

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Sarcoidosis is a chronic multi-system inflammatory disorder of unknown etiology characterized pathologically by the formation of non-caseating granulomas in the involved organs or tissues. Essentially, any body tissue may be affected,1)2) but the most commonly involved include the lymph nodes, skin, lung, musculoskeletal system, and eyes.
Although the overall prognosis of patients with systemic sarcoidosis is generally favorable, cardiac sarcoidosis (CS) is significantly associated with a poor prognosis due to congestive heart failure, arrhythmias (such as an advanced atrioventricular block), and ventricular tachyarrhythmia.3)4) Thus, an early and precise diagnosis of CS is essential. Recent studies have demonstrated the usefulness of 18F-fluorodeoxyglucose (18F-FDG) positron emission tomography (PET) and cardiac magnetic resonance imaging (CMR) for assessing CS. In this review, we focus on the pathophysiology and diagnostic aspects of CS with multimodality imaging.
Go to : 
ETIOLOGY
The incidence of sarcoidosis and its cardiac involvement varies among ethnic groups and regions.5)6) Symptomatic CS has been reported in up to 10% of the patients with systemic sarcoidosis.7)8)9)10) An autopsy series from the United States and Japan showed that approximately 27% and 80% of patients with systemic sarcoidosis, respectively, had CS.11)12) Recent advances in cardiac imaging tools have enabled the detection of asymptomatic CS.13) As such, imaging series have reported higher rates of cardiac involvement in patients with extra-CS, ranging from 19% to 55% for asymptomatic CS.4)8)13)14)15)
Go to :
PATHOLOGICAL CHARACTERISTICS OF CARDIAC SARCOIDOSIS
The pathological hallmark of CS is the non-caseating epithelioid granuloma with a compact central area of macrophages and scattered lymphocytes.1) If there is active inflammation, the granuloma can progress to irreversible fibrosis.16) The myocardium of the left ventricular free wall is the most common location of sarcoid involvement, followed by the interventricular septum, papillary muscles, right ventricle, and atria.17)18) An endomyocardial biopsy is a valuable tool in the definitive diagnosis of CS,19) but it is limited owing to its low sensitivity due to the patchy distribution of granulomas and its complications.
Go to :
CLINICAL PRESENTATION
CS manifestations can range widely from a clinically asymptomatic form to sudden cardiac death.20) Arrhythmic, cardiomyopathic, and pericardial manifestations are common clinical signs and symptoms (Table 1).20)21)22)23)24)25)
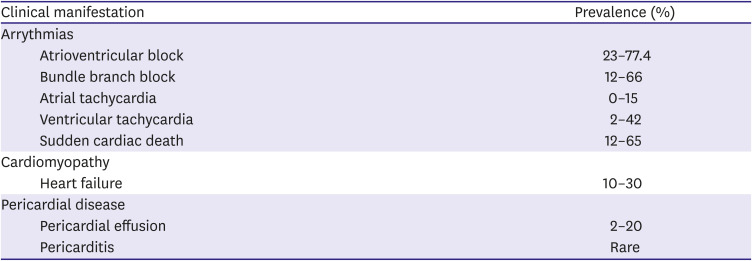
Table 1
Clinical presentations of cardiac sarcoidosis
![]()
Atrioventricular conduction disease due to the infiltration of sarcoid granulomas is the most common finding in patients with CS.26) Ventricular and atrial arrhythmias are also frequent manifestations, with the latter being caused by atrial dilation secondary to left ventricular dysfunction and the atrial infiltration of sarcoid granulomas. Both systolic and diastolic ventricular dysfunction can result from granulomatous inflammation and subsequent scarring, subsequently leading to heart failure. Meanwhile, pulmonary infiltration may lead to right ventricular failure. Less commonly, CS may manifest as progressive pericardial diseases, such as pericarditis or tamponade.
Go to :
CRITERIA FOR THE DIAGNOSIS OF CARDIAC SARCOIDOSIS
CS is conventionally diagnosed by the appropriate combination of clinical and physiological signs and symptoms and multimodal imaging. Several diagnostic criteria have been proposed, and one commonly used is the Japanese Ministry of Health and Welfare criteria,27)28) modified in 2015 by the Japanese Society of Sarcoidosis and Other Granulomatous Disorders (Table 2).25) The Heart Rhythm Society Expert Consensus Statement of the CS was also published in 2014 (Table 3).29) In these 2 criteria, the diagnosis is separated by histological and clinical methods. To confirm the histological diagnosis, the presence of non-caseating epithelioid granulomas from the endomyocardial biopsy sample should be demonstrated. The histological analysis of operative or endomyocardial biopsy specimens could be the gold standard. However, endomyocardial biopsy cannot be performed on all suspected regions and has a lower sensitivity in diagnosing CS.19) On the contrary, the clinical diagnosis correlates the histological diagnosis of extra-cardiac sarcoidosis with the electrocardiographic and imaging findings, including echocardiography, 67Ga scintigraphy, 18F-FDG PET, and late gadolinium enhancement on CMR.
