

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Mental health problems have become an emerging overriding burden of disease in Korea. An epidemiological survey on mental health conducted every 5 years reported that the lifetime prevalence of mood disorders and suicidal thoughts were 5.3% and 15.4%, respectively [1]. Korea's suicide rate is the 2nd highest (24.6 per 100,000 population) among the Organization for Economic Co-operation and Development nations [2].
Epidemiological studies have provided increasing evidence that a poorer diet quality increased the risk of developing psychiatric symptoms, such as depression and anxiety, and nutrition has been implicated in the prevention and treatment of mental illness [34].
On the other hand, Korean studies on the relationship between diet patterns and mental illness are rare. Recent research [5] examining the association between the dietary patterns and depression in middle-aged Korean adults revealed a negative association of healthy dietary pattern (rich in vegetables, soybeans, mushroom, seaweeds, white fish, shellfish, and fruits) and a positive association of an unhealthy dietary pattern (rich in white rice, meats, ramen, noodles, bread, and coffee) with depression. This study was the first to investigate the relationship between the dietary patterns and depression in Koreans, but it was limited to middle-aged adults and could not assess the overall food quality. In addition, few studies have examined the association between psychiatric distress, such as stress and suicide, other than depression, and the diet quality of Koreans. Recently, the Korean healthy eating index (KHEI) for adults was newly developed to evaluate the diet quality of Korean adults. This study evaluated the association of depressive symptoms, stress perception, and suicidal ideation with the overall dietary quality using the newly developed KHEI.
Go to : 
SUBJECTS AND METHODS
Study population
This study used data from the 6th Korea National Health and Nutrition Examination Survey (KNHANES) 2013 and 2015. KNHANES is a nationwide survey using a stratified multistage probability sampling design and consists of a health interview, behavioral and nutritional surveys, and a medical examination. Additional details regarding the study design and methods are reported elsewhere [6]. Of 12,058 adults aged 19 years or older who participated in the 6th KNHANES 2013 and 2015, 10,124 individuals participated in all the health interviews, behavioral and nutritional surveys, and medical examinations. Individuals with missing data from questions on depressive symptoms (n = 603), stress (n = 604), suicidal ideation (n = 602), and healthy eating index (HEI; n = 69) were excluded. Finally, 9,607 adults (3,939 men and 5,668 women) were included in the analysis.
Ethical approval
The protocol of 2013-2015 KNHANES was approved by the Institutional Review Board (IRB) of the Korea Centers for Disease Control and Prevention (IRB approval number in 2013 and 2015: 2013-07CON-03-4C and 2015-01-02-6C). Written informed consent was obtained from all the participants.
Measurement of psychological distress
Trained interviewers measured the depressive symptoms, stress perception, and suicidal ideation to assess psychological distress from the behavioral health survey questions. The depressive symptoms were assessed using the following question: “Have you ever felt sad or hopeless enough to disrupt your daily life for more than 2 weeks in a row during the past year?” The “yes” or “no” response was used to determine if the participants had depressive symptoms. To assess the stress perception, participants were asked how stressed they were on a daily basis. When participants responded to feel “extremely or quite stressed” in their daily lives, stress perception was classified as “yes”. The “a little or hardly stressed” was classified as no stress perception. Suicidal ideation was measured by the question of whether the participants had seriously thought of committing suicide during the past year. The “yes” or “no” response was used to classify their suicide ideation.
Dietary assessment and the KHEI
The dietary intake was assessed by a trained nutritionist using a food frequency questionnaire (FFQ) and 24-hour-recall from a nutritional survey. KHEI scores were calculated using the FFQ data. The KHEI was developed to assess the overall diet quality in Korean adults. The KHEI was composed of 8 adequacy components (breakfast, whole grains, fruits, vegetables, meat/fish/eggs and beans, and milk and dairy), 3 moderation components (saturated fatty acids, sodium, and sweets and beverages), and 3 balance components (carbohydrates, total fat, and energy). The maximum KHEI score was 100 points, and the minimum score was 0; a higher score means more adherence to a healthier diet. The KHEI components and standards for scoring the details are reported elsewhere [7].
