

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Atrial fibrillation (AF)-associated ischemic stroke poses significantly higher morbidity and mortality than strokes of vascular origin.1) Cardiac emboli originating from the left atrial appendage (LAA) are common causes of ischemic stroke in patients with AF,2) and are associated with more severe ischemic stroke and longer transient ischemic attacks (TIAs) than strokes secondary to atherosclerotic cerebrovascular disease.3) With the increased risk of arterial thromboembolism associated with AF, stroke prevention with oral anticoagulation (OAC) is the cornerstone of AF management.4) Non-vitamin K antagonist oral anticoagulants (NOACs) are often superior to vitamin K antagonists with respect to efficacy and safety, and exhibit more predictable pharmacodynamics and -kinetics, making them less susceptible to drug and food interactions and eliminating the need for regular blood monitoring.5) Given the safety issues of indefinite OAC use with either approach, LAA occlusion (LAAO) may be an alternative strategy for prevention of stroke, systemic embolization, bleeding, and death in AF patients taking OACs.6) Recent studies have reported less disabling and lethal strokes after percutaneous LAAO with the Amplatzer cardiac plug (ACP; Abbott Vascular, St. Paul, MN, USA) or Watchman device (Boston Scientific, Marlborough, MA, USA) than those in patients on warfarin therapy.7)8)9) However, no comparative data regarding ischemic cerebrovascular event-associated neurological outcomes following percutaneous LAA closure or NOAC treatment are available. This study investigated post-stroke neurological outcomes in non-valvular AF (NVAF) patients treated with LAAO, compared to those treated with NOAC therapy.
METHODS
Ethical statement
The study protocol adhered to the ethical guidelines of the 2013 Declaration of Helsinki. Use of all registry data was approved by the Institutional Review Board (Approval number: 4-2017-0343), which waived the requirement for informed consent.
Study population
We performed a multi-center, multi-national retrospective cohort study of ischemic stroke and TIA patients who underwent percutaneous LAAO or received NOACs before the index stroke. From the medical records of 1,427 consecutive patients in the Korean LAAO registry (May 2013 to January 2017), European ACP Multi-Center Registry (December 2008 to November 2013), or Hong Kong Prince of Wales Hospital LAAO registry (June 2009 to October 2017), we identified 30 patients who experienced ischemic stroke or TIA during follow-up after LAAO. We enrolled 86 patients who were treated with NOAC among 1,792 consecutive, acute ischemic stroke or TIA patients who were admitted to the neurology departments at 6 hospitals in South Korea (Severance Stroke Center, Gangnam Severance Stroke Center, Kyung Hee University Hospital Stroke Center, Changwon Fatima Hospital, Inje Paik Hospital, and Pusan National University Hospital) within 7 days from stroke onset from January 2013 to December 2016, despite NOAC usage among NVAF patients (Figure 1). Exclusion criteria were hemorrhagic or periprocedural strokes. In this analysis, we excluded 11 patients who underwent LAA closure due to intracranial hemorrhage and periprocedural stroke.

Left atrial appendage closure procedure and clinical follow-up
All procedures were performed by experienced operators under transesophageal echocardiography (TEE) and fluoroscopy for guidance using ACP and Watchman devices. Implanted device size was determined based on LAA angiography and pre-procedural TEE according to each device's sizing instructions.
