

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Menopause is a physiological state in which estrogen secretion is reduced due to ovarian failure, resulting in the termination of ovulatory cycles and the permanent cessation of menstruation [1]. During this period, women may experience certain health problems, such as facial flushing, chills, headaches, memory loss, depression, and arthralgia [23]. These symptoms may lead to a depressed mood or clinical depression [4]. Indeed, the prevalence of depression during menopause is 2-fold higher than that in the premenopausal state [5]. Depression is a mood disorder caused by complex interactions between physical, psychological, and situational factors.
Recent studies have reported that dietary omega-3 fatty acids may play a role in depression [6]. A meta-analysis including nine cross-sectional and seven cohorts showed a significantly decreased risk of depression with increased levels of omega-3 fatty acids [7]. In addition, a pooled analysis of nine clinical trials conducted in China, Europe, and the United States on adults aged 60 years and older consistently showed that the symptoms of depression were significantly lower in individuals who were taking omega-3 fatty acid supplements at doses of more than 1.5 g/day [8]. However, few studies have analyzed the association between dietary omega-3 fatty acids and depression in postmenopausal Korean women.
Omega-3 fatty acids may play a major role in preventing depression as the metabolites of omega-3 fatty acids can exert anti-inflammatory action and have a protective effect against depression by increasing the serotonin levels [9]. Indeed, postmenopausal women who have deficient levels of estrogen tend to be at a greater risk of depressive disorders and mood symptoms [101112]. Estrogen plays a critical role in promoting the growth and survival of neurons [13] and the prefrontal cortex [14] and is involved in the serotonergic system in several brain areas [15]. Since estrogen can stimulate the conversion of essential fatty acids into long-chain metabolites [16], an estrogen-deficit-associated omega-3 fatty acid deficiency may exacerbate the risks of depression. Therefore, it is important to determine whether omega-3 fatty acids can be an alternative therapy (with other cardiometabolic health benefits) for postmenopausal women, who are at a higher risk of depression.
Previous studies that investigated the role of omega-3 fatty acids in depression among postmenopausal women were mostly clinical studies reported from the United States and Iran [1718] and only scant epidemiologic data are available for Korean postmenopausal women [1920]. Previous Korean studies did not consider the possible errors in the measurement of dietary assessments (for instance, participants with implausible total energy intake were not screened) or dose-response relationships on menopause. Therefore, it is pertinent to investigate whether a higher intake of omega-3 fatty acids is associated with lower rates of depression in a dose-dependent manner, considering various potential confounding factors and measurement errors in Korean postmenopausal women who are at a high risk of depression due to menopause and the presence of climacteric symptoms.
The purpose of this study was to analyze the association between dietary omega-3 fatty acid intake and depression and to determine the dose-response patterns in postmenopausal women using representative data from the Korean population.
Go to : 
SUBJECTS AND METHODS
Study population
The Korea National Health and Nutrition Examination Survey (KNHANES) is a cross-sectional nationwide health and nutrition survey of non-institutionalized Korean individuals aged over 1 year and residing in South Korea. To facilitate the representability of the sample and accuracy of the estimation, a complex sampling method of two-stage stratified cluster sampling was used. The detailed KNHANES survey methods and protocols have been described elsewhere [21]. Briefly, various demographic, lifestyle, dietary, and health-related data were obtained through health interviews, health examinations, and nutrition surveys. KNHANES was first started in 1998 and was conducted every 3–4 years in the early part of its history. The rolling sample survey method was implemented subsequently and has been conducted every year since 2007. This study used the data from KNHANES VI, the most recently completed survey period; the dietary omega-3 fatty acid intake variable was available at the time of analysis.
For the purposes of this study, both natural and artificial menopause were categorized as menopause; this was based on amenorrhea or menstruation-related items in the women's health questionnaire. A total of 22,948 respondents were registered in KNHANES VI (2013–2015). Individuals who met the following criteria were excluded from the analysis: 1) men (n = 10,599), 2) pregnant, lactating, or premenopausal women (n = 7,818), 3) women with a total energy intake of less than 500 kcal or more than 5,000 kcal per day [22] (n = 380), and 4) women with no data on depression (n = 1). Finally, 4,150 postmenopausal women were included in the analysis. The study followed the guidelines of the Declaration of Helsinki. All participants signed an informed consent form, and the study was approved by the Institutional Review Board of the Korea Centers for Disease Control and Prevention (approval No. 2013-07CON-03-4C, 2013-12EXP-03-5C).
