95% CI, 3.0–4.9). In addition, Hoang et al.35 reported an association between maternal diabetes and any type of CHD (pooled RR, 3.59; 95% CI, 3.03–4.50).
3) Maternal obesity
We identified 2 meta-analyses reporting the association between maternal obesity and CHD. Cai et al.36 found that maternal body mass index (BMI) was associated with CHD. A dose–response effect of maternal overweight (pooled OR, 1.08; 95% CI, 1.02–1.15), moderate obesity (pooled OR, 1.15; 95% CI, 1.11–1.20), and severe obesity (pooled OR, 1.39; 95% CI, 1.31–1.47) on the occurrence of CHD was found. Similarly, Zhu et al.37 demonstrated that CHD was associated with maternal BMI based on a meta-analysis of 17 case-control and cohort studies. Maternal overweight status (pooled OR, 1.06; 95% CI, 1.02–1.10) and obesity (pooled OR, 1.17; 95% CI, 1.14–1.20) significantly elevated the risk of CHD based on 13 case-control studies and 4 cohort studies. On the other hand, underweight maternal status was not associated with CHD.
4) Other maternal history
We identified 3 meta-analyses investigating the effect of other maternal histories and congenital anomalies. Davenport et al.38 showed that prenatal exercise did not increase the OR for congenital anomalies, based on 10 randomized controlled trial studies (pooled OR, 1.23; 95% CI, 0.77–1.95). Yu et al.39 found no significant association between maternal polycystic ovary syndrome and congenital anomalies, based on 6 cohort studies (pooled RR, 0.94; 95% CI, 0.36–2.42). Feng et al.40 showed that there was no evidence of association between maternal parity and the risk of CHD based on 14 case-control studies and 2 cohort studies (pooled OR, 1.01; 95% CI, 0.97–1.06).
Maternal drug, supplement, and food consumption
1) Maternal drug intake
We identified 5 meta-analyses reporting maternal drug intake associated with congenital anomalies. Results from 2 studies suggested a positive association between maternal drug intake and the risk of congenital anomalies. Based on 28 cohort studies, Tanoshima et al.13 found an association between valproic acid intake and congenital malformation (pooled RR, 2.44; 95% CI, 2.13–2.80), CHD (pooled RR, 2.08; 95% CI, 1.55–2.79), cleft lip (pooled RR, 3.37; 95% CI, 2.09–5.42), neural tube defects (pooled RR, 7.41; 95% CI, 4.61–11.90), urogenital anomalies (pooled RR, 3.10; 95% CI, 2.28–4.22), and musculoskeletal anomalies (pooled RR, 3.32; 95% CI, 2.26–4.88).13A positive association between exposure to fluoxetine and congenital malformation was shown in the study by Gao et al.,14 based on 12 cohort studies (pooled RR, 1.18; 95% CI, 1.08–1.29). In addition, fluoxetine was positively associated with CHD (pooled RR, 1.36; 95% CI, 1.17–1.59). However, urogenital anomalies, musculoskeletal anomalies, and nervous system defects were not significantly associated with fluoxetine.14 Yakoob et al.41 found no significant association between maternal intake of β-blockers and congenital anomalies overall. However, maternal β-blockers intake was significantly associated with subtypes of congenital anomalies, such as CHD (pooled OR, 2.01; 95% CI, 1.18–3.42), cleft lip (pooled OR, 3.11; 95% CI, 1.79–5.43), and neural tube defects (pooled OR, 3.56; 95% CI, 1.19–10.67).41 Grigoriadis et al.42 showed that CHD was associated with maternal antidepressant use (pooled OR, 2.50; 95% CI, 1.32–4.73). However, Wang et al.43 showed no significant association between selective serotonin reuptake inhibitors (SSRIs) and CHD.
2) Maternal supplementation
We identified 2 meta-analyses reporting the association between maternal supplementation and congenital anomalies. Feng et al.44 reported a significantly negative association between folic acid supplementation and CHD, based on a meta-analysis based on 1 randomized controlled trial, 1 cohort study, and 16 case-control studies (pooled RR, 0.72; 95% CI, 0.63–0.82). Xu et al.45 also reported a meta-analysis showing a negative association of maternal folic acid supplementation and CHD, which was based on 20 case-control studies (pooled OR, 0.60; 95% CI, 0.49–0.71).
3) Maternal diet
We identified 1 meta-analysis reporting the association between maternal diet and congenital anomalies. Li et al.46 showed that no significant association was found between maternal coffee consumption and neural tube defects.
