

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Asthma is the most common chronic inflammatory airway disease on a global scale.12 It is characterized by airway hyper-responsiveness and variable expiratory airway limitation; it is associated with poor quality of life, increased risk of acute exacerbation of asthma, and increased need for health-care resources.3 Although three of four children with childhood asthma outgrow it by mid-adulthood,4 several studies have reported that childhood asthma could hinder pulmonary functions in adulthood.5678 A United States (US)-based study of adults with childhood asthma found that moderate-to-severe allergic asthma in childhood caused irreversible damage to the pulmonary function in adulthood due to airway remodeling from repeated chronic inflammation of the airway.9 Therefore, it is important to prevent asthma onset and exacerbation of asthma.10
One of the environmental risks factors of childhood asthma is exposure to environmental tobacco smoke (ETS).11 It is a known modifiable risk factor involved in the development and exacerbation of childhood asthma.121314 Exposure to cigarette smoke increases the expression of TLR4 on the airway epithelial surface and induces a decrease in the threshold of allergen recognition. Increased expression of reactive oxygen species and epithelial cytokine (IL-33, TSLP) expression disrupts the epithelial barrier function,1516 and promotes allergic sensitization by Th2 immunity.171819 Parental smoking is a common cause of exposure to ETS among children.20 A systematic review and meta-analysis of a birth cohort reported that prenatal maternal smoking had a significant association with wheezing and asthma in the offspring.21 Wang et al.22 found that ETS doubled the severity of asthma in children, including the risk of hospitalization for exacerbation and reduced pulmonary function.
However, about 70% of previous studies identified parental smoking status solely using self-reported data,22 which may be underestimated due to biased recalls or fear of social stigma.2324 Cotinine is the main metabolite of nicotine and is considered a biomarker of tobacco smoking status. A Korean study on the discrepancy between self-reported and cotinine-verified smoking status showed that the rate of cotinine-verified smoking was 11.1% higher than the self-reported smoking rate.25 In pregnant women, the percentage of self-reported active smoking was 0.55%, but the percentage of cotinine-validated active smoking was 3.03%.26 It is important to investigate the accurate parental smoking status using a biomarker rather than self-report to make a strategy for preventing childhood asthma, but there are very few studies on the parental urinary cotinine level in children with asthma in Korea. Therefore, we hypothesized that parental urinary cotinine-verified smoking status would be significantly associated with childhood asthma. In this study, we evaluated the status of parental smoking and the correlation between children's asthma status and parental urinary cotinine-verified smoking status using nationally representative data.
Go to : 
METHODS
Study populations and design
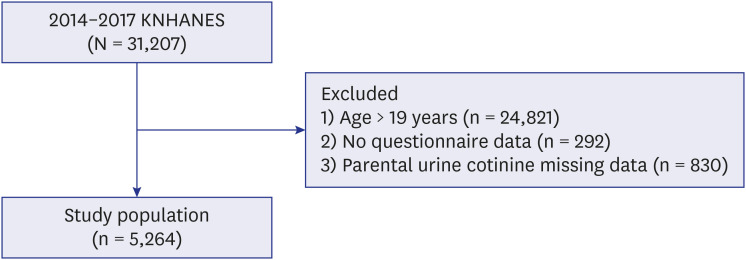
Data from the Korean National Health and Nutrition Examination Survey (KNHANES) between 2014 and 2017 were used. The KNHANES is an annual nationwide cross-sectional survey that has been used to evaluate health status and dietary intake as well as health examinations by the Korean Center for Disease Control and Prevention.27 In the present study, 5,264 subjects aged under 19 years who participated the KNHANES survey and with data on paternal or maternal urinary cotinine levels were included (Fig. 1).