All implanted patients were followed up via scheduled clinical visits at each center, medical report review, or telephone interviews. Clinical follow-up was complete in 1,379/1,399 of successfully implanted patients (98.6%; European ACP registry, 98.2%; Korean LAAO registry, 100%; Hong Kong Prince of Wales hospital registry, 99.1%). Although the Watchman and ACP devices were recommended in the duration of anti-coagulation and anti-platelet agents, the cessation of antithrombotic treatment after a successful procedure was done at the physician's discretion based on individualized risk estimation.6)10) Only patients with cerebrovascular events were specifically assessed at each visit for their degree of disability in daily activities. To ensure effective LAAO without significant residual leaks, the absence of device-related thrombi and erosion of the device with pericardial effusion or device embolization was determined through TEE or computed tomography regularly performed at least once 3–6 months after the procedure. Significant peri-device leakage was defined as that ≥3 and 5 mm for the ACP and Watchman devices, respectively.6)11)
Non-vitamin K antagonist oral anticoagulant treatment and clinical follow-up
Full-dose NOACs (per day) were defined as follows: dabigatran 150 mg twice, apixaban 5 mg twice, rivaroxaban 20 mg once, and edoxaban 60 mg once. Reduced NOAC doses (per day) were defined as follows: dabigatran 110 mg twice, apixaban 2.5 mg twice, rivaroxaban 15 mg or 10 mg once, and edoxaban 30 mg once. During follow-up, stroke neurologists and/or research nurses regularly contacted the patients or their caregivers via regular face-to-face visits or telephone interviews with/without medical chart review.
Definition and outcomes
All clinical events were adjudicated by 2 cardiologists for the LAAO group and stroke neurologists for the NOAC group and were confirmed by a third referee if needed. Neurologists in each institution determined the functional outcomes by review of the medical records and, face-to-face or telephone interviews after ischemic events. Stroke was defined as follows: 1) an acute episode of focal neurological dysfunction caused by brain, spinal cord, or retinal vascular injury as a result of infarction; 2) duration of neurological dysfunction over 24 hours; 3) duration of neurological dysfunction less than 24 hours due to a new imaging-documented infarction; or 4) a neurological dysfunction resulting in death.12) TIA was defined as any neurological dysfunction not satisfying the above criteria for stroke, such as lasting fewer than 24 hours without an imaging-documented acute brain infarction.12)
We assessed the functional outcome as modified Rankin Scale (mRS) scores before the event, at discharge, and at 3 and 12 months after ischemic stroke or TIA. The primary endpoint was defined as the rate of disabling ischemic stroke at discharge and at 3 and 12 months post-stroke. Disabling ischemic stroke were defined as those with a mRS score of 3 to 6.13)
Statistical analysis
Normally distributed continuous variables are expressed as means±standard deviations and were compared using Student's t-tests. Non-normally distributed continuous variables are reported as medians and interquartile ranges (interquartile range) and were compared using Mann-Whitney U test. Through linear mixed modeling, the mRS scores of 2 groups at each point were compared, and mRS scores were also compared by adjusting for various confounding factors. Categorical variables are presented as percentile values and were compared with χ2 or Fisher's exact tests as appropriate. mRS scores were treated as a continuous variable due to its linearity.13) Associations between follow-up disabling ischemic stroke at 12 months post-procedure or NOAC treatment were assessed after adjustment for multiple risk factors using the logistic regression model with the inverse probability of treatment weighting (IPTW).14) All significance tests were 2-tailed, and p values less than 0.05 indicated statistical significance. All statistical analyses were performed with SPSS statistical software (SPSS version 23.0 for Windows; IBM Corp., Armonk, NY, USA).
RESULTS
Baseline and post-procedural parameters
Patient characteristics are presented in Table 1. The overall mean age of the patients was 73.4±9.3 years (range, 46–89 years), and 46.6% (54/116) of patients were male. Compared to stroke patients treated with NOAC, those with LAAO had higher prevalence of diabetes mellitus and congestive heart failure. Other baseline and clinical characteristics, including incidence of previous stroke or TIA, were similar between the 2 groups. The risks of stroke or major bleeding as assessed by CHADS2 (p=0.69), CHA2DS2-VASc (p=0.67), and HAS-BLED scores (p=0.75) were also similar between the 2 groups.