Demographic and lifestyle information
The demographic, lifestyle, and health information were collected using self-reported questionnaires. The household income levels were classified into four categories: low, mid-low, mid-high, and high. Education levels were categorized as less than high school graduation and high school graduation or higher. The body mass index (BMI) was calculated and categorized based on the BMI criteria of the World Health Organization for Asian populations: normal or less (< 23 kg/m2) and overweight or obesity (≥ 23 kg/m2) [23]. Based on their smoking and drinking status, they were classified as smokers or non-smokers and drinkers or non-drinkers, respectively. The metabolic equivalents of task (METs-h/week) [24] were calculated as the weekly physical activity time and through the application of weights by exercise intensity. The survey data on the days and hours spent performing intense/moderate/walking physical activity were obtained, and a weight value according to each exercise intensity was applied. In the 2014 and 2015 surveys, high- and moderate-intensity physical activities were further categorized into work and leisure activities, and the average value of each item was used to calculate the METs-h/week. The calculated values of METs-h/week were classified into tertiles for the analysis. The responses for the use of unspecified dietary supplements were classified as “yes” or “no”.
Dietary assessment
The dietary information was obtained using a 24-h recall method, which contains information regarding every consumed food item, in addition to the meal times, places of eating, and the quantity of food consumed during the 24 h before the survey. Assisting aids were used to enhance the validity of the recall data. These data were converted to individual foods using the food recipe database developed by the Korea Health Industry Development Institute [25], and the nutrient intake was calculated using the food composition table published by the Rural Development Administration [26]. In this study, we used the daily energy intake (kcal) and dietary omega-3 fatty acid intake (g) as variables for the analysis. The first dietary fatty acid database was established using 24-h recall data from the KNHANES VI-1(2013) [27] and has been updated thereafter [28]. The fatty acid levels of foods were obtained from the food composition tables of national institutions (Rural Development Administration, National Fisheries Research & Development Institute) [2930], the US Department of Agriculture [31], and the Japan Ministry of Education, Culture, Sports, Science, and Technology [32]. The detailed methods for developing the fatty acid composition table have been presented elsewhere [27].
Criteria for diagnosis of depression
Depression was defined based on the data obtained from a self-reported mental health questionnaire under the supervision of an investigator [33]. Depression was defined based on the following factors: 1) diagnosed with depression by a physician, 2) having depression currently, or 3) under treatment for depression. Those who provided a response of “yes” for any of these questions were included in the depression group.
Statistical analysis
The analysis of this study was conducted considering the sampling weight, stratification variables, and cluster variables related to the complex sampling of the KNHANES [21]. The participants were divided into quintiles according to the intake levels of dietary omega-3 fatty acids. To compare the general characteristics between groups, the chi-square test and general linear regression analysis were used for categorical and continuous variables, respectively. The residual adjustment method was used to calculate the levels of energy-adjusted nutritional intake [34]. Multivariate logistic regression analysis was performed to calculate the odds ratios (ORs) and their 95% confidence intervals (CIs). The potential confounding factors and effect modifiers that could affect the association between the dietary omega-3 fatty acid intake levels and depression in the analysis were selected based on a review of the literature [7193536] and preliminary analysis, determining whether key demographic, lifestyle, or dietary variables were associated with omega-3 fatty acid intake and depression and whether the identified potential confounding variables were not on the causal pathway between omega-3 fatty acid intake and depression in women.