Data collection
Sociodemographic variables including age, sex, levels of education, household income, occupation, and tobacco smoking status were collected during face-to-face interviews. Household income levels were categorized as low, lower middle, higher middle, and high according to the quartiles of monthly family income. Levels of education were categorized into four groups: elementary, middle school, high school, and college or higher. In the present study, occupations were reclassified into five categories from 11 occupation groups based on the Korean Standard Classification of Occupations of the Korea National Statistical Office: professional and manager, non-manual, skilled, unskilled workers, and unemployed. Parental cotinine-verified smoking status was categorized into three groups according to self-reported smoking status and urinary cotinine levels (active smoker, passive smoker, and non-smoker). Parents were asked the following questions: “How many cigarettes did you smoke in your lifetime?” and “Do you currently smoke?”. If the participants responded that they had smoked 100 cigarettes or more in their lifetime and that they smoke currently, they were categorized as “active smokers”. Parents who were exposed to tobacco smoke either at home or in the workplace during the previous week and did not currently smoke were categorized as “passive smokers”. Non-smokers were defined as participants who did not smoke currently and were not exposed to ETS. In addition, non-smokers were reclassified as active smokers or passive smokers if their urinary cotinine concentrations were > 50 ng/mL or 5–50 ng/mL, respectively. Body mass index (BMI) was measured as weight in kilograms divided by the height in squared meters. BMI was classified into underweight (BMI < 18.5 kg/m2), normal (BMI = 18.5–24.9 kg/m2), overweight (BMI = 25–29.9 kg/m2) and obesity (BMI ≥ 30 kg/m2) according to World Health Organization (WHO) guidelines. Diagnosis of asthma, atopic dermatitis (AD), and allergic rhinitis (AR) were defined by responders providing a positive response to the following questions: “Were you ever diagnosed with asthma, AD, and AR by a physician?”
Measurement of urinary cotinine levels
A random urine sample was collected from the participants. Urinary cotinine concentration was measured by gas chromatography and mass spectrometry using the Agilent 110 Series with API 4000 (AB Sciex, Framingham, MA, USA). The lower limit of detection for urinary cotinine was 0.27 ng/mL.
Statistical analysis
Because the KNHANES uses a complex, multistage, and clustered probability design to select participants who represent the non-institutionalized Korean population, we applied sample weights to all analyses. Survey weights take into account non-response, oversampling, post-stratification, and sampling error. The primary outcome was the incidence of childhood asthma. We compared normally distributed continuous variables and categorical variables between the asthma and non-asthma groups using the t-test and the χ2, respectively. The parental urinary cotinine concentration was naturally log-transformed. Pearson correlation analysis was used to determine the association between paternal and maternal urinary cotinine levels. Multivariable logistic regression was used to identify the parental cotinine-verified smoking status associated with childhood asthma. The adjusted odds ratio (aOR) from ordered logistic regression models were presented with 95% confidence intervals (CIs). Statistical analyses were performed using the STATA version 16 (StataCorp LLC, College Station, TX, USA). A P value of less than 0.05 was considered significant.
Ethics statement
This study was approved by the Institutional Review Board (IRB) of Kosin University Gospel Hospital (IRB file No. KUGH 2019-12-037). Given that the databases used in this present study included only de-identified data, informed consent was not required.
Go to :
RESULTS
Characteristics of pediatric population
Table 1 shows the clinical characteristics of the study subjects. The weighted mean (standard error [SE]) age of the study population was 10 (0.1) years, and the weighted proportion (SE) of boys was 52.2 (0.6%). Of the total 5,264 study subjects, 176 (3.3%) responded that they had ever been diagnosed with asthma. The weighted mean (SE) ages of the asthma and non-asthma groups were 11.3 (0.4) years and 9.9 (0.1) years, respectively (P < 0.001). The weighted proportions (SE) of males in the asthma and non-asthma groups were 58.7 (2.8%) and 52.0 (0.6%), respectively (P = 0.024). The weighted proportion of body weight by age was > 95‰ in the asthma group (20.4%) and was significantly higher than that in the non-asthma group (0.9%) (P < 0.001). The weighted proportions of AD and AR in the asthma group were significantly higher than those in the non-asthma group (P < 0.001). Although there was no significant difference in the history of parental and paternal allergic diseases between the asthma and non-asthma groups, the weighted proportions of maternal asthma and AD were significantly higher in the former than those in the latter (P < 0.001). The weighted mean (SE) paternal urinary cotinine level was 872.9 (106.7) ng/mL in the asthma group and 643.3 (21.8) ng/mL in the non-asthma group (P = 0.026). There was no significant difference between the groups in terms of residential region, paternal and maternal urinary cotinine-verified smoking status, and maternal urinary cotinine levels.