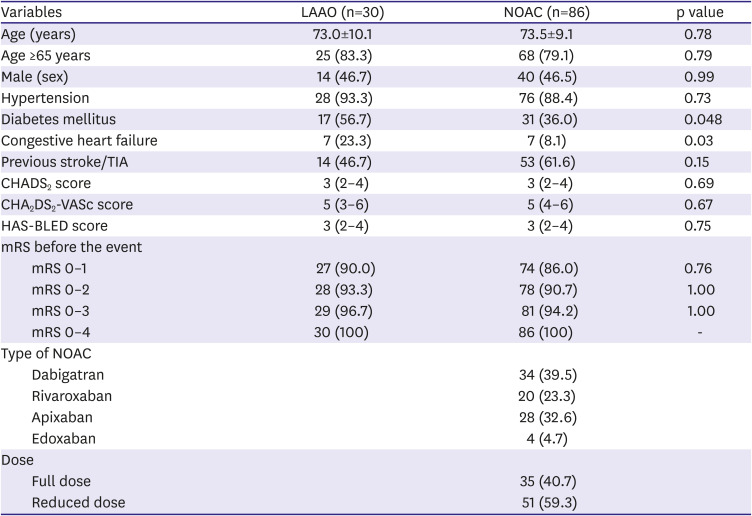
Table 1
Baseline characteristics
Data are presented as a mean±standard deviation, median (interquartile range), or number (%).
LAAO = left atrial appendage occlusion; mRS = modified Rankin Scale; NOAC = non-vitamin K antagonist oral anticoagulant; TIA = transient ischemic attack.
![]()
Among patients treated with NOACs, 39.5% (34/86) patients received dabigatran, 23.3% (20/86) received rivaroxaban, 32.6 (28/86) received apixaban, and 4.7% (4/86) patients received edoxaban. The majority of patients (59.3% [51/86]) received reduced doses of their respective NOAC because of advanced age, low body weight, or elevated creatinine level. 37 (43.0%) patients were treated with off-label dose of NOAC. Of the 86 patients who experienced stroke after taking NOACs, 19 (22.1%) were taking antiplatelet agents together (Supplementary Table 1).
The clinical indications of LAAO procedures in 30 patients with stroke were as follows: thromboembolism despite OAC treatment (n=7), previous major bleeding (n=9), high risk of bleeding (n=6), triple therapy (n=3), labile international normalized ratio (n=1), and patient preference (n=4). Among 30 patients treated with an LAA closure device, 24 (80.0%) received an ACP, and 6 (20.0%) received a Watchman device. Routine TEE surveillance was recommended at 6–8 weeks post-procedure to evaluate device positioning, the presence of device-related thrombosis, and intra- or peri-device leakage. Device thrombosis and peri-device leakage occurred in 4 (13.3%) and 3 (10.0%) patients, respectively (Table 2). In 2 patients with device thrombosis, the thrombus was not found during routine TEE surveillance, but documented at the repeat TEE after the stroke event. The time intervals between percutaneous LAA closure and stroke event of the 2 patients with device thrombosis were 2,344 and 208 days, respectively.
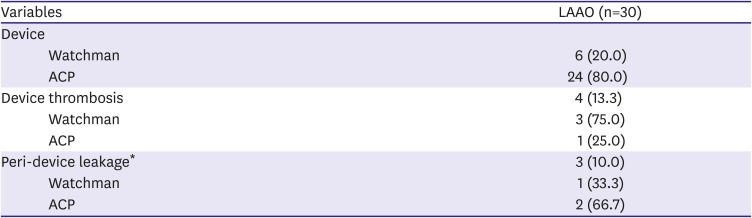
Table 2
Procedural characteristics
| Variables | LAAO (n=30) | |
|---|---|---|
| Device | ||
| Watchman | 6 (20.0) | |
| ACP | 24 (80.0) | |
| Device thrombosis | 4 (13.3) | |
| Watchman | 3 (75.0) | |
| ACP | 1 (25.0) | |
| Peri-device leakage* | 3 (10.0) | |
| Watchman | 1 (33.3) | |
| ACP | 2 (66.7) | |
Data are presented as a number (%).
ACP = Amplatzer cardiac plug; LAAO = left atrial appendage occlusion.