Artificial reproductive technologies
We identified 6 meta-analyses reporting the association between artificial reproductive technologies (ART) and congenital anomalies. Two of these showed a positive relationship between ART and CHD. Wen et al.16 reported a pooled OR of 1.64 (95% CI, 1.30–2.07), while Zheng et al.17 reported a pooled RR of 1.22 (95% CI, 1.01–1.47). In addition, Wen et al.16 reported associations of ART and nervous system (pooled OR, 2.01; 95% CI, 1.27–3.20); genitourinary system (pooled OR, 1.69; 95% CI, 1.33–2.15); digestive system (pooled OR, 1.66; 95% CI, 1.28–2.16); musculoskeletal system (pooled OR, 1.48; 95% CI, 1.03–2.02); and ear, face, and neck (pooled OR, 1.43; 95% CI, 1.01–2.05) anomalies. Zheng et al.17 showed an association between ART and various congenital anomalies. Massaro et al.47 and Qin et al.48 published 2 papers about the positive association between ART and congenital malformation (pooled RR, 1.33; 95% CI, 1.24–1.43 and pooled RR, 1.37; 95% CI, 1.29–1.45). Several studies have shown a weak relationship between in vitro fertilization (IVF)/intra-cytoplasmic sperm injection (ICSI) and several types of congenital malformations.17 Zheng et al.17 reported a significant association between the risk of musculoskeletal, urogenital, and digestive system malformations based on 17 cohort studies (pooled RR, 1.16; 95% CI, 1.05–1.27); risk of nervous system malformations based on 16 cohort studies (pooled RR, 1.28; 95% CI, 1.07–1.53). However, Zheng et al.17 did not find evidence of association between IVF/ICSI and risk of congenital anomalies such as cleft lip and/or palate; eye, ear, face, and neck; and respiratory system malformation. Massaro et al.47 showed a positive association between congenital malformation and ICSI as opposed to IVF (pooled OR, 1.27; 95% CI, 1.02–1.59).49 Lacamara et al.50 also showed a positive association between ICSI and congenital malformation, based on 5 cross-sectional studies and 15 cohort studies (pooled OR, 1.98; 95% CI, 1.86–2.11).
Socioeconomic status
We identified 2 meta-analyses reporting on socioeconomic status (SES) and congenital anomalies. Yu et al.51 reported that SES indices, including maternal educational attainment, family income, and maternal occupation, were negatively associated with an increased risk of CHD (pooled RR [95% CIs] ranging from 1.05 [1.01–1.09] to 1.51 [1.02–2.24]). Deguen et al.52 showed a significant association between low neighborhood SES and cleft palate, compared to high SES and found a significantly higher cleft lip rate in deprived neighborhoods, based on 6 case-control studies and 1 ecological study (pooled OR, 1.22; 95% CI, 1.10–1.36). However, no significant difference was observed according to SES in terms of neural tube defects and CHD.52
Multiple factors
We identified 6 meta-analyses reporting on the role of multiple factors and congenital anomalies. Results from 2 studies suggested a strong positive association between multiple factors and the risk of any congenital anomalies. Daliri et al.53 found that congenital malformation was associated with multiple risk factors, such as the baby's sex (boys), preterm delivery, consanguineous marriage in the families of the children, paternal age (> 45 years), and paternal smoking. Oldereid et al.9 found that the overall estimate of the OR for paternal age (> 45 years) and birth defects was 1.05 (95% CI, 1.02–1.07). They showed an association between exposure to multiple factors, such as paternal age > 45 years (pooled OR, 1.03; 95% CI, 0.99–1.06) and paternal smoking (pooled OR, 1.75; 95% CI, 1.25–2.44), and CHD. In addition, they found positive associations between paternal smoking and 2 types of congenital anomalies, i.e., orofacial defect (pooled OR, 1.51; 95% CI, 1.16–1.97) and brain tumors (pooled OR, 1.12; 95% CI, 1.03–1.22). However, they found no significant association between paternal age (> 45 years) and 3 types of congenital anomalies, such as spinal bifida, orofacial defects, and gastroschisis, compared to a younger paternal age. Peng et al.10 found a positive association between multiple factors and CHD and reported that increased paternal age, paternal smoking, paternal drinking, and exposure to toxicants were associated with the occurrence of CHD. Zwink et al.8 found positive associations between parental risk factors, such as maternal overweight, maternal obesity, maternal history of diabetes during pregnancy, and anorectal malformations. Results from 2 studies suggested a strong positive association between multiple factors and the risk of musculoskeletal anomalies. De Hundt et al.6 and Ortiz-Neira et al.7 reported the overall estimates of developmental dysplasia of the hip (DDH) upon exposure to multiple factors, such as breech delivery, baby's sex (girl), family history of DDH, mode of delivery, and first birth.
