

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The emerging obesity prevalence in developing countries worldwide is alarming, including that in Korea. In 2016, 40% of women aged 18 years and above were overweight and 15% of women were obese worldwide [1]. According to the National Center for Health Statistics reports, the age-adjusted prevalence of severe obesity among adults represented 6.9% of men and 11.5% of women [2]. The prevalence of overweight and obesity was similar in men and women, whereas the prevalence of severely obese women was approximately twice as high as that of men. The increasing rate of overweight and obesity in Korea, as well as Western societies, results in a serious public health problem. The prevalence of obesity has rapidly increased between 1998 (26.0%) and 2018 (34.6%) in Korean adults. The prevalence of obesity remained relatively stable from 25.2% in 2008 to 25.5% in 2018 for women, while the prevalence in men sharply increased from 2005 (35.3%) to 2018 (42.8%) [3]. Despite the stable findings on the overall prevalence rate of obesity in Korean women, a consistent increase in morbid obesity (body mass index [BMI] ≥ 30.0 kg/m2) from 3.5% in 2008 to 4.9% in 2018 has been recorded [34].
Increased prevalence of obesity leads to a wide spectrum of diseases, including hyperlipidemia, metabolic syndrome, hypertension (HTN), cardiovascular diseases, type 2 diabetes mellitus (T2DM), cancer, and depression, without specific symptoms [56]. By losing approximately 5–10% of body weight, HTN, insulin resistance, the risk of osteoarthritis, cancers, and other hazards for chronic diseases can be significantly improved [78]. In 2019, the incidence rates of T2DM, HTN, myocardial infarction, and stroke consistently increased as BMI increased between ages 20–39 years in Koreans [5]. Seo et al. [5] also reported that T2DM, HTN, and hyperlipidemia were significantly higher in individuals with BMI ≥ 25 kg/m2. Additionally, the detrimental consequences of being obese have been found to be especially harmful in women, elevating risks for mental health conditions, polycystic ovary syndrome, endometriosis, and cancer, including endometrial and breast cancer [91011]. Therefore, it is important to prevent and manage obesity.
The final goal of obesity treatment is to achieve and maintain an ideal body weight (IBW). There are several methods that have been used to treat obesity, such as lifestyle modifications (diet and behavior), exercise, medications, endoscopic procedures, and surgery [12]. Diet and behavior modification and exercise are conventional treatment methods, but many studies reported that lifestyle modifications might fail at sustaining weight loss [131415]. Some researchers also suggest that traditional therapy is not very effective in T2DM patients with severe obesity [16]. Diet and behavior modifications as well as exercise, with or without medication, is the best initial treatment method; however, methods such as bariatric surgery or endoscopic procedures are needed for individuals with severe obesity [17]. Bariatric surgery, including gastric bypass (GBP), adjustable gastric band, sleeve gastrectomy, and duodenal switch, has been reported to be effective in the long term for weight loss. Despite these advantages, surgery should be considered only for patients with BMI ≥ 35 kg/m2 who have failed nonsurgical methods (with or without medications) and who have obesity-related complications. Further, bariatric surgery has limitations: it is an expensive and invasive procedure and may cause serious complications such as nutritional shortages, gallstones, ulceration, and hernias [18].
Intragastric balloons (IGBs), which are a form of nonsurgical therapy, are designed for weight loss and have minimal side effects compared with bariatric surgery [19]. The Garren-Edwards Gastric Bubble was the first US Food and Drug Administration-approved IGB in 1985 [20]. IGBs that were more effective in promoting weight loss have consistently been developed over the last 20 years. Typically, an IGB is filled with air or saline solution of 400–700 mL and placed in the stomach to occupy space and reduce gastric capacity, resulting in weight loss [21]. The most common complications of IGBs include vomiting, nausea, and a treatment duration of 6 mon; however, treatment side effects are minimal compared with those of bariatric surgery. The End-Ball®, approved by the Ministry of Food and Drug Safety, and the most generally used IGB treatment in Korea, is made of smooth spherical elastic polyurethane [22].