The interactions were tested using multiplicative terms in logistic regression models, and no significant interaction was found. The models, with step-by-step adjustment of confounding factors, were as follows: model 1, unadjusted; model 2, adjusted for age, household income, obesity status, education level, alcohol consumption, smoking status, physical activity, use of dietary supplements, energy-adjusted intake level of dietary fiber, and vitamin C. The P-value for the trend was calculated using the median of the quintiles of dietary omega-3 fatty acid intake as a continuous variable. The dose-response relationship between dietary omega-3 fatty acids and depression was examined semi-parametrically using restricted cubic splines with three knots, excluding values beyond the 5th and 95th percentiles. All analyses in this study were performed using the Statistical Analysis System (SAS version 9.4; SAS Institute, Cary, NC, USA). A significance level of α = 0.05, using two-tailed tests, was considered statistically significant.
Go to :
RESULTS
General characteristics of participants by intake levels of dietary omega-3 fatty acid
The 4,150 postmenopausal women were divided into quintiles according to their dietary omega-3 fatty acid intake. The median values for the 1st, 2nd, 3rd, 4th, and 5th quintiles were 0.3, 0.6, 0.9, 1.4, and 2.7 g/day, respectively; their general characteristics are presented in Table 1. A higher intake of dietary omega-3 fatty acid was observed among younger women (P < 0.001), alcohol drinkers (P = 0.01), and those with a higher level of education (P < 0.001), higher household income (P < 0.001), and higher physical activity level (P < 0.001), but no significant differences were observed in terms of obesity and smoking status.
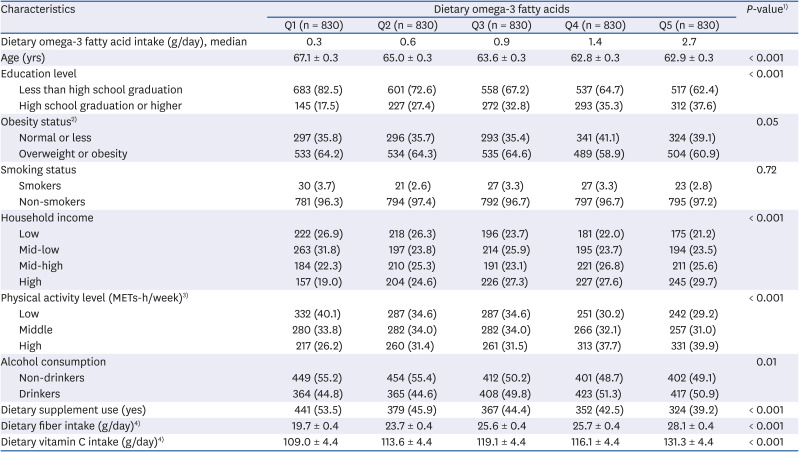
Table 1
Characteristics of postmenopausal women according to quintiles of energy-adjusted intake levels of dietary omega-3 fatty acid
Values are mean ± SE or number (%).
Q, quintile; METs, metabolic equivalents of tasks.1)
P-values were derived from the χ2 test for categorical variables and a general linear regression for continuous variables.
2)Obesity status was categorized as follows: normal or less < 23 kg/m2 and overweight or obesity ≥ 23 kg/m2.
3)Physical activity level was calculated as metabolic equivalent time hours per week (METs-h/week) and categorized into tertiles.
4)Values were adjusted for total energy intake.
![]()
Association between dietary omega-3 fatty acid intake and depression
The ORs of depression, according to quintiles of dietary omega-3 fatty acid intake, are shown in Table 2. In the unadjusted model (model 1), higher levels of dietary omega-3 fatty acid intake were associated with lower depression (P for trend = 0.02). After adjusting for multiple confounding variables (model 2), this inverse association remained significant (P for trend = 0.04). Compared to women in the lowest quintile of dietary omega-3 fatty acid intake, depression was 1.72-fold less likely in those in the highest quintile (OR, 0.52; 95% CI, 0.33–0.83; model 2).

Table 2
Odds ratio (95% confidence interval) for depression according to quintiles of energy-adjusted intake levels of dietary omega-3 fatty acid in postmenopausal women
Q, quintile.
1)P for trend across quintiles of dietary omega-3 fatty acids was calculated using a general linear regression.
2)Model 1: crude.
3)Model 2: adjusted for age, household income, obesity status, education level, alcohol consumption, smoking status, physical activity, use of dietary supplements, and energy-adjusted intake levels of dietary fiber and vitamin C.