Genetic risk factors with evidence of association
Table 3 provides a summary of the association between genetic factors and congenital anomalies. We summarized the evidence for these associations in the included meta-analyses in Table 4 and Fig. 3. More detailed results about the association between each factor and congenital anomaly are described below.
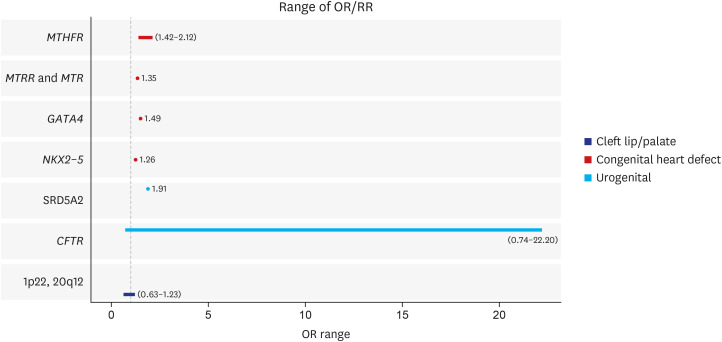 | Fig. 3The range of ORs or RRs in the association between non-environmental risk factor and congenital anomalies (significantly association only).OR = odds ratio, RR = risk ratio, MTHFR = methylene tetrahydrofolate reductase, MTRR = methionine synthase reductase gene, MTR = methionine synthase, GATA4 = GATA binding protein 4, NKX2-5 = NK2 homeobox 5, SRD5A2 = steroid 5 alpha-reductase type 2 gene, CFTR = cystic fibrosis transmembrane conductance regulator.
|
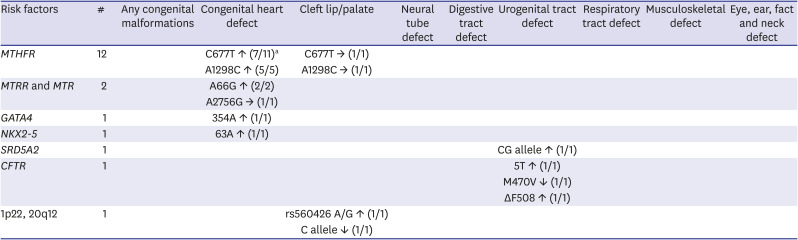
Table 3
The summary of evidence on significance with association between genetic risk factors for congenital diseases
MTHFR = methylene tetrahydrofolate reductase, MTRR = methionine synthase reductase gene, MTR = methionine synthase, GATA4 = GATA binding protein 4, NKX2-5 = NK2 homeobox 5, SRD5A2 = steroid 5 alpha-reductase type 2 gene, CFTR = cystic fibrosis transmembrane conductance regulator, ↑ = positive pooled estimate association, → = no effect, ↓ = negative pooled estimate association, # = the numbers of meta-analysis studies.
a(numbers of significant pooled estimate/total numbers of meta-analysis).
![]()
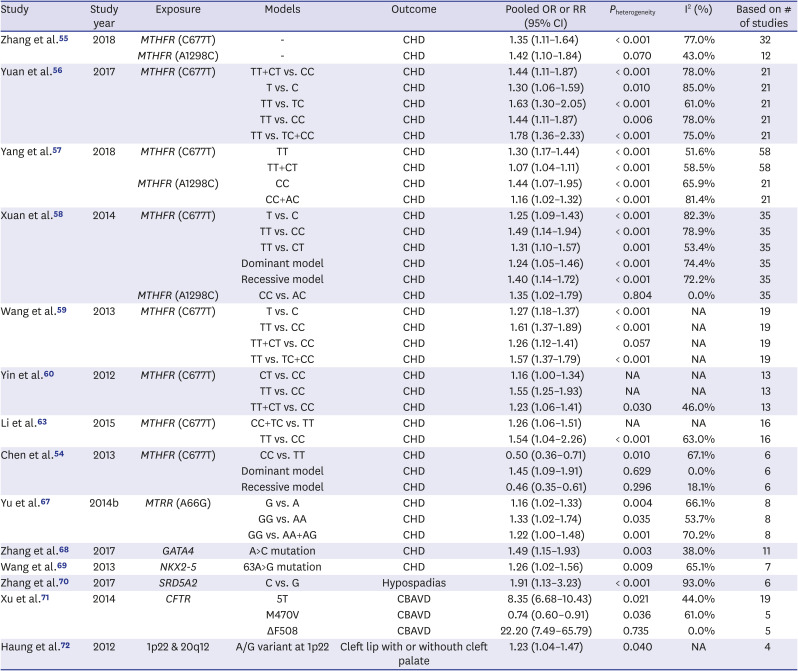
Table 4
Results of effectiveness of congenital anomalies in the significant studies of meta-analysis included for genetic risk factors
| Study | Study year | Exposure | Models | Outcome | Pooled OR or RR (95% CI) | Pheterogeneity | I2 (%) | Based on # of studies |
|---|---|---|---|---|---|---|---|---|
| Zhang et al.55 | 2018 | MTHFR (C677T) | - | CHD | 1.35 (1.11–1.64) | < 0.001 | 77.0% | 32 |
| MTHFR (A1298C) | - | CHD | 1.42 (1.10–1.84) | 0.070 | 43.0% | 12 | ||
| Yuan et al.56 | 2017 | MTHFR (C677T) | TT+CT vs. CC | CHD | 1.44 (1.11–1.87) | < 0.001 | 78.0% | 21 |
| T vs. C | CHD | 1.30 (1.06–1.59) | 0.010 | 85.0% | 21 | |||
| TT vs. TC | CHD | 1.63 (1.30–2.05) | < 0.001 | 61.0% | 21 | |||
| TT vs. CC | CHD | 1.44 (1.11–1.87) | 0.006 | 78.0% | 21 | |||
| TT vs. TC+CC | CHD | 1.78 (1.36–2.33) | < 0.001 | 75.0% | 21 | |||
| Yang et al.57 | 2018 | MTHFR (C677T) | TT | CHD | 1.30 (1.17–1.44) | < 0.001 | 51.6% | 58 |
| TT+CT | CHD | 1.07 (1.04–1.11) | < 0.001 | 58.5% | 58 | |||
| MTHFR (A1298C) | CC | CHD | 1.44 (1.07–1.95) | < 0.001 | 65.9% | 21 | ||
| CC+AC | CHD | 1.16 (1.02–1.32) | < 0.001 | 81.4% | 21 | |||