IGB could play a beneficial role in reducing obesity by reducing stomach volume with minimal side effects compared with surgery. However, the beneficial effects of IGB in Korean women have not been fully investigated. Therefore, this study aimed to evaluate the effects of IGB treatment for 6 mon on obesity in Korean women.
Go to : 
SUBJECTS AND METHODS
Subjects and study design
This clinical study was a retrospective study, using subjects' medical records. We analyzed data from 74 female patients with obesity (BMI ≥ 25 kg/m2) who received IGB treatment. The study included data collected during the period from February 2016 to July 2017. Data retrieved from subjects' medical records included information on age, sex, weight, height, body composition, comorbidities with obesity, and health-related behaviors. We analyzed their medical records before IGB and 6 mon after IGB. Subjects who had a BMI of < 25 kg/m2, were under 18 years of age, were males, or had no medical records before and after IGB were excluded from the study. Power calculations to determine the required sample size were performed with GPower (version 3.1.) using an alpha value of 0.05 and a power of 95%. This retrospective medical record review was approved by Changwon National University's Institutional Review Board (IRB) (IRB No. 1040271-201711-HR-030). Patients' medical records were analyzed before IGB and at 1, 3, and 6 mon after IGB treatment.
Anthropometric analysis
Anthropometric measurements were obtained from all subjects. Height and weight were measured with a digital scale. BMI was calculated by dividing the subject's weight (kg) by the square of the subject's height (m2). Body fat mass (BFM; kg), percent body fat (PBF; %), and skeletal muscle mass (SMM; kg) were measured using bioimpedance analysis (InBody 3.0; Biospace, Seoul, Korea). Waist circumference (WC) and hip circumference (HC) were measured with a flexible and substantial tape. Waist-to-hip ratio (WHR) was calculated as the WC divided by HC. Anthropometric measurements and body composition data were measured before and 1, 3, and 6 mon after IGB treatment. Percentage of excess weight loss (%EWL) was generally calculated using the formula: %EWL = (preoperative weight – initial weight) ÷ (initial weight − IBW) ×100.
General characteristics, health-related lifestyle, and experience of nonsurgical treatments
For all the subjects, general characteristics, lifestyle, and experience of nonsurgical treatments were analyzed using questionnaires and medical interviews. The general characteristics of age (20–29, 30–39, 40–49, or ≥ 50 years), marital status (married/unmarried), and occupation (manual worker, office clerk, student, or unemployed) were assessed. The health-related lifestyles were categorized as follows: alcohol consumption (yes, no), smoking status (yes, no), and complication-related obesity (osteoarthropathy, women-specific diseases, sleep disturbance, diabetes, psychical disorder, HTN, asthma, fatty liver, and others). Nonsurgical treatments were classified as diet therapy, exercise, behavior modification, pharmacotherapy, and others.
Eating habits questionnaire
The eating habit section was designed to investigate dietary patterns related to meal frequency (irregular, once, 2 times, or 3 times per day), meal time (fixed time, sometimes irregular, or irregular), meal speed (> 20, 10–20, or within 10 min), and overeating (≤ 1 time, 2–3 times, or ≥ 4 times per week). The eating habits questionnaires were administered to the subjects once during the study, and subjects were asked about their dietary behaviors.
Statistical analysis
All data are represented as means ± SD, and the statistical significance was set at P < 0.05. The data from the questionnaire surveys were compared using the χ2 test. In addition, the changes in weight and body composition determined before and at 1, 3, and 6 mon after IGB treatment were analyzed using a 1-way repeated measures analysis of variance. The collected data were analyzed using IBM SPSS Statistics version 24 software package (IBM Corp., Armonk, NY, USA).