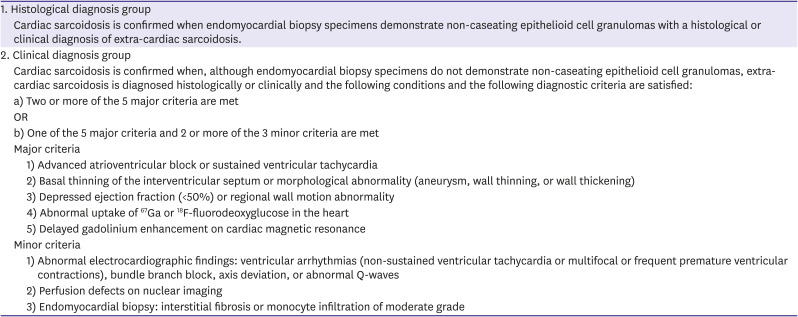
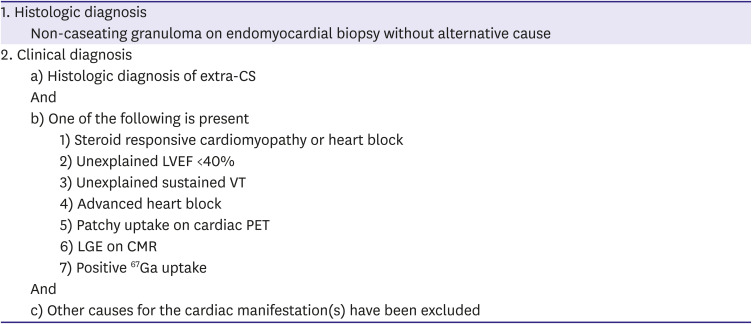
Table 2
Japanese Society of Sarcoidosis and Other Granulomatous Disorders 2015 criteria for cardiac sarcoidosis25)
![]()
Table 3
Heart Rhythm Society's Expert Consensus Statement for diagnosis of CS29)
CMR = cardiac magnetic resonance imaging; CS = cardiac sarcoidosis; LGE = late gadolinium enhancement; LVEF = left ventricular ejection fraction; PET = positron emission tomography; VT = ventricular tachycardia.
![]()
Go to :
18F-FLUORODEOXYGLUCOSE POSITRON EMISSION TOMOGRAPHY/COMPUTED TOMOGRAPHY
PET is a highly sensitive and non-invasive molecular imaging technique that can visualize and quantify the active processes of physiological function and disease conditions, in contrast to anatomical approaches. 18F-FDG is a glucose analog widely used to visualize and quantify glucose metabolism in the target region since it is taken up by plasma membrane glucose transporters (GLUT) in living cells and phosphorylated by intracellular hexokinase into 18F-FDG-6-phosphate (18F-FDG-6-P) similar to glucose. 18F-FDG-6-P is retained within the cell without further metabolism along the glycolytic pathway, a phenomenon known as metabolic trapping. Therefore, tissue activity can be directly visualized using 18F-FDG PET.
Cardiac metabolism and preparation to suppress the physiological 18F-fluorodeoxyglucose uptake
Under normal conditions, free fatty acids (FFAs) and glucose are the major energy sources for cardiac metabolism. Since the 18F-FDG is an analog of glucose, its physiological accumulation in the myocardium has a causal influence on the false-positive diagnosis of CS.30) The fasting state has a significant effect on the physiological uptake. Figure 1 shows a representative case of various physiological uptakes during follow-up in one patient (non-CS case). Under long fasting conditions, glucose production and glucose oxidation decrease, leading to the release of available FFA from adipose tissue to provide an alternative energy source. The physiological uptake of 18F-FDG in the myocardium can be suppressed with a low-carbohydrate diet and a high-fat diet due to the switch to FFA metabolism. As such, FFA level is an important marker of physiological 18F-FDG uptake suppression.31)
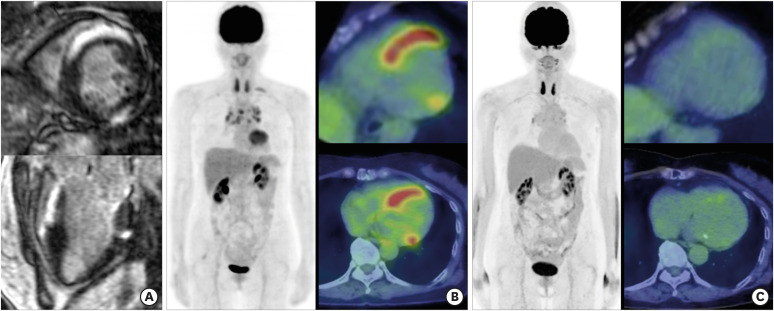
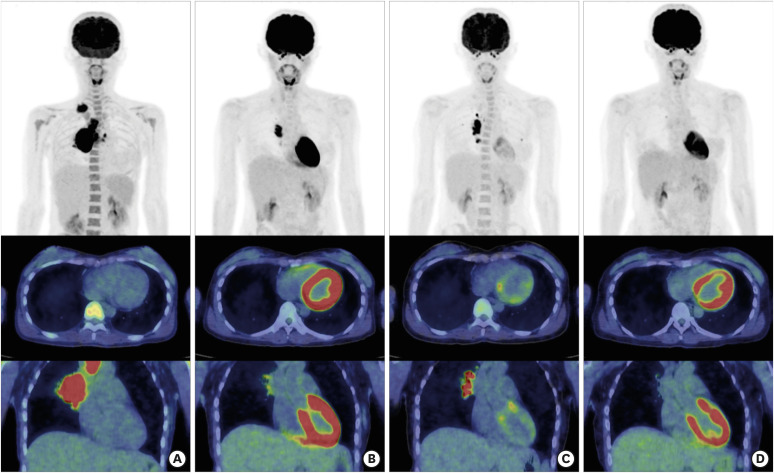 | Figure 1A representative case of various physiological myocardial uptake patterns during follow-up in one patient.A patient with malignant lymphoma underwent serial 18F-fluorodeoxyglucose positron emission tomography/computed tomography scans for follow-up after chemotherapy. Focus on the left ventricular uptake, no uptake (A), diffuse strong uptake with left ventricular uptake (B), predominant regional uptake in the base of the myocardium (C), and diffuse uptake (D) is pointed out.