| Xuan et al.58 | 2014 | MTHFR (C677T) | T vs. C | CHD | 1.25 (1.09–1.43) | < 0.001 | 82.3% | 35 |
| TT vs. CC | CHD | 1.49 (1.14–1.94) | < 0.001 | 78.9% | 35 | |||
| TT vs. CT | CHD | 1.31 (1.10–1.57) | 0.001 | 53.4% | 35 | |||
| Dominant model | CHD | 1.24 (1.05–1.46) | < 0.001 | 74.4% | 35 | |||
| Recessive model | CHD | 1.40 (1.14–1.72) | < 0.001 | 72.2% | 35 | |||
| MTHFR (A1298C) | CC vs. AC | CHD | 1.35 (1.02–1.79) | 0.804 | 0.0% | 35 | ||
| Wang et al.59 | 2013 | MTHFR (C677T) | T vs. C | CHD | 1.27 (1.18–1.37) | < 0.001 | NA | 19 |
| TT vs. CC | CHD | 1.61 (1.37–1.89) | < 0.001 | NA | 19 | |||
| TT+CT vs. CC | CHD | 1.26 (1.12–1.41) | 0.057 | NA | 19 | |||
| TT vs. TC+CC | CHD | 1.57 (1.37–1.79) | < 0.001 | NA | 19 | |||
| Yin et al.60 | 2012 | MTHFR (C677T) | CT vs. CC | CHD | 1.16 (1.00–1.34) | NA | NA | 13 |
| TT vs. CC | CHD | 1.55 (1.25–1.93) | NA | NA | 13 | |||
| TT+CT vs. CC | CHD | 1.23 (1.06–1.41) | 0.030 | 46.0% | 13 | |||
| Li et al.63 | 2015 | MTHFR (C677T) | CC+TC vs. TT | CHD | 1.26 (1.06–1.51) | NA | NA | 16 |
| TT vs. CC | CHD | 1.54 (1.04–2.26) | < 0.001 | 63.0% | 16 | |||
| Chen et al.54 | 2013 | MTHFR (C677T) | CC vs. TT | CHD | 0.50 (0.36–0.71) | 0.010 | 67.1% | 6 |
| Dominant model | CHD | 1.45 (1.09–1.91) | 0.629 | 0.0% | 6 | |||
| Recessive model | CHD | 0.46 (0.35–0.61) | 0.296 | 18.1% | 6 | |||
| Yu et al.67 | 2014b | MTRR (A66G) | G vs. A | CHD | 1.16 (1.02–1.33) | 0.004 | 66.1% | 8 |
| GG vs. AA | CHD | 1.33 (1.02–1.74) | 0.035 | 53.7% | 8 | |||
| GG vs. AA+AG | CHD | 1.22 (1.00–1.48) | 0.001 | 70.2% | 8 | |||
| Zhang et al.68 | 2017 | GATA4 | A>C mutation | CHD | 1.49 (1.15–1.93) | 0.003 | 38.0% | 11 |
| Wang et al.69 | 2013 | NKX2-5 | 63A>G mutation | CHD | 1.26 (1.02–1.56) | 0.009 | 65.1% | 7 |
| Zhang et al.70 | 2017 | SRD5A2 | C vs. G | Hypospadias | 1.91 (1.13–3.23) | < 0.001 | 93.0% | 6 |
| Xu et al.71 | 2014 | CFTR | 5T | CBAVD | 8.35 (6.68–10.43) | 0.021 | 44.0% | 19 |
| M470V | CBAVD | 0.74 (0.60–0.91) | 0.036 | 61.0% | 5 | |||
| ΔF508 | CBAVD | 22.20 (7.49–65.79) | 0.735 | 0.0% | 5 | |||
| Haung et al.72 | 2012 | 1p22 & 20q12 | A/G variant at 1p22 | Cleft lip with or withouth cleft palate | 1.23 (1.04–1.47) | 0.040 | NA | 4 |
OR = odds ratio, RR = risk ratio, CI = confidence interval, MTHFR = methylene tetrahydrofolate reductase, MTRR = methionine synthase reductase gene, MTR = methionine synthase, GATA4 = GATA binding protein 4, NKX2-5 = NK2 homeobox 5, SRD5A2 = steroid 5 alpha-reductase type 2 gene, CFTR = cystic fibrosis transmembrane conductance regulator, CHD = congenital heart defect, CBAVD = congenital bilateral absence of vas deferens.
![]()
MTHFR