Go to :
RESULTS
General characteristics
A total of 74 subjects were enrolled in this study; their general and health-related lifestyle characteristics at baseline are shown in Table 1. The mean age was 34.7 years. The mean BMI was 31.0 ± 4.2 kg/m2. A total of 43.2% of the subjects had age and BMI within 30–39 years and 25–30 kg/m2, respectively. Among the subjects, 32 (43.2%), 28 (37.8%), and 14 (18.9%) met the BMI criteria for obesity, severe obesity, and morbid obesity, respectively. Subjects who reported as unmarried constituted 63.5% of the sample, and most subjects (72.5%) were office clerks. Regarding alcohol consumption, 60.8% of the subjects responded “yes,” and 39.2% responded otherwise. The smoking response rate for “no” was 70.3%.
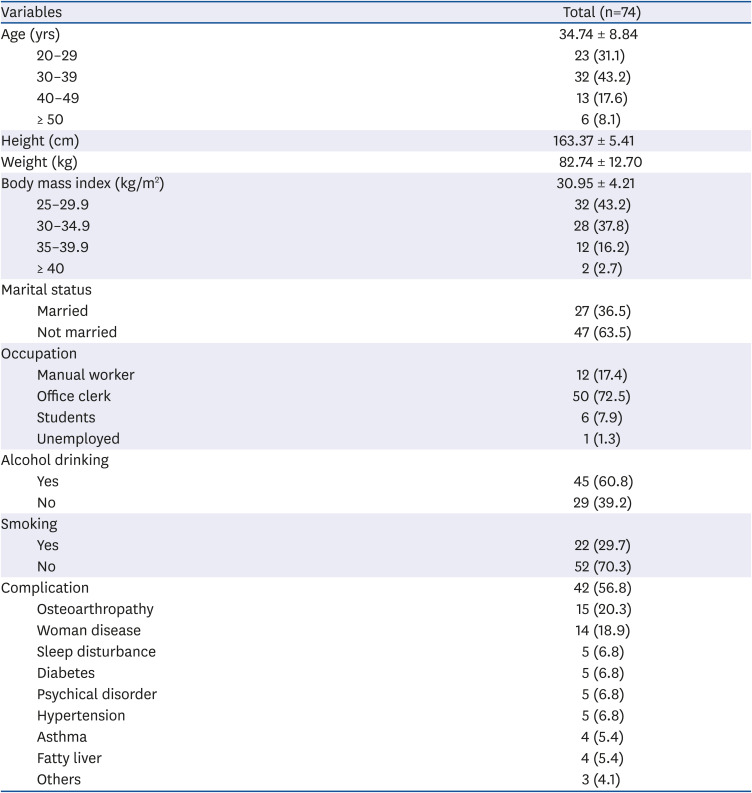
Table 1
General characteristics of the subjects at baseline
Values are presented as mean ± SD or number (%). The data from the questionnaire surveys were compared using the χ2 test.
![]()
Data on the subjects' experience of nonsurgical treatments at baseline are shown in Table 2. According to the questionnaire, 42 (56.8%) subjects had obesity-related complications. Osteoarthropathy (20.3%) and women-specific diseases (18.9%) were more frequently found in these subjects. Among the subjects with complications, 5% of the respondents indicated sleep disturbance, diabetes, psychical disorder, and HTN. Asthma, fatty liver, and others each accounted for 4% of the total responses. All subjects had tried nonsurgical therapy, such as pharmacotherapy (89.2%), exercise (85.1%), and diet modifications (71.6%, Table 2).
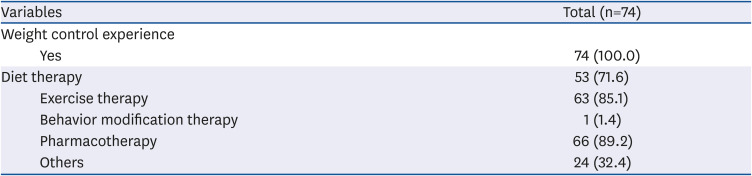
Table 2
Experience of nonsurgical treatments of the subjects at baseline
| Variables | Total (n=74) | |
|---|---|---|
| Weight control experience | ||
| Yes | 74 (100.0) | |
| Diet therapy | 53 (71.6) | |
| Exercise therapy | 63 (85.1) | |
| Behavior modification therapy | 1 (1.4) | |
| Pharmacotherapy | 66 (89.2) | |
| Others | 24 (32.4) | |
Values are presented as number (%). Multiple choices are available. The data from the questionnaire surveys were compared using the χ2 test.