|
18F-fluorodeoxyglucose accumulation in sarcoidosis lesion
The significant 18F-FDG accumulation in sarcoidosis lesions is caused by activated inflammatory cells, such as neutrophils, macrophages, and lymphocytes; GLUT1 and GLUT3 in the cell membrane; and hexokinase.32)33) As 18F-FDG uptake reflects active inflammation, it is therefore useful in detecting CS and guiding immunosuppression management.34)
Figure 2 shows a representative case of CS before and after steroid therapy.
 | Figure 2A representative case of a woman in her 60s with complete right bundle branch block before and after steroid therapy. Cardiac magnetic resonance shows subepicardial gadolinium enhancement at the basal septum and lateral wall (A). Focal myocardial fluorodeoxyglucose uptake at the septum and multiple uptake at the mediastinal lymph nodes are consistent with cardiac sarcoidosis (B). After administration of steroid therapy, myocardial and mediastinal uptake are diminished (C).
|
Myocardial 18F-FDG uptake patterns are conventionally divided into 4 groups: none, diffuse, focal, and focal on diffuse.35)36) When myocardial 18F-FDG uptake is absent, it is negative for active CS lesions. Definite diffuse 18F-FDG uptake in the entire left ventricular wall is generally a physiological uptake and does not indicate an abnormality. On the contrary, focal and focal on diffuse 18F-FDG uptake in the left ventricular wall are considered positive for CS. In addition, the diffuse at base uptake pattern is known to be associated with inadequate physiologic suppression.37)
The combination of 18F-FDG and perfusion findings has led to improvements in the accurate diagnoses and prognostication.3)
With its high diagnostic value and high inter-rater reproducibility, 18F-FDG PET texture analysis can also be used to diagnose CS, focusing on its heterogeneous distribution.38) Texture analysis can differentiate abnormal and physiological CS uptake.
Go to :
CARDIAC MAGNETIC RESONANCE IMAGING
Late gadolinium enhancement
CMR offers both functional and structural information to help detect the acute and chronic inflammatory phases of CS. In contrast, it does not require specific preparation such as long fasting before examination as required for 18F-FDG PET; however, it is contraindicated in patients with MR unsafe or some MR conditional implantable devices.
CMR with late gadolinium enhancement (LGE) is an emerging tool for evaluating CS. Mid-wall or subepicardial LGE in the basal ventricular wall, lateral wall, and septum (Figure 2) is the most common pattern seen in CS,4) recently confirmed in a meta-analysis of studies with histological confirmation.39)
Myocardial enhancement on LGE-CMR images adds an independent prognostic value for the risk stratification sarcoidosis patients.40)41) Greulich et al.8) also reported that the presence of LGE was the best independent predictor of death and other adverse events in CS. However, it is difficult to differentiate active inflammation from chronic fibrosis using LGE alone.
T1/T2 mapping
CMR mapping techniques such as T1, T2, and extracellular volume can provide additional quantitative information regarding interstitial changes. In combination with LGE, CMR mapping can significantly improve the diagnosis of subclinical CS.42) Greulich et al.43) compared 61 patients with sarcoidosis and 26 healthy patients and found that the former had significantly higher native T1, T2, and extracellular volume. The weighted mean T1 value at 1.5 T of 994 ms (range, 975–1,039 ms) in the patients with sarcoidosis was significantly higher than the controls (960 ms; range, 942–986 ms), independent of the presence of LGE. Meanwhile, the patients with sarcoidosis had a weighted mean T2 value at 1.5 T of 52.3 ± 3.8 ms, higher than the 49.0 ± 1.6 ms in the controls. At 3 T, the values were 54.0 ± 12.2 ms and 45.0 ± 10.8 ms, respectively.44)
Figure 3 shows active CS with LGE-CMR and T2 mapping, which correlate with positive 18F-FDG PET findings. T2 mapping provides an absolute and objective parameter for active inflammation. Native T1 and T2 mapping could be used for disease monitoring and differentiating sarcoid patients from healthy controls without the use of gadolinium.45)
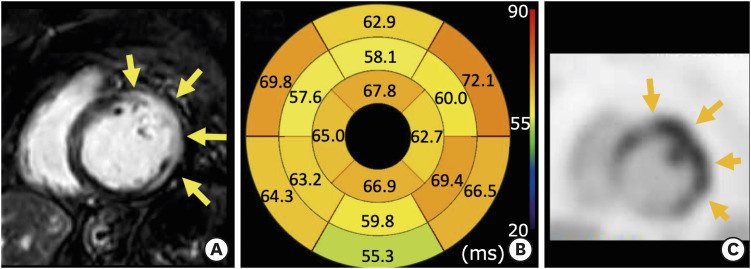 | Figure 3A woman in her 60s was admitted to the hospital with acute heart failure. Cardiac magnetic resonance imaging shows abnormal gadolinium enhancement with transmural and epicardium distribution of left ventricle (A, arrows). Through T2 mapping, the diffuse prolongation of T2 values is observed, suggesting myocardial edema or inflammation due to active cardiac sarcoidosis (B, normal range was under 54 ms). 18F-fluorodeoxyglucose positron emission tomography/computed tomography reveals correlated focal uptake, confirming active cardiac sarcoidosis (C, arrows).