Assessment of covariates
The height and weight were measured to the nearest 0.1 cm using a portable stadiometer (Seriter, Bismarck, ND, USA) and the nearest 0.1 kg using a Giant-150N calibrated balance-beam scale (Hana, Seoul, Korea), respectively [8]. The body mass index (BMI) was calculated by dividing the weight in kilograms by the height in meters squared. The blood pressure (BP) was measured using a mercury sphygmomanometer in the seated position after 5 minutes of rest 3 times. The mean of the 3 measurements was used for systolic BP (SBP) and diastolic BP (DBP). Hypertension was defined as SBP ≥ 140 mmHg, DBP ≥ 90 mmHg, or current intake of antihypertensive medications. Blood samples were collected in the fasting state. The fasting blood sugar (FBS) and total cholesterol (TC) were analyzed enzymatically (COBAS 8000 C702; Roche, Risch-Rotkreuz, Switzerland). Type 2 diabetes was defined as FBS levels of ≥ 126 mg/dL or the use of insulin or oral glucose-lowering medication. Hypercholesterolemia was defined as TC levels of ≥ 240 mg/dL or current intake of cholesterol-lowering medications.
The health interview and behavioral surveys contained demographic, socioeconomic and lifestyle factors, including age, sex, family income, presence of a spouse, smoking habits, alcohol consumption, and physical activity. Family income was categorized into 5 groups: < 100 × 104 (Korean currency; 1 dollar = 1,220 won), 100–199 × 104, 200–299 × 104, 300–399 × 104, 400–499 × 104, and ≥ 500 × 104 won/month. The smoking status was divided into 3 categories: current smoker, ex-smoker, and never smoker. Alcohol consumption was divided into 4 groups according to the average amount of alcohol consumed per day: none, 1–14.9, 15–29.9, and ≥ 30 g/day. The total weekly metabolic equivalents of the task energy expenditure was calculated using the reported minutes per week of walking, moderate, and vigorous activity [910].
Statistical analysis
Statistical analyses were performed using STATA (version 14.2; Stata Corp., College Station, TX, USA) according to the analytical guidelines to reflect the complex sampling design [11]. The survey sample weights were used for all analyses to extrapolate the findings to the entire Korean population. The continuous variables were reported as the means with SEs and categorical variables as percentages.
The KHEI score was divided into sex-specific quartiles to analyze the associations with depressive symptoms, stress perception, and suicidal ideation. Differences between the groups were tested using survey regression analysis for the continuous variables and a χ2 test for the categorical variables. A Bonferroni post hoc test was used to determine the significance of the differences in the continuous variables according to the quartile of KHEI. Survey logistic regression analyses controlling for age (continuous), BMI (continuous), family income level (< 100 × 104, 100–199 × 104, 200–299 × 104, 300–399 × 104, 400–499 × 104, and ≥ 500 × 104 won/month), smoking status (current smoker, ex-smoker, and never smoker), daily alcohol intake (none, 1–14.9, 15–29.9, and ≥ 30 g/day), total weekly physical activity, total daily energy intake (kcal/day), spouse (yes or no), type 2 diabetes (yes or no), hypertension (yes or no), and hypercholesterolemia (yes or no) were performed to determine if the KHEI scores were independently associated with the presence of psychologic distress using the lowest quartile of the KHEI scores as a reference. This study also tested for the linear trends across the increasing quartile of KHEI as entering the quartile categories as a continuous term in the model. A P-value < 0.05 was considered significant.