![]()
Eating habits
Results about the eating habits of study subjects at baseline are shown in Table 3. Regarding the number of meals per day, 35.6% and 42.4% of the subjects reported “Irregular” and “2 times,” respectively. Only 20.3% had meals 3 times per day. Furthermore, the mealtime response rate for “irregular” was 49.3%, whereas 35.8% and 14.9% of subjects had “sometimes irregular” and “fixed” mealtimes, respectively. Most (46.5%) subjects finished their meals within 10 min, whereas 39.4% and 14.1% of the subjects finished their meals within 10–20 min and ≥ 20 min, respectively. Approximately 50% of the subjects reported overeating 2–3 times per week, and 44.8% overate ≥ 4 times per week. Thus, most subjects tended to eat at irregular times, ate fast (within 10 min), and overeat 2–3 times per week.
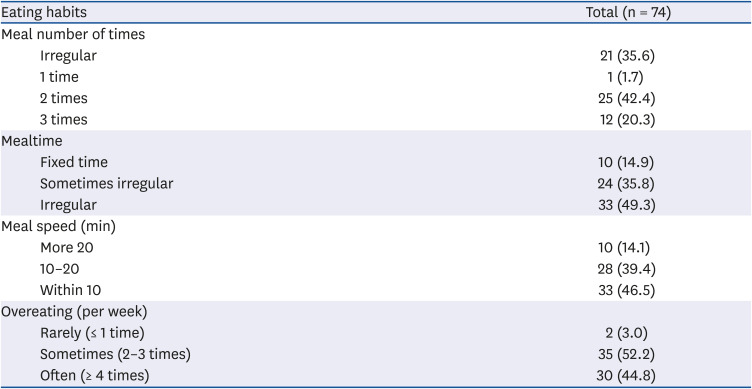
Table 3
Eating habits of subjects at baseline
Values are presented as number (%). The data from the questionnaire surveys were compared using the χ2 test.
![]()
Changes in body composition in subjects
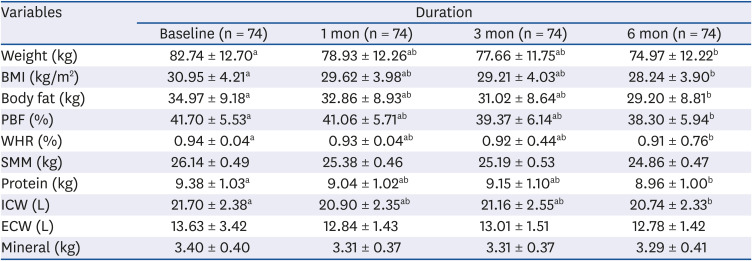
Body composition analyses before and after IGB are presented in Table 4. The results from anthropometrics indices before and after IGB showed significant reduction in body weight, BMI, BFM, PBF, and WHR at 6 mon after IGB treatment. There were no statistically significant differences in SMM and mineral contents after IGB treatment. The rate of weight loss, BFM loss, and WHR loss were 8.8%, 14.3%, and 2.6%, respectively, at 6 mon after IGB treatment. In particular, the decrease rate of the PBF was highest among the anthropometric measurements. The decreasing rate of PBF was significantly higher from 1 mon to 3 mon after IGB, whereas the decreasing rate of body weight and WHR were significantly higher from baseline to 1 mon after IGB (Fig. 1). Particularly, severely obese subjects (35 kg/m2 ≤ BMI < 40 kg/m2) showed greater weight loss (−11.7%, Fig. 2).