|
Strain imaging
Myocardial strain analysis has been developed to objectively evaluate the regional myocardial function, including longitudinal, circumferential, radial, and rotational myocardial strains.46) Among these, left ventricular global longitudinal strain (GLS) has been receiving the most attention because subendocardial fibers originate longitudinally and thus, may be sensitive in detecting early changes in various cardiomyopathies. Two-dimensional speckle tracking echocardiography has been used to evaluate CS. GLS and global circumferential strain were significantly lower in extra-cardiac sarcoidosis patients despite not exhibiting any cardiac symptoms.47) Impaired GLS is associated with major cardiac events in patients with CS.47) Due to its association with cardiac events in patients with sarcoidosis, a recent study also reported that biventricular strain deterioration can be used as an early marker of cardiac involvement.48)
Similar to speckle tracking echocardiography, CMR techniques for assessing myocardial strain, such as tagging,49) strain-encoded (SENC) magnetic resonance imaging (MRI),50)51) and myocardial feature-tracking deformation imaging (FTI),52) have the potential to detect a wide range of myocardial diseases early, accurately, and without the need for contrast agent injection. A small study using SENC for CS has been reported.53) Specifically, FTI is also useful for evaluating regional and global strains, well correlated with SENC MRI.54) This method requires only cine images without specific extra scanning. Dabir et al.55) reported that GLS assessed with FTI was reduced in patients with a negative outcome, possibly serving as a marker for early cardiac involvement in sarcoidosis. Figure 4 shows a case of positive LGE and 18F-FDG PET with FTI evaluation. In this case, regional deformation due to aneurysmal formation was visualized well with FTI.
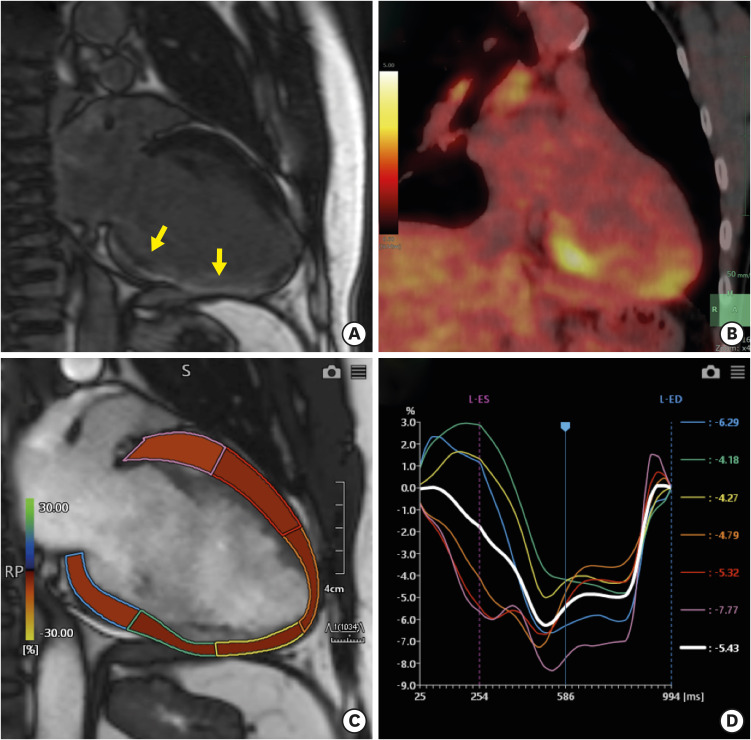 | Figure 4A man in his 40s was diagnosed as systemic sarcoidosis by transbronchial lung biopsy.Due to complete right bundle branch block and diffuse left ventricular dysfunction, he was referred for CMR. Left ventricular 2-chamber view of the late gadolinium enhanced CMR shows hyperenhancement at the inferior wall (A, yellow arrows). After a long fast with a low-carbohydrate diet, the 18F-FDG positron emission tomography/computed tomography reveals abnormal FDG uptake at the inferior wall, indicating active cardiac sarcoidosis (B). (C and D) Feature-tracking using cine magnetic resonance imaging for longitudinal strain clearly depicts regional wall motion abnormality with aneurysmal deformation of the mid-inferior wall (green strain curve).
CMR = cardiac magnetic resonance imaging; FDG = fluorodeoxyglucose.
|
An autopsy study reported that aneurysm formation was present in 8% of patients with cardiac sarcoidosis,18) the combination of CMR and 18F-FDG PET could help differentiate left ventricular aneurysm due to CS from myocardial infarction.
Go to :
DIAGNOSTIC ABILITY
Systematic reviews about the diagnostic ability of 18F-FDG PET and CMR are summarized in Tables 4, 5, 6.56)57)58)59)60)61)62)63)64)65)66)67)68)69)70)71)72)73)74)75)76)77)78)79)80)81)82)83)84)85)86)87)88)89)90)91)92)93)94)95)96)97)98)99)100)101)102)103)104)105)106)107)108)109)110)111) The sensitivity of 18F-FDG PET in the diagnosis of CS ranges from 27% to 100%, depending on disease activity since it can only detect active lesions. CMR has a similar sensitivity in detecting CS (range, 28%–100%). Importantly, 18F-FDG PET and CMR provide different aspects of the pathophysiology of CS.108) Therefore, both modalities are recommended for patients who meet the following criteria: (1) equivocal or negative CMR findings in the setting of high clinical suspicion; (2) CMR findings with highly probable CS. In such cases, 18F-FDG PET may identify inflammation/potential role for immunosuppressive therapies. The suggested algorithm for diagnosis is CMR. If LGE is negative, the patient's prognosis would be excellent. However, if LGE is positive or inconclusive, the disease activity should be evaluated using 18F-FDG PET for immunosuppressive therapy.