*Significant peri-device leakage was defined as ≥3 and 5 mm ACP and Watchman, respectively.
![]()
Cerebrovascular events
The mean intervals (months) from NOAC initiation or percutaneous LAAO to ischemic stroke or TIA were 9.9±9.8 and 20.1±20.2 months, respectively. We noted 30 ischemic events (2.1%) in the LAAO group (n=1,427), with a composite of 19 strokes and 11 TIAs. In the NOAC group (n=858), 85 strokes and one TIA occurred in patients with NVAF. Fourteen patients in the LAAO group (14/30, 46.7%) and 53 in the NOAC group (53/86, 61.6%) had a history of stroke or TIA (p=0.15). Twenty-three LAAO patients (76.7%) were on single antiplatelet therapy when the ischemic event occurred, while only 5 patients were undergoing dual antiplatelet therapy at the time of the event. Two patients were taking warfarin due to hypertrophic cardiomyopathy with AF, as well as rivaroxaban due to device thrombosis. Of the 86 patients in the NOAC group, 2 were treated with an intravenous tissue plasminogen activator (tPA) treatment, 13 were treated with endovascular treatment (EVT), and 2 were treated with both intravenous tPA and EVT after stoke.
Neurological assessment after ischemic cerebrovascular event
Neurological outcomes according to mRS categories are shown in Supplementary Table 2. Estimated mRS scores at discharge (1.8±0.3 vs. 2.7±0.2, p=0.03), 3 months (1.1±0.4 vs. 2.6±0.2, p<0.01) and at 12 months (1.0±0.4 vs. 2.5±0.2, p<0.01) post-event were lower in the LAAO group than in the NOAC group (Table 3). The LAAO group showed similar rates of disabling ischemic stroke at discharge (36.7% vs. 44.2%, p=0.52), compared to the NOAC group; however, the disabling ischemic stroke rates at 3 and 12 months post-stroke were significantly lower in LAAO patients (3 months: 23.3% vs. 44.2%, p=0.049; 12 months: 13.3% vs. 43.0%, p=0.01).
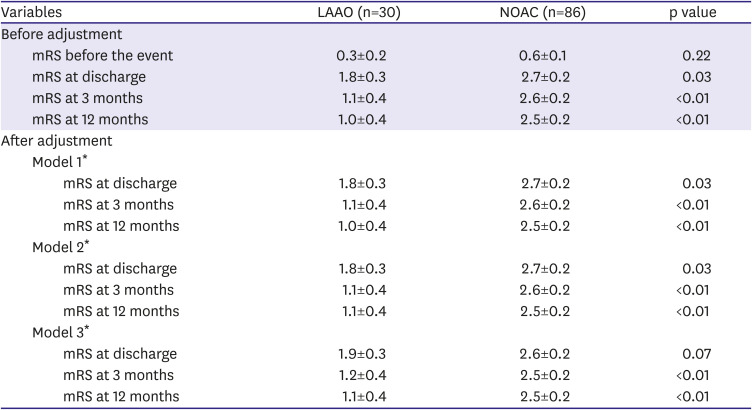
Table 3
Stroke burden after adjustments
Data are presented as the least square mean±standard error.
LAAO = left atrial appendage occlusion; mRS = modified Rankin Scale; NOAC = non-vitamin K antagonist oral anticoagulant.
*Model 1: adjusted for CHA2DS2-VASc score. Model 2: similar to model 1, with the additional inclusion of HAS-BLED score. Model 3: similar to model 2, with the additional inclusion of age, gender, and cardiovascular risk factors (age, sex, hypertension, diabetes mellitus, congestive heart failure and previous stroke/transient ischemic attack).
![]()
mRS scores between hospital discharge and 12 months post-stroke were significantly reduced in the LAAO group (Figure 2). The LAAO group showed a trend toward having a lower estimated mRS scores at baseline to those of the NOAC group (p=0.07) and scores at 12 months post-stroke were significantly lower in the LAAO group (p<0.01), even after adjusting for several variables, including CHA2DS2-VASc score, HAS-BLED score, age, gender, and other cardiovascular risk factors.