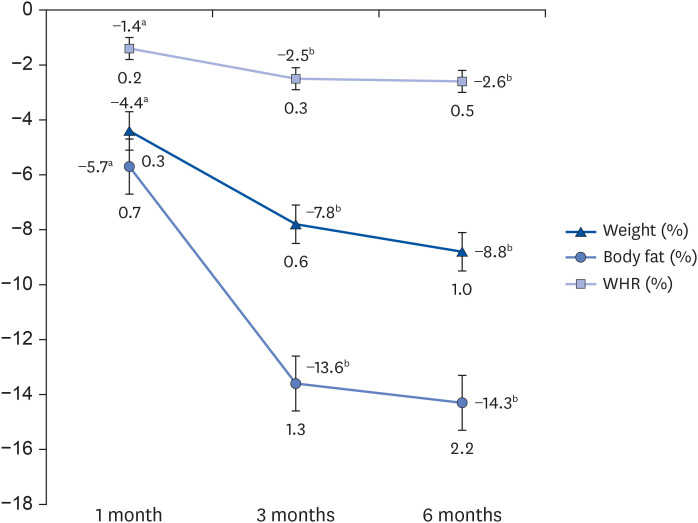 | Fig. 1Percentage changes in weight, body fat, and waist-hip ratio at 1, 3, and 6 mon after intragastric balloon treatment. All values are presented as mean ± SD, analyzed using repeated measures analysis of variance. Values in a line with different superscript letters are significantly different at P < 0.05.WHR, waist-hip ratio.
|
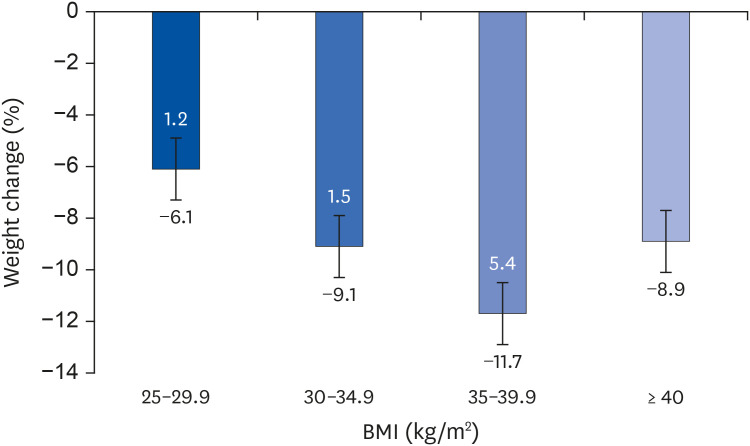
Table 4
Changes in body composition at baseline and after IGB treatment
All values are expressed as mean ± SD, analyzed using repeated measures analysis of variance. Means in the same row not sharing a common letter are significantly different at P < 0.05.
BMI, body mass index; PBF, percent body fat; WHR, waist-hip ratio; SMM, skeletal muscle mass; ICW, intracellular water; ECW, extracellular water.
![]()
Changes in body composition according to degree of obesity
Changes in BMI between baseline and after 6 mon in morbidly obese (BMI ≥ 30.0 kg/m2) subjects are presented in Table 5. The rate of morbidly obese subjects decreased after IGB treatment from 56.8% to 36.5%. The %EWL of morbidly obese subjects (BMI ≥ 30 kg/m2) was presented at 33.0 ± 28.4%.

Go to :
DISCUSSION
During the past few decades, the prevalence rates of obesity have been rapidly increasing worldwide, reaching a critical point. According to the World Health Organization, over 650 million (13%) of the world's adult population were obese in 2016 [1]. Thus, obesity has become a serious public health problem worldwide and can result in obesity-related diseases. We investigated the beneficial effects of IGB treatment on obesity in Korean women with obesity. Seventy-four women were recruited, and their general characteristics, eating habits, health related lifestyle, and body composition were analyzed.