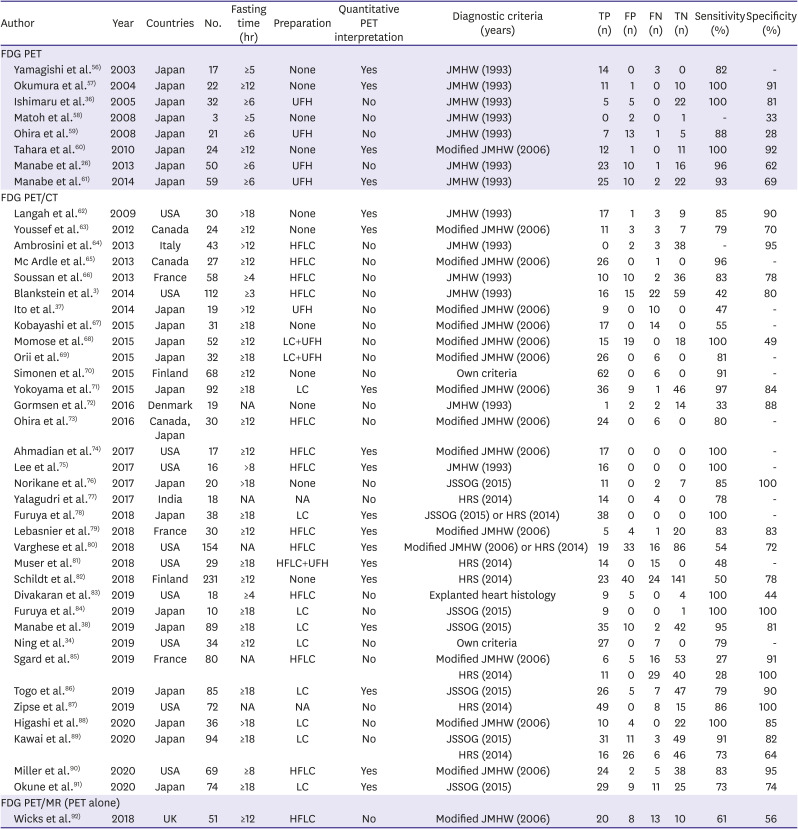
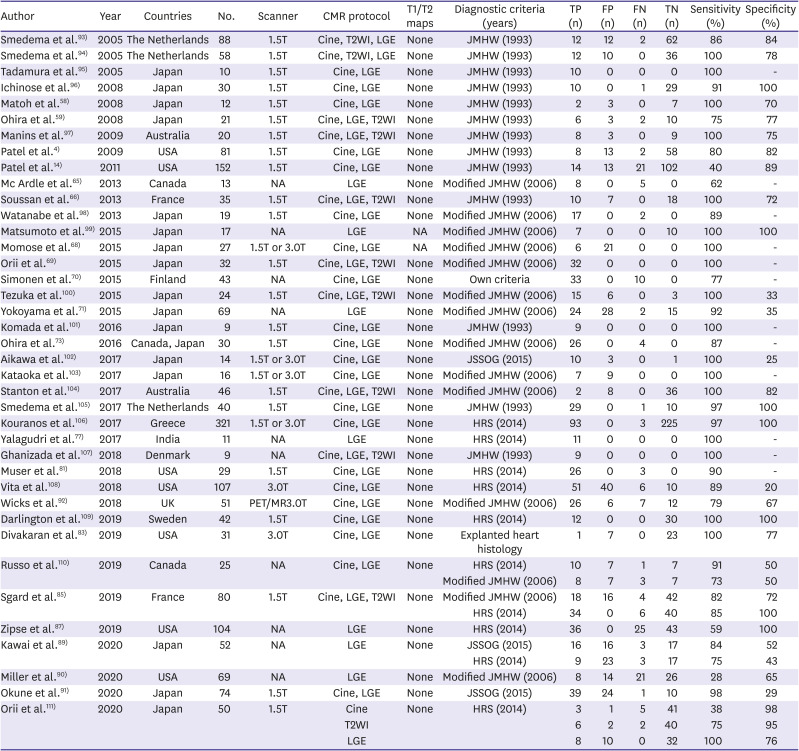
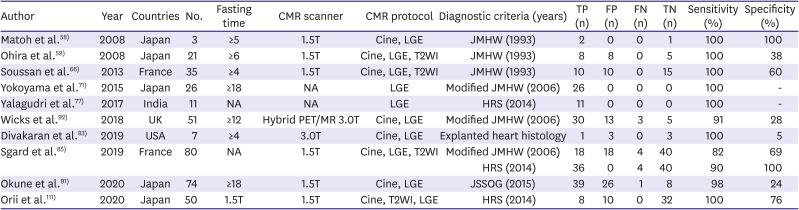
Table 4
Diagnostic performance of 18F-FDG PET and 18F-FDG PET/CT to detect cardiac involvement in patients with sarcoidosis
| Author | Year | Countries | No. | Fasting time (hr) | Preparation | Quantitative PET interpretation | Diagnostic criteria (years) | TP (n) | FP (n) | FN (n) | TN (n) | Sensitivity (%) | Specificity (%) | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| FDG PET | ||||||||||||||
| Yamagishi et al.56) | 2003 | Japan | 17 | ≥5 | None | Yes | JMHW (1993) | 14 | 0 | 3 | 0 | 82 | - | |
| Okumura et al.57) | 2004 | Japan | 22 | ≥12 | None | Yes | JMHW (1993) | 11 | 1 | 0 | 10 | 100 | 91 | |
| Ishimaru et al.36) | 2005 | Japan | 32 | ≥6 | UFH | No | JMHW (1993) | 5 | 5 | 0 | 22 | 100 | 81 | |
| Matoh et al.58) | 2008 | Japan | 3 | ≥5 | None | No | JMHW (1993) | 0 | 2 | 0 | 1 | - | 33 | |
| Ohira et al.59) | 2008 | Japan | 21 | ≥6 | UFH | No | JMHW (1993) | 7 | 13 | 1 | 5 | 88 | 28 | |
| Tahara et al.60) | 2010 | Japan | 24 | ≥12 | None | Yes | Modified JMHW (2006) | 12 | 1 | 0 | 11 | 100 | 92 | |
| Manabe et al.26) | 2013 | Japan | 50 | ≥6 | UFH | No | JMHW (1993) | 23 | 10 | 1 | 16 | 96 | 62 | |
| Manabe et al.61) | 2014 | Japan | 59 | ≥6 | UFH | Yes | JMHW (1993) | 25 | 10 | 2 | 22 | 93 | 69 | |
| FDG PET/CT | ||||||||||||||
| Langah et al.62) | 2009 | USA | 30 | >18 | None | Yes | JMHW (1993) | 17 | 1 | 3 | 9 | 85 | 90 | |
| Youssef et al.63) | 2012 | Canada | 24 | ≥12 | None | Yes | Modified JMHW (2006) | 11 | 3 | 3 | 7 | 79 | 70 | |
| Ambrosini et al.64) | 2013 | Italy | 43 | >12 | HFLC | No | JMHW (1993) | 0 | 2 | 3 | 38 | - | 95 | |
| Mc Ardle et al.65) | 2013 | Canada | 27 | ≥12 | HFLC | No | Modified JMHW (2006) | 26 | 0 | 1 | 0 | 96 | - | |
| Soussan et al.66) | 2013 | France | 58 | ≥4 | HFLC | No | JMHW (1993) | 10 | 10 | 2 | 36 | 83 | 78 | |
| Blankstein et al.3) | 2014 | USA | 112 | ≥3 | HFLC | No | JMHW (1993) | 16 | 15 | 22 | 59 | 42 | 80 | |
| Ito et al.37) | 2014 | Japan | 19 | >12 | UFH | No | Modified JMHW (2006) | 9 | 0 | 10 | 0 | 47 | - | |
| Kobayashi et al.67) | 2015 | Japan | 31 | ≥18 | None | No | Modified JMHW (2006) | 17 | 0 | 14 | 0 | 55 | - | |
| Momose et al.68) | 2015 | Japan | 52 | ≥12 | LC+UFH | No | Modified JMHW (2006) | 15 | 19 | 0 | 18 | 100 | 49 | |
| Orii et al.69) | 2015 | Japan | 32 | ≥18 | LC+UFH | No | Modified JMHW (2006) | 26 | 0 | 6 | 0 | 81 | - | |
| Simonen et al.70) | 2015 | Finland | 68 | ≥12 | None | No | Own criteria | 62 | 0 | 6 | 0 | 91 | - | |
| Yokoyama et al.71) | 2015 | Japan | 92 | ≥18 | LC | Yes | Modified JMHW (2006) | 36 | 9 | 1 | 46 | 97 | 84 | |