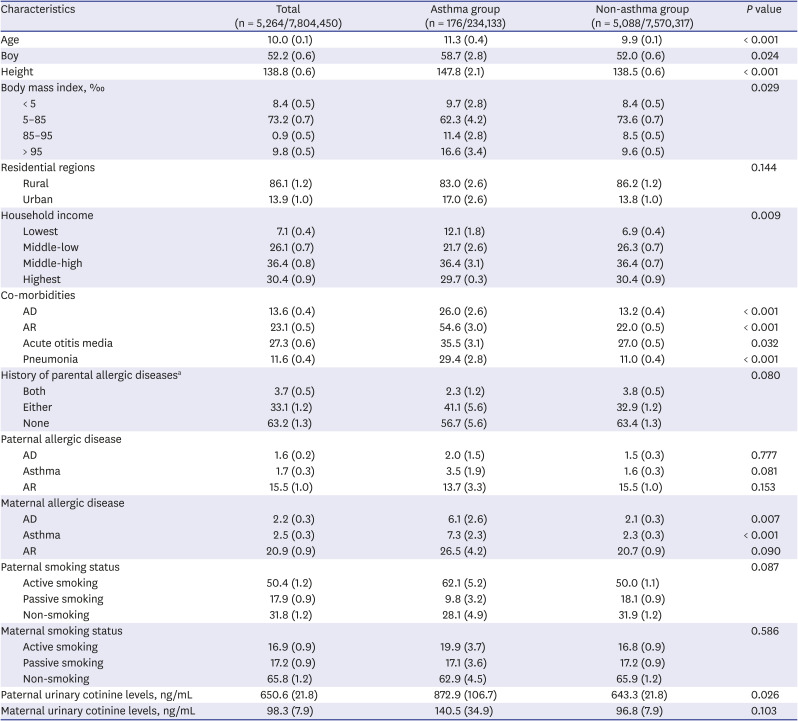
Table 1
Clinical characteristics of study population
Percentages and means were weighted. Number indicated unweighted sample number/weighted sample number.
AD = atopic dermatitis, AR = allergic rhinitis.
aHistory of parental allergic diseases was defined if parents had ever been diagnosed with atopic dermatitis, asthma, or allergic rhinitis.
![]()
Clinical characteristics of parents according to urinary cotinine-verified smoking status
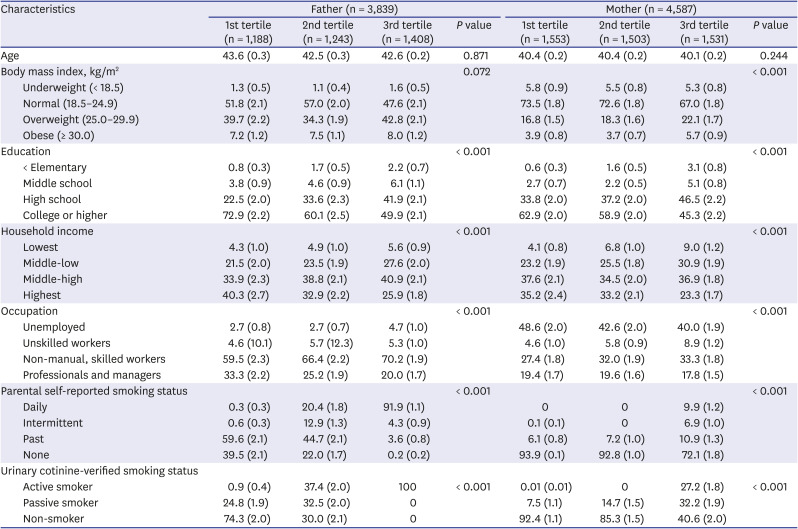
The range of paternal urinary cotinine concentration was divided into 1st (< 0.941 ng/mL), 2nd (0.942–680 ng/mL), and 3rd tertile (686–5,030.8 ng/mL), and maternal urinary cotinine concentration was divided into 1st (< 0.51 ng/mL), 2nd (0.511–1.21 ng/mL), and 3rd tertile (1.22–4,896.0 ng/mL). When paternal urinary cotinine levels increased, the weighted proportions of high education level, high household income, and professional occupation decreased, while those of low education level, low household income, and unemployment increased (P < 0.001) (Table 2). Maternal urinary cotinine level increased with high BMI, low level of education, and low household income (all P < 0.001) (Table 2). Paternal and maternal urinary cotinine levels were significantly associated (r = 0.19, P < 0.001) (Fig. 2).