In MTHFR, which encodes methylenetetrahydrofolate reductase, 2 polymorphisms, C677T and A1298C, have been investigated. Eleven meta-analyses have investigated the association of congenital diseases with C677T,5455565758596061626364 All meta-analyses analyzed the risk of CHD and only 1 study examined both congenital heart disease and orofacial cleft. Three studies showed no significant association between C677T and congenital heart disease, while 7 studies described a positive association with these conditions. In particular, the largest odds ratio was found in the study by Yuan et al.,56 which reported a significant positive effect in a homozygote model based on 21 case-control studies. However, Chen et al.54 reported 2 negative ORs, for the recessive model and for the homozygote model, each based on 6 case-control studies. Yang et al.57 conducted a meta-analysis using 42 studies; both MTHFR C677T and A1298C polymorphisms were associated with the risk of CHD.56 A TT model (pooled RR, 1.30; 95% CI, 1.14–1.48) and a TT+CT model (pooled RR, 1.09; 95% CI, 1.04–1.14) showed a significant positive relationship with congenital heart disease. Only 1 study found a statistically non-significant association between orofacial cleft and C677T in mothers, based on 8 case-control studies.64 Five studies have identified associations with the A1298C polymorphism.5556576465 All 5 studies considered congenital heart disease, while only Verkleij-Hagoort et al.64 further analyzed orofacial cleft. Moreover, all 5 studies showed an increasing effect of A1298C on CHD. The largest OR was reported by Zhang et al.55 based on 11 case-control studies (pooled OR, 1.42; 95% CI, 1.10–1.84). On the other hand, A1298C in mothers and children did not have a significant effect on orofacial cleft.64 Additionally, Yang et al.57 also reported A1298C effects on congenital heart disease using RR. They found that the CC (pooled RR, 1.44; 95% CI, 1.07–1.95) and CC+AC genotype groups (pooled RR, 1.16; 95% CI, 1.02–1.31) had a higher risk of CHD than did the other genotype group, based on 21 case-control studies.57
MTRR and MTR
A meta-analysis of 8 case-control studies examined the association between the methionine synthase reductase gene (MTRR) and the risk of CHD and showed that the G allele of the A66G polymorphism had a pooled OR of 1.35 (95% CI, 1.14–1.59) for CHD.66 However, there was no risk of CHD associated with the A2756G in this gene, based on 4 case-control studies. Similarly, a meta-analysis by Yu et al.,67 which included 8 case-control studies, also showed that the MTRR A66G polymorphism was associated with a higher risk of CHD, based on 8 case-control studies (G>A: pooled OR, 1.16; 95% CI, 1.01–1.33).