| Gormsen et al.72) | 2016 | Denmark | 19 | NA | None | No | JMHW (1993) | 1 | 2 | 2 | 14 | 33 | 88 | |
| Ohira et al.73) | 2016 | Canada, Japan | 30 | ≥12 | HFLC | No | Modified JMHW (2006) | 24 | 0 | 6 | 0 | 80 | - | |
| Ahmadian et al.74) | 2017 | USA | 17 | ≥12 | HFLC | Yes | Modified JMHW (2006) | 17 | 0 | 0 | 0 | 100 | - | |
| Lee et al.75) | 2017 | USA | 16 | >8 | HFLC | Yes | JMHW (1993) | 16 | 0 | 0 | 0 | 100 | - | |
| Norikane et al.76) | 2017 | Japan | 20 | >18 | None | No | JSSOG (2015) | 11 | 0 | 2 | 7 | 85 | 100 | |
| Yalagudri et al.77) | 2017 | India | 18 | NA | NA | No | HRS (2014) | 14 | 0 | 4 | 0 | 78 | - | |
| Furuya et al.78) | 2018 | Japan | 38 | ≥18 | LC | Yes | JSSOG (2015) or HRS (2014) | 38 | 0 | 0 | 0 | 100 | - | |
| Lebasnier et al.79) | 2018 | France | 30 | ≥12 | HFLC | Yes | Modified JMHW (2006) | 5 | 4 | 1 | 20 | 83 | 83 | |
| Varghese et al.80) | 2018 | USA | 154 | NA | HFLC | Yes | Modified JMHW (2006) or HRS (2014) | 19 | 33 | 16 | 86 | 54 | 72 | |
| Muser et al.81) | 2018 | USA | 29 | ≥18 | HFLC+UFH | Yes | HRS (2014) | 14 | 0 | 15 | 0 | 48 | - | |
| Schildt et al.82) | 2018 | Finland | 231 | ≥12 | None | Yes | HRS (2014) | 23 | 40 | 24 | 141 | 50 | 78 | |
| Divakaran et al.83) | 2019 | USA | 18 | ≥4 | HFLC | No | Explanted heart histology | 9 | 5 | 0 | 4 | 100 | 44 | |
| Furuya et al.84) | 2019 | Japan | 10 | ≥18 | LC | No | JSSOG (2015) | 9 | 0 | 0 | 1 | 100 | 100 | |
| Manabe et al.38) | 2019 | Japan | 89 | ≥18 | LC | Yes | JSSOG (2015) | 35 | 10 | 2 | 42 | 95 | 81 | |
| Ning et al.34) | 2019 | USA | 34 | ≥12 | LC | No | Own criteria | 27 | 0 | 7 | 0 | 79 | - | |
| Sgard et al.85) | 2019 | France | 80 | NA | HFLC | No | Modified JMHW (2006) | 6 | 5 | 16 | 53 | 27 | 91 | |
| HRS (2014) | 11 | 0 | 29 | 40 | 28 | 100 | ||||||||
| Togo et al.86) | 2019 | Japan | 85 | ≥18 | LC | Yes | JSSOG (2015) | 26 | 5 | 7 | 47 | 79 | 90 | |
| Zipse et al.87) | 2019 | USA | 72 | NA | NA | No | HRS (2014) | 49 | 0 | 8 | 15 | 86 | 100 | |
| Higashi et al.88) | 2020 | Japan | 36 | >18 | LC | No | Modified JMHW (2006) | 10 | 4 | 0 | 22 | 100 | 85 | |
| Kawai et al.89) | 2020 | Japan | 94 | ≥18 | LC | No | JSSOG (2015) | 31 | 11 | 3 | 49 | 91 | 82 | |
| HRS (2014) | 16 | 26 | 6 | 46 | 73 | 64 | ||||||||
| Miller et al.90) | 2020 | USA | 69 | ≥8 | HFLC | Yes | Modified JMHW (2006) | 24 | 2 | 5 | 38 | 83 | 95 | |
| Okune et al.91) | 2020 | Japan | 74 | ≥18 | LC | Yes | JSSOG (2015) | 29 | 9 | 11 | 25 | 73 | 74 | |
| FDG PET/MR (PET alone) | ||||||||||||||
| Wicks et al.92) | 2018 | UK | 51 | ≥12 | HFLC | No | Modified JMHW (2006) | 20 | 8 | 13 | 10 | 61 | 56 | |