Go to :
RESULTS
General characteristics of the subjects
The mean age of the study population was 45.1 ± 0.33 years in men and 47.1 ± 0.34 years in women (P < 0.001). The percentage of subjects with experience of a depressive mood, higher stress perception, and suicidal ideation was 8.2%, 25.0%, and 3.7% in men and 15.4%, 27.3%, and 6.0% in women, respectively. The mean KHEI score was 61.5 ± 0.29 in men and 64.8 ± 0.24 in women, respectively (P < 0.001).
Table 1 lists the characteristics of the participants according to the quartiles of the KHEI score. Age showed a significant difference according to the KHEI score among men (P < 0.001) and women (P < 0.001). Both men and women in group Q4 (highest KHEI score) were more likely to be at a high level of household income and be non-drinkers, but less likely to be current smokers, compared to those in group Q1 (lowest KHEI score). The total daily calorie intake was lower in the women in group Q1 compared to other groups (P < 0.001), but the total daily calorie intake in men was similar regardless of the quartiles of the KHEI score.
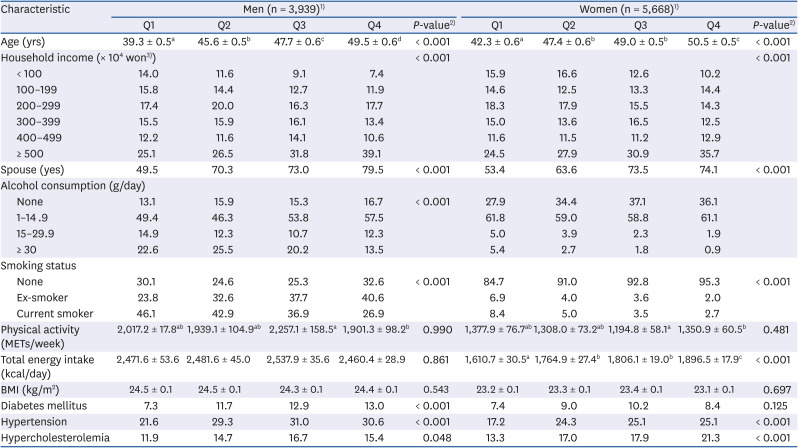
Table 1
Characteristics of participants according to the quartiles of KHEI scores
Values are reported as the mean ± SE or percentages. Different superscript letters are significantly different (P < 0.05 by Bonferroni post hoc test).
Cutoff values for quartiles of KHEI are as follows: for men Q1, 17.6–54.2; Q2, 54.3–63.4; Q3, 63.5–71.6; and Q4, 71.7–99.1; for women Q1, 19.6–56.8; Q2, 56.9–66.0; Q3, 66.1–74.8; and Q4, 74.9–99.6.
KHEI, Korean healthy eating index; MET, metabolic equivalent; BMI, body mass index.
1)Number was represented by the unweighted sample.
2)Differences between groups were tested using a survey linear regression analysis for continuous variables and a χ2 test for categorical variables.
3)Won, Korean currency.
![]()
Prevalence of psychological distress according to the quartiles of the KHEI score and gender
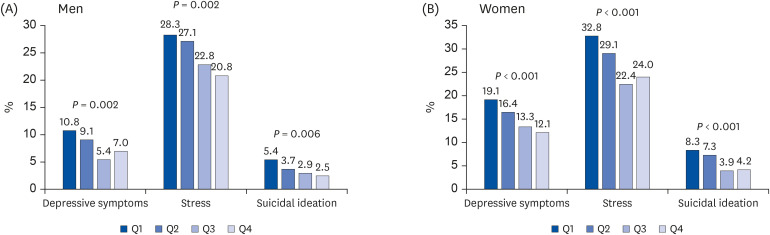
Fig. 1 shows the percentages of depressive symptoms, stress perception, and suicidal ideation according to the quartiles of the KHEI score. Both men and women with the highest quartile of the KHEI score had lower rates of depressive symptoms (highest vs. lowest, 7.0% vs. 10.8%, P ≤ 0.002 in men and 12.1% vs. 19.1%, P < 0.001 in women), stress perception (20.8% vs. 28.3%, P = 0.002 in men and 24.0% vs. 32.8%, P < 0.001 in women), and suicide ideation (2.5% vs. 5.4%, P = 0.006 in men and 4.2% vs. 8.3%, P < 0.001 in women) than the lowest quartiles.