![]()
Dose-response relationship between dietary omega-3 fatty acid intake and depression
Spline analysis suggested a monotonic dose-response relationship between dietary omega-3 fatty acid intake and depression (P for non-linearity=0.32; Fig. 1). Depression tended to decrease with an increase in dietary omega-3 fatty acid intake; however, further benefits were not evident as the intake of dietary omega-3 fatty acids increased beyond 1.8 g/day.
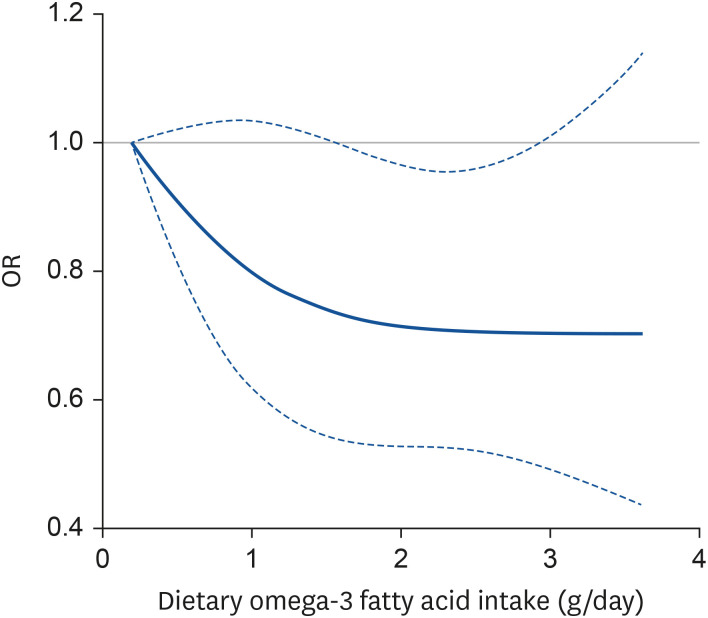 | Fig. 1ORs of the prevalence of depression by energy-adjusted intake levels of dietary omega-3 fatty acid via restricted cubic spline regression. Dashed lines represent the 95% confidence intervals. The models were adjusted for age, household income, obesity status, education level, alcohol consumption, smoking status, physical activity, use of dietary supplements, and energy-adjusted intake levels of dietary fiber and vitamin C (P for non-linearity = 0.32).OR, odds ratio.
|
Go to :
DISCUSSION
In this nationwide survey in Korea, postmenopausal women with a higher intake of dietary omega-3 fatty acids demonstrated a lower depression than their counterparts, and this association was linear. Omega-3 fatty acids play an important role in brain cell function by directly maintaining cell membrane fluidity in the central nervous system and by regulating ion channels and the cyclic adenosine monophosphate (cAMP) cascade [373839]. In particular, they impact the expression of brain-derived neurotrophic factor and cAMP response element-binding protein, which may lead to improved neurogenesis and neuroplasticity [384041]. Previous studies have also reported that the depletion of omega-3 fatty acids is associated with a lack of neuronal membrane stability, with decreased levels of serotonin, norepinephrine, and dopamine, suggesting lower cognitive function in depression [42].
In this study, depression was lower in postmenopausal women with higher dietary omega-3 fatty acid intake. This may be related to several mechanisms. Owing to the imbalance of eicosanoids, the rapid decrease in estrogen during menopause increases the levels of prostaglandin E2 (PGE2), an inflammation-promoting factor [394344]. This subsequently induces sickness behavior and affects neuronal function, causing cognitive and impulse control disorders [42]. Indeed, a significant association was observed between inflammatory markers and depression in adults in the Netherlands; those with higher levels of inflammatory biomarkers, such as interleukin-6, had increased risks of major depressive disorders [45]. Omega-3 fatty acids act as estrogens, inhibiting the production of PGE2, which is an eicosanoid that consequently inhibits the production of inflammatory cytokines [3946]. In an animal study, lifetime exposure to omega -3 polyunsaturated fatty acid (PUFA)-rich diets restored the Aβ-induced depressive-like profile [47]. Therefore, the intake of omega-3 fatty acids is believed to have a beneficial effect on depression in postmenopausal women; it relieves the hypersensitive immune system and has an anti-inflammatory effect [48].