GATA4
Zhang et al.68 reported a meta-analysis of 11 case-control studies, and found that GATA 354A>C mutation was associated with an increased risk of CHD (pooled OR, 1.49; 95% CI, 1.15–1.93). However, neither GATA4 99G>T nor GATA 487C>T mutations were related to the incidence of CHD.
NKX2-5
Seven studies were included in a meta-analysis of the association between NKX2-5 63A>G and congenital heart disease in the Chinese population, which showed a pooled OR of 1.26 (95% CI, 1.02–1.56).69 Four studies included in meta-analysis showed no evidence for association between NKX2-5 60G>C and CHD.
SRD5A2
Six case-control studies were included in a meta-analysis that showed an increased risk of hypospadias associated with the V89L polymorphism of the steroid 5-alpha-reductase type 2 gene (SRD5A2), for the G vs C allele (pooled OR, 1.91; 95% CI, 1.13–3.23), GC vs GG genotype (pooled OR, 2.36; 95% CI, 1.35–4.13), GC+CC vs. GG genotypes (pooled OR, 2.46; 95% CI, 1.27–4.72), and CC vs. GC+GG genotypes (pooled OR, 1.91; 95% CI, 1.00–3.66).70
CFTR
Twenty-nine case-control studies were included in the meta-analysis investigating the association between congenital bilateral absence of the vas deferens (CBAVD) and polymorphism in CFTR.
71 Cystic fibrosis patients often carry variations in CFTR, which encodes a glycosylated transmembrane protein that is widely expressed in epithelial cells of exocrine tissues, including sweat glands, lungs, and vas deferens. Three variations showed significant associations with CBAVD: 5T (pooled OR, 8.35; 95% CI, 6.68–10.43), M470V (pooled OR, 0.74; 95% CI, 0.60–0.91), and ΔF508 (pooled OR, 22.20; 95% CI, 7.49–65.79).
1p22 and 20q12 anomalies
The C allele of a single nucleotide polymorphism at 20q12 (rs13041247), as opposed to the T allele, was associated with a reduced risk of cleft lip, with or without cleft palate, in a meta-analysis of 4 case-control studies (pooled OR, 0.63; 95% CI, 0.53–0.59).72 Moreover, the rs560426 A/G variant at 1p22 was associated with an elevated risk of cleft (pooled OR, 1.23; 95% CI, 1.04–1.47).
Go to :
DISCUSSION
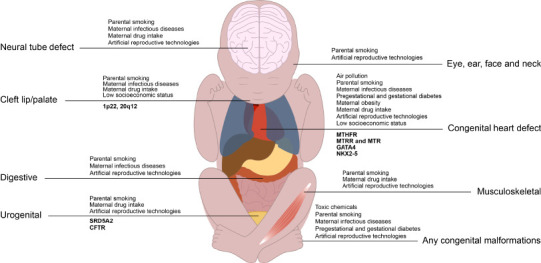
Overall, we reviewed 66 systematic reviews and meta-analyses that investigated the association between non-genetic or genetic risk factors and congenital anomalies. Seven categories of non-genetic and genetic risk factors were identified that showed association with congenital anomalies. We categorized congenital anomalies into CHD, cleft lip and/or palate, neural tube defects, defects in digestive, urogenital, and respiratory tracts, musculoskeletal anomalies, and eye, ear, face, and neck anomalies. Overall, 269 associations for non-genetic risk factors and 128 associations for genetic risk factors were found.
The risk of congenital anomalies was elevated by non-genetic risk factors, such as maternal exposure to environmental exposures (air pollution and toxic chemicals), parental smoking, maternal history (infectious diseases during pregnancy, PGDM and GDM, maternal obesity), maternal drug intake, pregnancy through ART, and socioeconomic factors (low SES). The association of maternal alcohol or coffee consumption with congenital anomalies was not significant, and maternal folic acid supplementation had a preventive effect on CHD. Genes or genetic loci associated with congenital anomalies included MTHFR, MTRR and MTR, GATA4, NKX2-5, SRD5A2, CFTR, and 1p22 and 20q12.