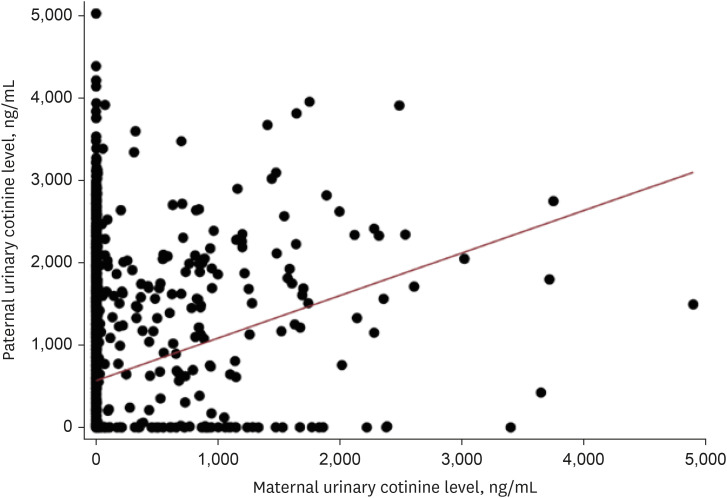 | Fig. 2Correlation between paternal and maternal urinary cotinine levels. Maternal urinary cotinine levels were positively associated with paternal urinary cotinine levels (r = 0.19; 95% confidence interval, 0.17–0.23; P < 0.001)
|
Table 2
Demographic characteristics of parents by urinary cotinine levels
![]()
Trends in parental smoking status and incidence of childhood asthma
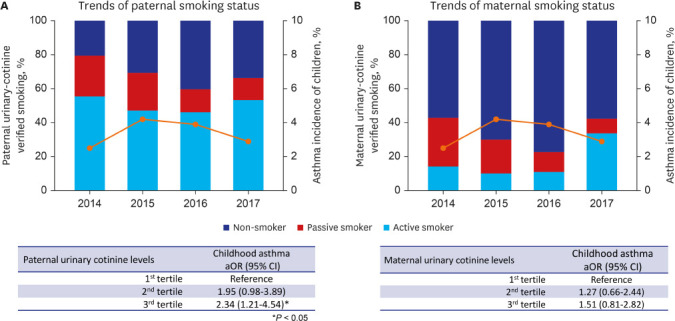
The proportions of paternal active smokers in 2014, 2015, 2016, and 2017 were 55.4%, 47.2%, 46.2%, and 53.3%, respectively, and the proportions of paternal non-smokers increased every year (20.6% in 2014, 30.7% in 2015, 40.4% in 2016, and 33.7% in 2017; Ptrend = 0.001) (Fig. 3A). The proportion of maternal active smoking abruptly increased in 2017 (33.7%) from that in 2014 (14.2%; Ptrend < 0.001) (Fig. 3B). The annual incidence rates of asthma showed no significant changes (2.5% in 2014, 4.2% in 2015, 3.9% in 2016, and 57.7% in 2017; P = 0.146).