A meta-analysis including nine cross-sectional and seven cohort studies reported that a high dietary omega-3 fatty acid intake decreases the risk of depression with a J-shaped association [7]. When divided by study design, depression was 21% lower in cross-sectional studies and 15% decreased in cohort studies [7]. This study explained that there was a high variation in intake levels in the Japanese population due to the very high intake of omega-3 PUFAs. A recent Japanese cohort study published after this meta-analysis also confirmed that Japanese adults with high omega-3 fatty acid intake had a low risk of depressive symptoms [49]. A recent meta-analysis of 12 randomized controlled trials demonstrated that supplementary intake of eicosapentaenoic acid (EPA)-pure (= 100% EPA) and EPA-major formulations (≥ 60% EPA) conferred clinical benefits for depression [50]. However, no benefits were found with supplements containing docosahexaenoic acid (DHA)-pure and DHA-major formulations. However, a recent multi-national multi-disciplinary Delphi study for the application of omega-3 PUFAs in the treatment of major depressive disorders found that current evidence is insufficient to conclude that “omega-3 PUFAs are one of the potential monotherapies for adult major depressive disorder” [51].
The average intake level of omega-3 fatty acids in these postmenopausal women was 1.31 g/day, which seemed to be slightly lower than that in premenopausal women (1.46 g/day) and men (1.76 g/day) in the KNHANES. We observed a monotonic dose-response relationship between dietary omega-3 fatty acid intake and depression at these dietary intake levels; however, this decreasing trend became flatter at more than approximately 1.9 g/day of dietary omega-3 fatty acids. A similar pattern was observed in a pooled recent meta-analysis of nine cross-sectional and seven cohorts, showing a dose-response relationship with a peak decrease in depression risk at approximately 1.8 g/day of omega-3 fatty acids [7]. Although data regarding the effect of omega-3 fatty acids on depression may not be univocal, there is a general agreement on the fact that supplementation with omega-3 fatty acids is useful in improving depressive symptoms, especially in elderly women and that dosages of 2–4 g/day may provide the maximum benefit [17525354].
Our study has some limitations. Dietary information in this study may not have accurately reflected the usual dietary intake as it was calculated using a 1-day 24-h recall survey, and we could not exclude the possibility of reverse causality between the intake of dietary omega-3 fatty acid and depression in postmenopausal women in this cross-sectional study; two additional concerns are confounding and measurement errors. Although we selected potential confounding factors based on a review of the literature and preliminary analysis, we could not exclude the possibility of residual unknown or unmeasured confounding factors that may have affected these associations. For instance, the total antioxidant capacity, which may inhibit oxidative stress, may influence the association between omega-3 fatty acids and depression. In addition, we did not consider information on the use of hormone therapy because of the lack of data. This is because those with high intake of omega-3 fatty acids may tend to be health-conscious; therefore, they can, in addition, eat more fruits and vegetables, which are rich in antioxidants, and may be a protective dietary factor for depression [55]. In addition, there is the possibility of non-differential misclassification regarding the identification of depression, because we used self-reported information for diagnosing depression. Therefore, in addition to underestimation, overestimation may have occurred due to inaccuracies in the recognition of depression by physicians, recall errors by participants, or under-treatment of depression. To minimize this error and maximize the specificity of the case definition, we used a combination of responses on disease diagnosis or treatment taken. Despite these limitations, our results may be generalized to the Korean population as the KNHANES data are representative of this population. These findings suggest that omega-3 fatty acids may be an alternative therapeutic option for relieving depression in postmenopausal women. Since we investigated mental health during menopause, our findings also provide basic data on the prevention and management of health problems in women. Previous research in this area has largely been inadequate.
In conclusion, our findings suggest that a higher intake of dietary omega-3 fatty acids is associated with lower depression in Korean postmenopausal women. Large-scale prospective cohort studies of Korean women are warranted to verify this association, using omega-3 fatty acids in both dietary and supplement forms.
Go to :
 XML Download
XML Download