CT = computed tomography; FDG = fluorodeoxyglucose; FN = false negative; FP = false-positive; HFLC = high-fat/low-carbohydrate diet; HRS = Heart Rhythm Society; JMHW = Japanese Ministry of Health and Welfare; JSSOG = Japanese Society of Sarcoidosis and Other Granulomatous Disorders; LC = low-carbohydrate; MR = magnetic resonance; NA = not available; PET = positron emission tomography; TN = true negative; TP = true positive; UFH = unfractionated heparin injection.
![]()
Table 5
Diagnostic performance of CMR to detect cardiac involvement in patients with sarcoidosis
| Author | Year | Countries | No. | Scanner | CMR protocol | T1/T2 maps | Diagnostic criteria (years) | TP (n) | FP (n) | FN (n) | TN (n) | Sensitivity (%) | Specificity (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Smedema et al.93) | 2005 | The Netherlands | 88 | 1.5T | Cine, T2WI, LGE | None | JMHW (1993) | 12 | 12 | 2 | 62 | 86 | 84 |
| Smedema et al.94) | 2005 | The Netherlands | 58 | 1.5T | Cine, T2WI, LGE | None | JMHW (1993) | 12 | 10 | 0 | 36 | 100 | 78 |
| Tadamura et al.95) | 2005 | Japan | 10 | 1.5T | Cine, LGE | None | JMHW (1993) | 10 | 0 | 0 | 0 | 100 | - |
| Ichinose et al.96) | 2008 | Japan | 30 | 1.5T | Cine, LGE | None | JMHW (1993) | 10 | 0 | 1 | 29 | 91 | 100 |
| Matoh et al.58) | 2008 | Japan | 12 | 1.5T | Cine, LGE | None | JMHW (1993) | 2 | 3 | 0 | 7 | 100 | 70 |
| Ohira et al.59) | 2008 | Japan | 21 | 1.5T | Cine, LGE, T2WI | None | JMHW (1993) | 6 | 3 | 2 | 10 | 75 | 77 |
| Manins et al.97) | 2009 | Australia | 20 | 1.5T | Cine, LGE, T2WI | None | JMHW (1993) | 8 | 3 | 0 | 9 | 100 | 75 |
| Patel et al.4) | 2009 | USA | 81 | 1.5T | Cine, LGE | None | JMHW (1993) | 8 | 13 | 2 | 58 | 80 | 82 |
| Patel et al.14) | 2011 | USA | 152 | 1.5T | Cine, LGE | None | JMHW (1993) | 14 | 13 | 21 | 102 | 40 | 89 |
| Mc Ardle et al.65) | 2013 | Canada | 13 | NA | LGE | None | Modified JMHW (2006) | 8 | 0 | 5 | 0 | 62 | - |
| Soussan et al.66) | 2013 | France | 35 | 1.5T | Cine, LGE, T2WI | None | JMHW (1993) | 10 | 7 | 0 | 18 | 100 | 72 |
| Watanabe et al.98) | 2013 | Japan | 19 | 1.5T | Cine, LGE | None | Modified JMHW (2006) | 17 | 0 | 2 | 0 | 89 | - |
| Matsumoto et al.99) | 2015 | Japan | 17 | NA | LGE | NA | Modified JMHW (2006) | 7 | 0 | 0 | 10 | 100 | 100 |
| Momose et al.68) | 2015 | Japan | 27 | 1.5T or 3.0T | Cine, LGE | NA | Modified JMHW (2006) | 6 | 21 | 0 | 0 | 100 | - |
| Orii et al.69) | 2015 | Japan | 32 | 1.5T | Cine, LGE, T2WI | None | Modified JMHW (2006) | 32 | 0 | 0 | 0 | 100 | - |
| Simonen et al.70) | 2015 | Finland | 43 | NA | Cine, LGE | None | Own criteria | 33 | 0 | 10 | 0 | 77 | - |