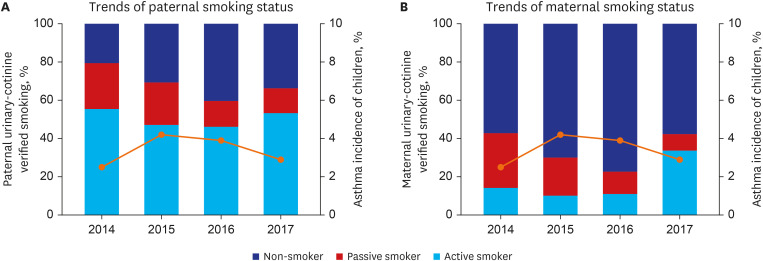 | Fig. 3Trends of parental smoking status and incidence of childhood asthma by year. (A) The proportion of paternal non-smoker increased every year (Ptrend = 0.009). (B) The proportion of maternal active smoking abruptly increase in 2017 (Ptrend < 0.001). Asthma incidence showed no significant annual changes (P = 0.991).
|
Association of parental smoking status and the incidence of childhood asthma
There was no significant association between urinary cotinine-verified status and childhood asthma. However, higher levels of paternal urinary cotinine were associated with the diagnosis of asthma in their children (aOR, 1.08; 95% CI, 1.01–1.15) (Table 3). In addition, the highest paternal urinary cotinine level tertile (vs. the lowest) was associated with pediatric patients with asthma (aOR, 2.34; 95% CI, 1.21–4.54) (Table 3). A dose-dependent relationship was observed in patients with asthma who had AR comorbidity (aOR, 2.31; 95% CI, 1.07–4.97 in the 2nd tertile vs. 1st tertile; aOR, 2.45; 95% CI, 1.16–5.18 in the 3rd tertile vs. 1st tertile) and was more significant than in patients without AR (aOR, 1.77; 95% CI, 0.67–4.67 in the 2nd tertile vs. 1st tertile; aOR, 2.71; 95% CI, 1.09–6.79 in the 3rd tertile vs. 1st tertile) (Table 4). The aORs of childhood asthma increased with maternal urinary cotinine levels, but the association was not statistically significant. Doctor-diagnosed asthma was not significantly associated with paternal or maternal urinary cotinine-verified active smoker status (fully aOR, 1.57; 95% CI, 0.77–3.22) (Table 3).
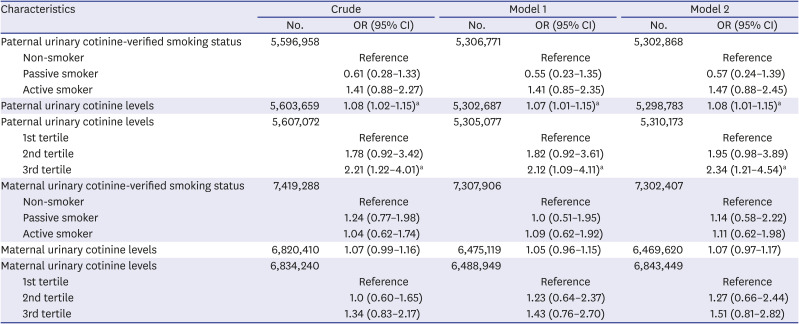
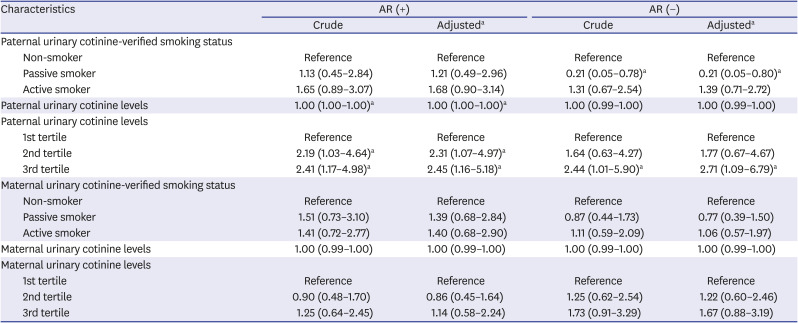
Table 3
Association of parental smoking status and the incidence of childhood asthma
Model 1 was controlled for sex, age, weight for age, household income, residential area, and family history of allergic diseases, and model 2 was further controlled for atopic dermatitis and allergic rhinitis. Number indicated weighted sample number.