Because of the analysis of general characteristics and health-related lifestyle factors, more than half of the subjects had one or more comorbidities, such as osteoarthropathy and woman’s disease. Osteoarthropathy is a syndrome that includes clubbing of the toes and fingers, periostitis of joint and long bones (radius, distal tibia, femur), and osteoarthritis [23]. Obesity is characterized by a systemic low-grade inflammatory status, leading to the development of metabolic diseases [24]. Obesity and pathogenesis of osteoarthropathy are not known; imbalanced adipokine expression leading to the remodeling and destruction of joint tissue has been reported [2526]. Reyes et al. [27] reported that as the BMI increased, the risk of knee osteoarthritis increased. Compared to normal weight, as the degree of obesity increased, the risk of irregular menstruation increased; at 20–24 years, the risks increased by 33.3%. BMI was also strongly associated with the risk of breast cancer among postmenopausal women. Maternal complications with increase in BMI in women [28]. Our results are in line with those of previous studies that showed that increase in obesity greatly elevated the risk of obesity-related complications [2930]. Thus, weight loss after IGB treatment is thought to effectively alleviate obesity, suggesting an improvement in osteoarthritis and women's disease. Crea et al. [29] reported that the incidence of T2DM, hypertriglyceridemia, hypercholesterolemia, and HTN at 1 year of follow-up after IGB was significantly lower than before IGB. Another previous study found that diastolic blood pressure significantly decreased after IGB removal [30]. Similar improvements in fasting blood glucose, total cholesterol, triglyceride (TG), C-reactive protein, and hemoglobin A1C (HbA1c) levels were also found in other studies of IGB in addition to significantly increased quality of life as compared to baseline [31]. Therefore, IGB treatment may be effective in improving the comorbidities of obesity, including metabolic syndrome.
The lack of exercise, sedentary lifestyle, and unhealthy eating habits are reported as the main causes of excess body fat accumulation [3233]. In a study by Hassan et al. [32], most obese and overweight Egyptian women, were engaged in health risk behaviors and unhealthy dietary patterns (the low intake of fruits, vegetables, and milk, the increasing consumption of snacks, sweets, salts, and soft drinks). Korean children in the overweight group were also significantly more likely to overeat and ate rapidly compared with the normal group [33]. In a study by Kang et al. [34], regarding the eating habits, high response rates for “Consumed meal quickly (< 10 min),” “Preference of oily foods”, and “A tendency to eat until the stomach is full” were observed in metabolically abnormal, obese women. Our study also showed that most obese subjects had negative eating habits, including eating at irregular times, eating fast (within 10 min), and overeating frequently (2–3 times per week), which was consistent with previous studies [20323334].
IGB with a volume of 400 mL or greater may also lead to feelings of satiety by delaying gastric emptying and finally reducing their food intake [21]. Additionally, evidence suggests that IGB suppresses food intake through the vagal signaling by modulated gastric mechanoreceptors [35]. The Bioenteric intragastric balloon (BIB), also known as ORBERA, has been most widely used in IGB treatment. BIB is made of silicone, which is thicker than polyethylene, and the balloon volume is, thus, significantly bigger and has a high incidence of complications [36]. Buzga et al. [36] reported a mean weight loss of 13.9 kg with a %EWL of 37.9% in 20 patients in 6 mon after End-Ball treatment. Keren and Rainis [37] reported a mean weight loss of 23.5 kg and a %EWL of 39.2% in 114 subjects who were treated with the End-Ball; the weight loss significantly continued for 1 year after End-Ball removal. Some researchers suggested classifying the outcome of IGB into three categories based on the %EWL: %EWL < 20, unsatisfying outcome; %EWL of 20–50, good outcome; and %EWL > 50, very good outcome [3839]. In this study, we also found that body weight, body fat, and WHR significantly decreased at 6 mon after IGB treatment. In particular, patients with morbid obesity (BMI ≥ 30 kg/m2) showed a mean %EWL of 33.0%.