Component of KHEI according to psychological distress and gender
Tables 2 and 3 list the differences in diet quality among men and women with or without psychological distress. Men with depressive symptoms had a lower HEI component score for meat, fish, eggs, and beans than non-depressed men (7.38 vs. 6.93, P = 0.046). Women with depressive symptoms had lower HEI component scores for the total vegetables and vegetables, excluding Kimchi and pickles consumption compared to women without depressive symptoms (3.35 vs. 3.17, P = 0.007 and 3.18 vs. 3.02, P = 0.042, respectively). Women with suicidal ideation also had lower HEI component scores for the total vegetables and vegetables, excluding Kimchi and pickles consumption, compared to women without suicidal ideation (3.34 vs. 3.09, P = 0.017 and 3.17 vs. 2.91, P = 0.017, respectively). The men with stress had a lower breakfast eating score than those without stress (7.21 vs. 6.77, P = 0.016).
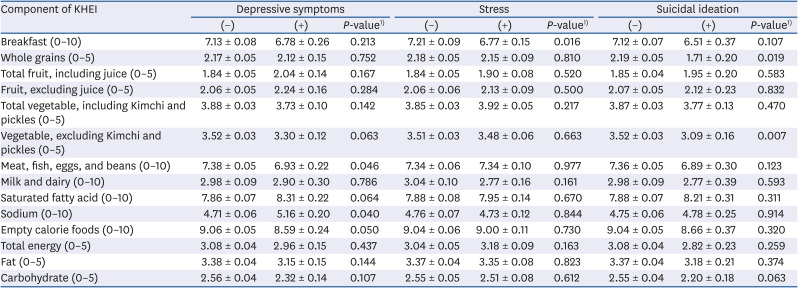
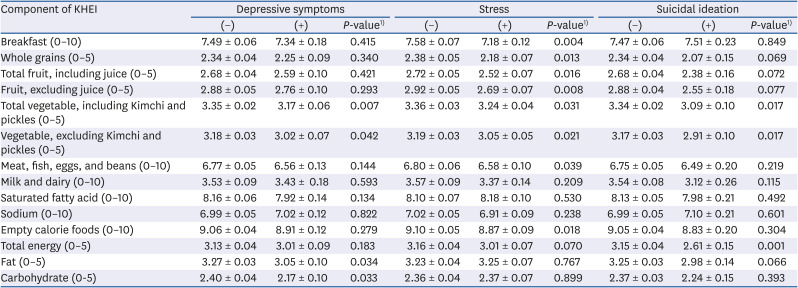
Table 2
Differences in the component of KHEI among men by psychological distress
All values are presented as means ± SE.
KHEI, Korean healthy eating index.
1)P-values are derived using survey linear regression analysis.
![]()
Table 3
Differences in the component of the KHEI among women by psychological distress
All values are presented as means ± SE.
KHEI, Korean healthy eating index.
1)Mean differences between groups were tested using a survey linear regression analysis.
![]()
Odds ratios (ORs) for psychological distress according to the quartiles of the KHEI score and gender
Table 4 presents the adjusted ORs and 95% confidence interval (CI) for depressive symptoms, stress perception, and suicidal ideation from multiple logistic regression analyses according to the quartiles of the KHEI scores. The multivariate-adjusted ORs for depressive symptoms, stress perception, and suicidal ideation in women with the highest quartile of KHEI scores compared to the lowest quartile were 0.69 (95% CI, 0.51–0.92), 0.73 (0.58–0.82), and 0.52 (0.33–0.82), respectively, and significant dose-response associations were observed (P for trend < 0.05 for all). On the other hand, these associations were not observed in men after adjusting for the confounding variables (all P for trend > 0.05).