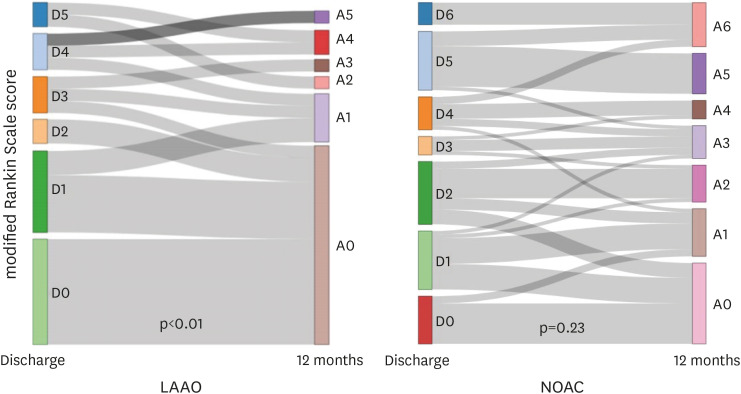
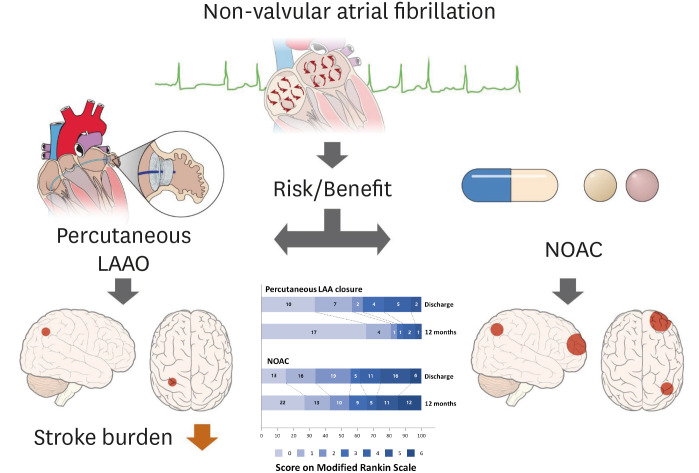
Figure 2
Comparison of stroke severity in patients treated with LAAO or NOACs. Changes in modified Rankin Scale scores of patients from each treatment group at the time of hospital discharge and at the 12-month follow-up visit are shown.
LAAO = left atrial appendage occlusion; NOAC = non-vitamin K antagonist oral anticoagulant.
![]()
Ten patients (2 in the LAAO group and 8 in the NOAC group) showed functional disability (mRS >2) before LAA closure or NOAC treatment. After excluding the above 10 patients, disabling ischemic stroke developed in 9 (32.1%) of the remaining 28 patients treated with LAAO and 30 (38.5%) of the remaining 78 patients treated with NOAC. Two (8.3%) and 29 (38.7%) patients remained disabled at 12 months after cerebrovascular events in the LAAO and NOAC groups, respectively. Similar to the results before excluding 10 patients who had previous functional disability, estimated mRS scores at 3 (p<0.01) and 12 months post-stroke (p<0.01) were significantly lower in the LAAO group, even after adjusting for several variables, including CHA2DS2-VASc score, HAS-BLED score, age, gender, and other cardiovascular risk factors (p<0.01). The LAAO group showed a trend toward having a lower estimated mRS scores at baseline to those of the NOAC group (p=0.05) (Supplementary Table 3).
Estimated mRS scores at 12 months post-stroke were significantly lower in the LAAO group, even after adjusting for several variables, including CHA2DS2-VASc score, HAS-BLED score, age, gender, and other cardiovascular risk factors (vs. off-label dose of NOAC; p<0.01, on-label dose; p=0.01) (Supplementary Tables 4 and 5).