The results of this study also showed that SMM and mineral contents were not significantly different after IGB treatment with adverse reduction in BFM. Obesity is negatively associated with muscle mass, which detrimentally affects muscle function. Obesity may induce an increase in intramuscular adipose tissue resulting in impaired muscle strength and mobility [40]. Reduced muscle function is a crucial predictor of serious problems, including the restriction of physical activity, mobility disability, hip fracture, falls, and increased mortality rate [41]. Thus, subjects with obesity also tended to have an increased risk of fracture in peripheral sites [40]. Bone mineral loss can accelerate the risk of hip fracture and osteoporosis in women. Nevertheless, excessive weight loss can also add to the increasing risk of fracture by inducing muscle mass loss and imbalance in bone metabolism [42]. Thus, maintenance of muscle and bone mineral should be the focus of therapeutic strategies for obesity. Previous studies have reported that bone mineral contents significantly decreased after bariatric surgery. Bone mineral density (BMD) at the hip tended to decline to an extent of 1 year after GBP [43]. Carrasco et al. [44] reported that GBP results in a significant loss in BMD with changes in body composition in women with obesity. Therefore, IGB, which has fewer side effects, muscle mass loss, and mineral reduction, is considered to play a key role in obesity treatment as compared with pharmacotherapy and surgery, especially in patients with mild to moderate obesity who failed previous treatment methods.
However, this study had some limitations. First, we did not investigate the improvement of obesity-related complications after IGB and metabolic parameters before and after IGB. Therefore, we could not assess how IGB helps with the improvement of metabolic status related obesity, maintenance of SMM, and bone mineral with sustained weight loss in subjects with obesity. Second, the time of exercise or physical activity on weekends was not included in the questionnaire survey. Third, we did not investigate the eating habits and health-related lifestyles of subjects after IGB. Fourth, we did not investigate the side effects of IGB. IGB may result in a few side effects such as nausea, heart burn, and gastric ulcers with bleeding and erosions [30]. However, IGB is reported to have a lower risk of complications than bariatric surgery.
Of the patients with bariatric surgery, 20-30% do not achieve weight loss [4546]. Approximately 20-25% of patients undergoing bariatric surgery can also achieve weight loss over a period of 10 years [46]. Although IGB has also been shown to be effective in achieving weight loss, only 22% of the patients with IGB maintained the weight loss in relation to their initial weight at the end of IGB removal [34]. Crea et al. [29] reported that weight regain generally presented during follow-up after IGB removal. Thus, weight regain remains a risk for all severely obese patients after IGB and bariatric surgery.
Maekawa et al. [47] investigated the effectiveness of combining a low-carbohydrate diet (< 120 g carbohydrate/day) versus a calorie-restricted diet (IBW × 25) with IGB treatment. At 1 year after IGB, the %EWL of both groups were shown as 49.9 ± 60.0 and 33.1 ± 27.0, respectively, showing an excellent weight loss effect. The TG, high-density lipoprotein cholesterol, saturated fatty acid, and HbA1c levels of the low-carbohydrate diet group were significantly decreased lower than before IGB. Weight regain was also significantly lower in the low-carbohydrate diet group than in the calorie-restricted diet group. Thus, dietary modulation is essential for preventing weight regain, and carbohydrate restriction is considered to be more effective in maintaining weight loss after IGB.
Papalazarou et al. [48] reported that the effect of weight loss varies according to eating habit modification and physical activity, even though patients would have undergone the same surgery for obesity. Subjects who are extremely obese have been reported to have poor eating habits, such as frequent (4 days or more per week) consumption of high-fat and sweet foods/drinks like hamburgers, sausages, chocolate, soft drinks, and ice cream before surgery [49]. Therefore, to increase weight loss after IGB treatment, it is necessary to correct bad eating habits before IGB treatment, and for this, continuous diet and health-related lifestyle modifications along with education on nutrition is required.
In conclusion, most Korean women with obesity had comorbidities related with obesity, such as osteoarthropathy and woman’s disease, and had negative eating habits. Additionally, IGB can be of beneficial effect in ameliorating obesity without adversely decreasing SMM and bone mineral. We suggest that further studies be conducted to evaluate the changes in eating habits and metabolic and inflammatory biomarkers in Korean women with obesity who have received IGB treatment.
Go to :
 XML Download
XML Download