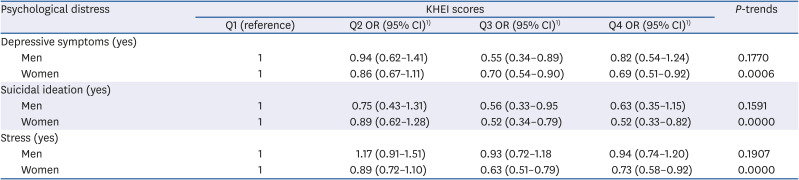
Table 4
Association between psychological distress and the adherence to the KHEI
Cutoff values for quartiles of KHEI are as follows: for men Q1, 17.6–54.2; Q2, 54.3–63.4; Q3, 63.5–71.6; and Q4, 71.7–99.1; for women Q1, 19.6–56.8; Q2, 56.9–66.0; Q3, 66.1–74.8; and Q4, 74.9–99.6.
KHEI, Korean healthy eating index; OR, odds ratio; CI, confidence interval.
1)ORs and 95% CIs were obtained from a survey logistic regression analysis adjusted for age (continuous), body mass index (continuous), family income level (< 100 × 104, 100–199 × 104, 200–299 × 104, 300–399 × 104, 400–499 × 104, and ≥ 500 × 104 won/month), smoking status (current smoker, ex-smoker, and never smoker), daily alcohol intake (none, 1–14.9, 15–29.9, and ≥30 g/day), total weekly physical activity, total daily energy intake (kcal/day), spouse (yes or no), type 2 diabetes (yes or no), hypertension (yes or no), and hypercholesterolemia (yes or no).
![]()
Go to :
DISCUSSION
This study indicated that poor diet quality was associated with psychological distress, e.g., depressive symptoms, stress perception, and suicidal ideation. Moreover, this association was more prominent in women. Men showed an inverse relationship between psychosocial distress and KHEI, but this association disappeared when adjusting for confounders. Most results of the association between depression [121314151617] or stress [181920] and diet quality did not show a gender difference. On the other hand, the longitudinal study by Elstgeest et al. [21] revealed a significant interaction of depressive symptoms and sex for HEI. Depressive symptoms were associated with a lower alternative HEI (AHEI) score in men but not in women, which was in contrast to the present result.
Unlike women, men with psychological distress were more likely to be related to other lifestyle factors, such as alcohol consumption, smoking, and physical activity, than a diet [222324]. Subgroup analysis was performed using the interaction terms to determine if smoking, alcohol consumption, and exercise affect the relationship between psychological distress and HEI (not shown in table). Smoking, alcohol consumption, and physical activity did not significantly modify the observed association between psychological distress and KHEI scores (P-interaction > 0.074 for all).
Relatively little research has been performed on the relationship between suicide and diet quality and certain types of food [2526272829]. Unlike the research results, a Dutch study reported that suicidal thoughts had no association with the diet quality using an AHEI 2010 [25]. A large population-based study in Japan suggested a prudent dietary pattern might be associated with a decreased risk of death from suicide in both men and women [27]. In contrast, a case-control study by Perera et al. [29] found that certain dietary food groups demonstrated no significant association with a history of attempted suicide. Their results are difficult to compare directly with the current results because the study population and target outcomes were different.
The present study reported a difference in adherence to specific dietary components of the KHEI between sexes. Men experiencing depressive symptoms were less likely to eat meat, fish, eggs, and beans, while depressed women showed a lower vegetable intake. Both men and women with suicidal ideation showed a lower intake of vegetables. A systematic review by Głąbska et al. [30] reported that a high total intake of fruits and vegetables might protect against depressive symptoms. In the present study, however, fruit consumption was not associated with depressive symptoms and suicidal ideation. A recent randomized controlled trial [31] showed that a 3-week simple dietary intervention that emphasizes lean meat, fish, and fresh fruits and vegetables appears to improve depressive symptoms. Further study will be needed to identify whether a healthy diet high in vegetables and lean meat can improve depressive symptoms in Koreans.