OR = odds ratio; CI = confidence interval.
aP < 0.05.
![]()
Table 4
Association of parental smoking status and the incidence of childhood asthma according to presence of AR
Values are presented as odds ratio (95% confidence interval).
AR = allergic rhinitis.
aAdjusting for sex, age, weight for age, household income, residential area, and family history of allergic diseases.
![]()
Go to :
DISCUSSION
To our knowledge, this is the first study to investigate the association between parental cotinine-verified smoking status and childhood asthma in Korea, using nationally representative data. We found that high levels of paternal urinary cotinine levels were significantly associated with childhood asthma. Although exposure to ETS is a preventable risk factor for childhood asthma, our data showed that parental smoking is persistently high in Korea. It is necessary to develop a detailed strategy for parents with active smoking status to prevent damage to their own respiratory health and that of their children.
Parental smoking is a common source of ETS for children at home. In the present study, there was no significant difference among urinary cotinine-verified active, passive, and non-smokers for childhood asthma. However, higher paternal urinary cotinine levels were significantly associated with the risk of childhood asthma. This discrepancy may be because the definition of urinary cotinine-verified active smoking (above 100 ng/mL) and the tertile level of urinary cotinine level (the highest tertile, 686–5,030.8 ng/mL) were different. Our results suggest that there is a dose-dependent relationship between urinary cotinine levels and childhood asthma. This dose-dependent relationship is similar to that reported in previous studies that evaluated the relationship between exposure to ETS at home and prevalence of childhood asthma. A cross-sectional study of children in Singapore showed that high prevalence rates of doctor-diagnosed asthma were directly associated with the numbers of cigarettes smoked by the parents.28 The US survey data showed that high serum cotinine levels in children were significantly associated with the risk of asthma in children aged 3–11 years.29 A dose-response relationship between the number of smokers in a household and the odds of current cases of asthma in the adolescent population was observed in Brazilian study.30 A multicenter, multi-country, cross-sectional study also showed an association between the increased risk of severe asthma in the offspring and number of cigarettes smoked per day by the father.31 However, our results do not indicate that smoking less is not influenced by children's respiratory health. A US-based study on children with asthma indicated that those with high secondhand smoke (SHS) exposure (serum cotinine level, > 3.0 ng/mL) and low SHS exposure (serum cotinine level, 0.05–2.99 ng/mL) were more likely to have an emergency visit and higher number of hospitalizations than children with asthma who are not exposed to SHS.32 In addition, we found that the dose-dependent relationship in the asthmatic patients with AR was clearer than that of patients without AR. Asthmatic patients with AR were more likely to have allergen sensitization than those without AR. The present results suggest that ETS exposure could be related to asthma with allergen sensitization or allergic disease multimorbidity. A study for Korean adolescents found that ETS exposure at multiple sites was more likely to be associated with multiple allergic diseases.33 A prospective birth cohort study showed a dose-response effect of parental smoking at home on inhalant and food sensitization.34 Previous studies supported these results that ETS could alter the immune response by impairing Th1-type and aggravating Th2-dependent responses.353637
We did not find a significant association between current maternal urinary cotinine levels and childhood asthma. While many pieces of evidence show that maternal smoking during pregnancy increases the risk of childhood asthma3839 by oxidative DNA damage and by altering the development of the pulmonary system,40 there are inconsistent findings on the relationship between current maternal ETS and the prevalence of childhood asthma.41 A pooled analysis of 12 cross-sectional studies on the relationship between different periods of ETS and childhood asthma showed that the fully aOR of the association between current parental smoking and childhood asthma was not statistically significant.42 A US-based study reported that current ETS exposure was not significantly associated with physician-diagnosed asthma in children.43 However, a recent cross-sectional study of adolescents in Middle Eastern countries showed a significant relationship between current ETS exposure at home and self-reported asthma.44 These contradictory findings can be attributed to different measurements of ETS exposure (various questionnaire items), different adjusted confounders used in statistical analyses, differences in time to diagnosis, and difficulty in distinguishing between the effects of exposure to ETS by paternal and maternal smoking. The mothers of our subjects first started smoking in their 20s (data not shown), and it is unclear whether they smoked during pregnancy. The little effects of current maternal ETS on childhood asthma in the present study is probably because the maternal urinary cotinine levels were much lower than the paternal urinary cotinine levels.