Exposure to NO2 increased the risk of CHD, while other pollutants showed no significant effect on CHD; however, more studies should be conducted because of the limitations of previous meta-analyses, such as small sample sizes. Air pollution could promote oxidative stress and increase production of free radicals, which may have developmental effects on the fetus.73 Oxidative stress due to air pollution has been reported to be associated with adverse birth outcomes.7475
The association between maternal alcohol consumption during pregnancy and congenital malformation was not significant. Alcohol consumption in pregnant women is socially considered as taboo; thus, women may underreport alcohol consumption status during surveys. Although maternal alcohol consumption was not associated with congenital anomalies in this study, alcohol is known to be a teratogen.76 Even a small amount of alcohol consumption at any point of pregnancy can have undesirable effects on the fetus, including small size for gestational age and preterm delivery.77 Heavy alcohol consumption during pregnancy can lead to fetal alcohol spectrum disorder (FASD) (an umbrella term including fetal alcohol syndrome (FAS), partial FAS, and alcohol-related neurodevelopmental disorder), manifested with intellectual disability and behavioral and developmental problems that may not necessarily be presented as congenital anomalies. Nonetheless, FASD most often co-occurs with congenital malformations in the heart, kidneys, or bones.78
Influenza could mediate teratogenic effects via several pathways; however, confounding due to the linkage between influenza and treatments with antipyretics or antivirals could be present. However, from the perspective of vaccination, whether the teratogenic effects are due to influenza or the drugs is not important, as vaccination would prevent both events.15 The pathways via which influenza leads to congenital anomalies are first, hyperthermia, and second, direct passage of virus through the placenta. Hyperthermia is reported to be associated with neural tube defects,79 and influenza virus can mediate teratogenic effects by placental transmission.80
CHD is associated with both maternal PGDM and GDM, but studies have shown that the associations with PGDM are stronger than those with GDM; this could be because GDM onset typically occurs after cardiac development.35 Previous studies have suggested that maternal hyperglycemia could disturb energy production during embryogenesis81 as well as the expression of PAX-3, which is a transcription factor for cardiac neural crest cells.8283 However, non-diabetic obese pregnant women also showed a greater risk CHD in the offspring.36 An explanation for this association is that obese pregnant women could be less responsive to folic acid supplementation at the standard dose than pregnant women who have a BMI in the normal range.84
A meta-analysis of 13 case-control and cohort studies showed that the use of beta-blockers during the first trimester increased the risk of CHD, cleft lip and palate, and neural tube defects.38 Beta-blockers are the most commonly prescribed antihypertensive drugs during the first trimester, and about 1 in 200 pregnant women are exposed to beta-blockers.85 Caton et al.85 pointed out that hypertension, which is an indication for beta-blockers, might be associated with congenital anomalies and act as a confounder in these associations. The estimated risk of beta-blockers in the study by Yakoob et al.41 was greater than the risk of hypertension itself, as shown in another study.86 However, none of the studies included in the meta-analysis compared the risk of malformation associated with beta-blockers in comparison to other types of antihypertensive medications.
The intake of fluoxetine increases the risk of congenital malformation and CHD. Fluoxetine is among the most commonly prescribed selective selective serotonin reuptake inhibitors (SSRIs) in the first trimester. While most SSRIs have a half-life of about 1 day, fluoxetine has a longer half-life (1–4 days) and its metabolite norfluoxetine has a half-life of approximately 7–15 days.87 Fluoxetine is known to cross the human placenta; a high concentration of fluoxetine and its metabolite are detected in umbilical cord blood.88 Although the mechanisms of fluoxetine-induced congenital anomalies are unknown, serotonin (5-hydroxytryptamine, 5-HT) is an important neurotransmitter for signaling during embryogenesis and cardiac morphogenesis.89 A mouse study showed that 5-HT has a direct effect on myocardial cell development90 and 5-HT affects cardiac morphogenesis during the formation of the endocardial cushion.91 Thus, it is suggested that healthcare providers and patients carefully consider the risk and benefit of fluoxetine therapy for depression during the first trimester.14
Two meta-analyses confirmed that folic acid supplementation intake reduces the risk of CHD, and most individual studies showed consistent results. According to a meta-analysis, the protective effect of folic acid supplementation against CHD is significant in China and Europe, but not in the United States, suggesting that it may be related to genetic background and environmental factors. The exact effects of folic acid supplements on heart formation are unknown, and more evidence is needed to support these findings.