The occurrence of disabling ischemic stroke at 12 months was significantly lower in the LAAO group (13.3%) than in the NOAC group (43.0%) (p=0.01). Similarly, recovery rates for disabling ischemic stroke at discharge to 12 months post-stroke were significantly higher for LAAO patients (50.0%) than for NOAC patients (5.6%) (p<0.01).
Using IPTW, we also evaluated the association between disabling ischemic stroke (mRS ≥3) and percutaneous LAAO, compared to NOAC treatment, after adjusting for cardiac risk factors and CHA2DS2-VASc and HAS-BLED scores. Percutaneous LAAO was significantly associated with a lower prevalence of disabling ischemic stroke at 12 months post-stroke (odds ratio, 0.23; 95% confidence interval, 0.07–0.64; p=0.01) than with NOAC treatment (Supplementary Tables 6 and 7).
DISCUSSION
The principal findings of our study are as follows: 1) the frequency of disabling ischemic stroke was lower in NVAF patients treated with LAAO than those treated with NOAC at 3 and 12 months after discharge; 2) recovery rates from disabling ischemic stroke at discharge to 12 months post-stroke were significantly greater in LAAO patients; and 3) mRS scores between discharge and 12 months post-ischemic cerebrovascular events were significantly reduced in the LAAO group. To the best of our knowledge, this is the first clinical study comparing the neurological outcomes of NVAF patients with LAAO and NOAC treatment after ischemic cerebrovascular events, even after excluding hemorrhagic stroke (Figure 3).
Previous papers have reported less lethal and disabling ischemic stroke after percutaneous LAAO than those treated with warfarin.7)9) More recently, we reported that NVAF patients previously treated with LAAO experienced more favorable outcomes following ischemic cerebrovascular events than patients taking warfarin.8) The prevalence of disabling ischemic stroke were 37.5% and 58.8% at discharge (p=0.07), 20.8% and 42.6% at 3 months (p=0.08), and 12.5% and 39.7% at 12 months (p=0.02) in the LAAO and warfarin groups, respectively. The mRS was significantly lower in the LAAO group at discharge, 3 months, and 12 months after ischemic cerebrovascular events (all p<0.01), despite no significant difference in mRS before ischemic cerebrovascular events (p=0.98). Patients in the LAAO group showed a significant reduction in mRS between discharge and 12 months (p<0.01), unlike patients in the warfarin group (p=0.10). Our current study expounded on favorable neurological outcomes of LAAO in patients with ischemic cerebrovascular events in comparison with NOAC treatment.
The incidences of ischemic stroke and TIA events were 1.33% (19 out of 1,427) and 0.77% (11 out of 1,427) in NVAF patients treated with LAAO were markedly low and within acceptable limits, especially considering the higher prevalence of previous cerebrovascular events (46.7%) and a high CHA2DS2-VASc score of 4.7±1.5 in these patients. Similarly, although hemorrhagic stroke was excluded from our formal analysis, the occurrence of intracranial hemorrhage events was low, despite relatively high HAS-BLED scores in our study participants. Thus, the low incidences of ischemic stroke, TIA, and/or hemorrhagic stroke in high-risk patients may be valuable advantages of LAAO over NOAC therapy.
Stroke in AF patients has been extensively associated with higher mortality and greater disability.1)2) In this study, after excluding LAAO patients with functional disability before the index event, only 2 patients (8.3%) remained disabled at 12 months after discharge, compared to 29 NOAC patients (38.7%). Of these patients, 32.1% (9/28) and 38.5% (30/78) of the patients in the LAAO and NOAC groups, respectively, presented with severe functional disability (mRS >2) at hospital discharge. Moreover, rates of recovery from disabling ischemic stroke at 12 months post-event were significantly higher in the LAAO group (66.7%) than in the NOAC group (7.1%). Significantly reduced mRS scores between hospital discharge and 12 months post-stroke were also seen in LAAO patients, but not in NOAC patients. These findings corroborate those of the PROTECT-AF trial,15) which reported disabling ischemic stroke in 31% (8/26) of patients after LAAO and in 55% (11/20) of patients after warfarin treatment with relatively low CHA2DS2-VASc scores. However, some differences between the PROTECT-AF study and the current study must be considered: Unlike the PROTECT-AF study, our study showed a lower rate of disabling ischemic stroke in LAAO, compared to anti-coagulant treatment only, from ischemic stroke and TIA, even after excluding hemorrhagic stroke, since hemorrhagic stroke is known to be more prevalent in anticoagulant treatment including NOAC. Secondly, the PROTECT-AF study used only the Watchman device for stroke prevention, while we included both the Watchman and ACP devices. However, the mRS scores post-stroke were not significantly different between the devices in our study, even after adjusting for multiple potential risk factors.