In the present study, half of the fathers and 16.9% of the mothers were cotinine-verified active smokers; the paternal smoking rate in our data was much higher than that reported in other countries.4546 The International Study of Asthma and Allergies in Childhood reported in Phase Three (2000–2003) indicated that the prevalence of current paternal smoking was 4.2–67.8% (Korea: 67.8%).31 The WHO recently reported that the number of males smoking tobacco products globally was on the decline, but a high prevalence of smoking is still observed in East Asian countries,47 approximately 49.8% of Korean men. During our study period, paternal smoking rates were similar throughout the years and non-smoking rates increased, but maternal smoking rates showed an increasing trend.46 Data from the KNHANES showed that rate of young female smokers increased by two times in 20 years, although it was still lower than the rate of male smokers.45 This trend of female smoking rate in South Korea was similar to the trend in the mid-twentieth century in the US, where the rate of female smokers started increasing, almost reaching the rate of male smokers, given the increased social acceptance of the smoking habits of women.48 Recently, the rate of female smokers showed a declining trend in high-income countries. In England, SHS exposure among children declined by 79% since 1998.49 A study on the smoking rates of the general female population in Western industrialized countries showed that the smoking rates ranged from 20% to 30% in 2000 and declined substantially to around 15% in 13 years.50 The American Lung Association analysis of Center of Disease Control data showed that rate of female smokers declined from 17.4% in 2007 to 12.2% in 2017.51 Thus, understanding the current smoking status of parents is important to design strategies to reduce ETS exposure in Korean children, with reference to interventions in other countries.
The current findings showed differences in parental urinary cotinine levels according to socioeconomic levels, consistent with previous findings of high ETS in children being associated with household income and parental education levels.5253 The current findings showed differences in parental urinary cotinine levels according to socioeconomic levels, consistent with previous findings of high ETS in children being associated with household income and parental education levels.54 Data from the KNHANES indicated that serum cotinine levels in children increased by 1.18 ng/L for a unit decrease in the family poverty income ratio.55 A meta-analysis of 41 studies indicated that low level of parental education was independently associated with ETS exposure in children at home.56 Thus, children in families with low socioeconomic status should be considered the key target groups for tobacco-control interventions.
Our study had several limitations. First, we relied on self-reported doctor-diagnosed asthma. In particular, it was possible to misdiagnose asthma in this study because it is not easy to make a diagnosis of asthma in children aged 5 years and younger. Second, because of the cross-sectional nature of the study, the children's exposure to tobacco was measured at one point in time; point prevalence assessment of urinary cotinine levels is useful for assessing ETS.57 We were not able to obtain data such as time-activity patterns and the degree of smoke exposure in the home environment. In addition, there was no information about current asthma symptoms and medication use in the KNHANES data participants under the age of 19 years. Therefore, the causality of the present association should be cautiously interpreted. Third, other factors associated with the risk of asthma in children, such as air pollution, pets, and allergens, were not considered. However, despite these limitations, the current study, using national representative data, outlines the importance that the percentage of children's ETS was high, and this had a significant association with the risk of childhood asthma.
We found that the proportion of paternal cotinine-verified active smokers was still high, and the proportion of maternal active smokers has been increasing recently in Korea. The proportion of parental low household income was increased when parental urinary cotinine level increased. In addition, it seems to be in a dose-related association between paternal urinary cotinine levels and the risk of childhood asthma. Because physicians are in the ideal position to counsel families, it is important to recognize children at high risk of ETS exposure. Additional studies are needed to develop an effective strategy to reduce parental smoking for childhood asthma.
Go to :
 XML Download
XML Download