Children born from pregnancies established by IVF and/or ICSI showed an increased risk of congenital defects. Excess risk of birth defects in these children may be due to the underlying infertility of the parents rather than ART itself.9293 Specific defects after ICSI may be associated with paternal subfertility against a particular genetic background.92 However, the procedure of ART itself may also increase the risk of adverse birth outcomes.94 It has been suggested that the risk of congenital anomalies in children born to parents who received ART should be compared with children born to infertile parents who spontaneously gave birth without ART, to assess the effect of ART per se on congenital anomaly.95 A previous study showed that parents who underwent ART generally had higher SES levels. These parents may have a stronger desire for a healthy pregnancy than those who conceived naturally, which may offset the risk of any adverse effects of the ART procedure.96
The 2 MTHFR polymorphisms, C677T and A1298C, are the most studied genetic factors associated with congenital anomalies, specifically CHD and orofacial cleft lips. MTHFR encodes the enzyme that catalyzes the reduction of 5, 10-methylenetetrahydrofolate to 5-methyltetrahydrofolate, which is a methyl donor to methionine.97 Thus, it is a crucial enzyme that connects the folate pathway and homocysteine metabolism.98 Mutation in MTHFR can cause inactivation or malfunctioning of the enzyme that breaks down the amino acid homocysteine and folate.55 The OR for the C677T polymorphism was much larger than that for the A1298C polymorphism. The risk of CHD associated with homozygosity was higher than that associated with heterozygosity; for example, recessive (TT vs. TC+CC) models were reported to have a greater effect than dominant models (TT+TC vs. CC). These results are not consistent with the fact that homozygosity for C677T results in 25% higher homocysteine levels than the normal genotype, which indicates low folate status.99
MTR encodes methionine synthase, an enzyme that transfers a methyl group from 5-methyl-tetrohydrofolic acid (5mTHF) to homocysteine and thus produces methionine and tetrahydrofolic acid (THF) by remethylation. In the early stage of embryo development, this methylation is the only method by which homocysteine is reduced and methionine is produced, and thus a defect in this gene can lead to folic acid metabolic disorder.67
MTRR encodes methionine synthase reductase, which plays an important role in inactivating methionine synthase. Therefore, defects in MTRR may disrupt the course of embryonic development by influencing the levels of homocysteine, 5mTHF, THF, and methionine.
NKX2-5 and GATA4 are cardiac transcription factors that regulate heart development.69
NKX2-5 has been shown to participate in heart development not only in animal models, such as zebrafish, frog, chicken, and mouse, but also in humans in previous family studies.69 During the first trimester of gestation, male external genitalia are developed by regulation of androgens, such as testosterone and dihydrotestosterone. Since SRD5A2 plays a role in androgen synthesis and metabolism, it may have an effect on the differentiation of genitalia in males.
This study had several limitations. First, it did not review individual articles that were not included in the systematic reviews and meta-analyses. Thus, certain categories of risk factors could have been missed. Second, the same article may have been included in several systematic reviews and meta-analyses. The availability of several meta-analyses on a topic does not necessarily mean that there are a greater number of individual articles published on the specific topic. Thus, caution is needed in interpreting the level of evidence based on the number of meta-analyses available. Third, the quality of the studies included in this systematic review was mostly low or very low according to the AMSTAR2 criteria. The main reason for the low quality was the lack of a reference list for the studies excluded from each meta-analysis. Although AMSTAR2 provides a valuable guideline for evaluating the quality of meta-analyses and for performing meta-analyses, it may be too strict to apply to the currently available literature because few studies satisfied the AMSTAR2 criteria for high quality meta-analyses. Fourth, it should be noted that case-control studies included in each meta-analysis could be subject to recall bias, which can be quite influential in studies of congenital anomalies, where mothers tend to have feelings of guilt.100
Despite these limitations, this study provided comprehensive information regarding both non-genetic and genetic risk factors of congenital anomalies, providing insight into which topic requires further studies. Suggestions for future studies include the following. First, it is necessary to analyze the disease burden of each risk factor of congenital anomalies by taking effect sizes and prevalence into account. There is a lack of systematic reviews that suggest health policy priorities for preventing congenital anomalies by considering the burden of disease of each individual risk factor. Second, there are relatively few systematic reviews and meta-analyses of studies on environmental and occupational risk factors for congenital anomalies. Not only toxic chemicals, but also occupational risk factors could affect birth outcomes. For example, studies on the effects of night shift work on congenital anomalies are very rare. This study provided a very comprehensive umbrella review of risk factors of congenital anomalies. Modifiable risk factors, such as maternal behaviors, medication, supplementation, and possibly environmental hazards, should be carefully considered to achieve better birth outcomes. Allocation of social resources is warranted to support such modifications, to protect mothers and children from congenital anomalies that could permanently affect development and function in children.
In conclusion, from umbrella review of systematic review and meta-analysis studies, we identified 66 studies reporting non-genetic and genetic risk factors of congenital anomalies, such as air pollution, toxic chemicals, parental smoking, alcohol consumption, maternal infectious diseases, pregestational diabetes, maternal obesity, maternal drug intake, maternal supplementation, maternal diet, and several genetic factors polymorphisms in MTHFR, MTRR and MTR, GATA4, NKX2-5, SRD5A2, CFTR, 1p22, and 20q12. Further studies are warranted to identify more diverse risk factors of congenital anomalies and elucidate the mechanisms of congenital anomalies.
Go to :
 XML Download
XML Download