The favorable neurological outcomes we observed in LAAO patients may be explained in several ways. Stroke severity in NVAF could be affected by the patient characteristics of age, risk stratification, stroke mechanism, or prior antithrombotic medication status. In this study, there were no differences in age and, CHADS2 or CHA2DS2-VASc scores between patients with LAAO and those with NOAC, which implies that the different neurological outcomes did not result from different baseline characteristics. Instead, compared to NOAC, LAAO could more effectively prevent thrombus formation within the heart, as most strokes in NVAF patients are caused by thrombi that originate from LAA and as severe stroke is related to larger thrombi in LAA.2) In a previous study, LAA closure was associated with an improvement in LA mechanical function,16) a powerful predictor of major cardiovascular events.17) In this regard, the neurological outcomes may have been better in patients who were treated with LAAO than by NOAC. LAAO has another benefit over anticoagulation in the setting of hemorrhagic complications following cerebral infarction in that it does not impact hemorrhagic transformation; therefore, anticoagulants would likely lead to more favorable neurological outcomes. Although OAC therapy can prevent the formation of intracardiac thrombi, its efficacy may be insufficient in patients with higher CHA2DS2-VASc scores or previous history of stroke18) On the contrary, the benefit of LAAO was greater in patients with higher CHA2DS2-VASc scores or those with previous history of stroke.19) In addition, the clinical net benefit of LAAO can be more prominent over 9 months after the procedure.20) Our study population had high CHA2DS2-VASc scores or higher proportion of previous stroke, and patients in LAAO group were followed up for more than 20 months. These factors could have led to more favorable outcomes for LAAO in our study.
Some limitations of our study should be noted. First, this is a retrospective, non-randomized, observational study that included a small number of patients, even from 3 multi-center registries. Therefore, there were some limitations in collecting detailed information of baseline characteristics, as well as comparing outcomes according to different devices and specific NOACs or different doses of NOACs. Additionally, the incidences of stroke in these registries for both groups were remarkably low because of possible incomplete reporting of stroke. Nevertheless, this is the first clinical study reporting the neurological outcomes of NVAF patients after treatment with LAAO devices, compared with NOAC therapy. Second, recurrent vascular events or hemorrhagic strokes were not analyzed in this study. Third, one should consider the different ethnicities between the LAAO group and NOAC groups. Fourth, although the degree or types of rehabilitation treatment could be associated with a patient's outcome, stroke patients included in this analysis received rehabilitation treatment in various centers, and we did not adjust the impact of rehabilitation, which could be another limitation in this study. Sixth, we did not compare the infarct size (area or volume in neuroimaging study), but we focused on comparing the functional neurological outcome through mRS and proportion of disabling ischemic stroke. Finally, in the current study, there was no imaging core lab for the acquisition and analysis of images. However, as a manner of multi-center registry, the analysis of echocardiographic images was performed by imaging specialists at each participating center, and all assessments of images were conducted following the generally recommended protocol.10)
In conclusion, percutaneous LAAO yielded favorable neurological outcomes, compared with NOAC, in patients who experienced ischemic cerebrovascular events. These findings suggest an increased neurological benefit of LAAO over NOAC use for long-term protection against thrombus formation in NVAF patients, including those at higher risk of cardio- and cerebrovascular events.
 XML Download
XML Download