Previous studies reported that women with chronic stress were more likely to exhibit unhealthy dietary behaviors [181932]. The current study reported that the quality of specific components of the diet, such as whole grains, sweets and beverages, fruit and vegetables, might be particularly impacted among women experiencing stress. These findings support previous studies reporting a high intake of processed foods and sugar are associated with perceived stress [333435]. Among the components of KHEI, breakfast skipping was associated with stress in both men and women. This is in accordance with previous studies [203637]. Widaman et al. [20] showed that habitual breakfast skippers with stress were likely to eat a higher intake of added sugars in the evening. In the present study, only women with stress consumed more added sugars.
The results of this study showed that diet is an important component of mental health. On the other hand, it is unclear if a poor diet is a consequence of depression or depression is the cause of poor intake. The NutriNet Santé cohort study [38] that included 26,225 participants (aged 18–86 years) initially free of depressive symptoms showed that high adherence to nutritional recommendations is associated with a reduced risk of incident depressive symptoms. The SUN cohort study [14] also showed an inverse and significant association between the AHEI-2010 and depression risk. The risk of depression was decreased by 40% in the extreme quintiles (fifth vs. first) of AHEI-2010. In a recent meta-analysis of 24 prospective cohort studies, adherence to a high-quality diet was significantly associated with a lower risk of developing depressive symptoms (ORs ranged 0.64–0.78 in a linear dose-response fashion [P < 0.01]) [39]. On the other hand, these results do not mean that unhealthy diet patterns are associated with an increased risk of depression.
A recent randomized controlled trial [40] showed that in patients with depression, a 12-week healthy diet intervention resulted in a significant decrease in depression symptoms. In the other RCT by Francis et al. [31], a 3-week brief diet intervention could reduce the symptoms of depression, anxiety, and stress in young adults. Few intervention studies confirmed whether diet remediated the stress symptoms or suicidal thoughts. Moreover, observational studies of stress and suicidal thoughts have not been established as studies regarding depression. Nevertheless, current evidence, including the present results, suggest that nutrition psychiatry is a field of research worth pursuing. Future studies should identify mechanisms linking depression, stress, suicidal thoughts to diet quality and determine if diet therapy can improve mental health.
This study had some limitations. First, the current study was a cross-sectional design without evidence of a temporal relationship between exposure and result, so a causal relationship between HEI and psychological distress cannot be inferred. Second, in this study, depressive symptoms and suicidal ideation were evaluated in response to one simple question. An important consideration is whether these questions accurately assessed the presence of depression and suicide attempts. These 2 items were proven through previous studies as a well-documented predictor of depression and suicidal attempts [4142]. Further research using more accurate evaluation tools for psychological distress will be needed to add more evidence to the relationship observed in this study. Third, the residual confounding variables, such as disability, adverse life events, personality traits, and social support, which could affect psychological distress, cannot be excluded. On the other hand, this study finely adjusted the potential confounding factors for psychological distress with detailed information on the sociodemographic characteristics and lifestyle factors.
Despite these limitations, this study has several strengths. This is the first study to identify an association of dietary quality with psychological distress using KHEI among a nationally representative sample of Koreans. A previous study used the recommended food score, which was calculated based on the reported consumption of foods that contain antioxidant nutrients, so there was a limitation in evaluating the overall dietary quality, including the total intake or intake of nutrients [43].
Poor adherence to dietary recommendations was associated with psychological distress, particularly in women. Although additional research will be needed to determine the effects of diet management on the relief of depression and stress symptoms, this study suggests a direction for diet management in patients with depression, stress, and suicidal thoughts.
Go to :
 XML Download
XML Download