| Tezuka et al.100) | 2015 | Japan | 24 | 1.5T | Cine, LGE, T2WI | None | Modified JMHW (2006) | 15 | 6 | 0 | 3 | 100 | 33 |
| Yokoyama et al.71) | 2015 | Japan | 69 | NA | LGE | None | Modified JMHW (2006) | 24 | 28 | 2 | 15 | 92 | 35 |
| Komada et al.101) | 2016 | Japan | 9 | 1.5T | Cine, LGE | None | JMHW (1993) | 9 | 0 | 0 | 0 | 100 | - |
| Ohira et al.73) | 2016 | Canada, Japan | 30 | 1.5T | Cine, LGE | None | Modified JMHW (2006) | 26 | 0 | 4 | 0 | 87 | - |
| Aikawa et al.102) | 2017 | Japan | 14 | 1.5T or 3.0T | Cine, LGE | None | JSSOG (2015) | 10 | 3 | 0 | 1 | 100 | 25 |
| Kataoka et al.103) | 2017 | Japan | 16 | 1.5T or 3.0T | Cine, LGE | None | Modified JMHW (2006) | 7 | 9 | 0 | 0 | 100 | - |
| Stanton et al.104) | 2017 | Australia | 46 | 1.5T | Cine, LGE, T2WI | None | Modified JMHW (2006) | 2 | 8 | 0 | 36 | 100 | 82 |
| Smedema et al.105) | 2017 | The Netherlands | 40 | 1.5T | Cine, LGE | None | JMHW (1993) | 29 | 0 | 1 | 10 | 97 | 100 |
| Kouranos et al.106) | 2017 | Greece | 321 | 1.5T or 3.0T | Cine, LGE | None | HRS (2014) | 93 | 0 | 3 | 225 | 97 | 100 |
| Yalagudri et al.77) | 2017 | India | 11 | NA | LGE | None | HRS (2014) | 11 | 0 | 0 | 0 | 100 | - |
| Ghanizada et al.107) | 2018 | Denmark | 9 | NA | Cine, LGE, T2WI | None | JMHW (1993) | 9 | 0 | 0 | 0 | 100 | - |
| Muser et al.81) | 2018 | USA | 29 | 1.5T | Cine, LGE | None | HRS (2014) | 26 | 0 | 3 | 0 | 90 | - |
| Vita et al.108) | 2018 | USA | 107 | 3.0T | Cine, LGE | None | HRS (2014) | 51 | 40 | 6 | 10 | 89 | 20 |
| Wicks et al.92) | 2018 | UK | 51 | PET/MR3.0T | Cine, LGE | None | Modified JMHW (2006) | 26 | 6 | 7 | 12 | 79 | 67 |
| Darlington et al.109) | 2019 | Sweden | 42 | 1.5T | Cine, LGE | None | HRS (2014) | 12 | 0 | 0 | 30 | 100 | 100 |
| Divakaran et al.83) | 2019 | USA | 31 | 3.0T | Cine, LGE | None | Explanted heart histology | 1 | 7 | 0 | 23 | 100 | 77 |
| Russo et al.110) | 2019 | Canada | 25 | NA | Cine, LGE | None | HRS (2014) | 10 | 7 | 1 | 7 | 91 | 50 |
| Modified JMHW (2006) | 8 | 7 | 3 | 7 | 73 | 50 | |||||||
| Sgard et al.85) | 2019 | France | 80 | 1.5T | Cine, LGE, T2WI | None | Modified JMHW (2006) | 18 | 16 | 4 | 42 | 82 | 72 |
| HRS (2014) | 34 | 0 | 6 | 40 | 85 | 100 | |||||||
| Zipse et al.87) | 2019 | USA | 104 | NA | LGE | None | HRS (2014) | 36 | 0 | 25 | 43 | 59 | 100 |
| Kawai et al.89) | 2020 | Japan | 52 | NA | LGE | None | JSSOG (2015) | 16 | 16 | 3 | 17 | 84 | 52 |
| HRS (2014) | 9 | 23 | 3 | 17 | 75 | 43 | |||||||
| Miller et al.90) | 2020 | USA | 69 | NA | LGE | None | Modified JMHW (2006) | 8 | 14 | 21 | 26 | 28 | 65 |
| Okune et al.91) | 2020 | Japan | 74 | 1.5T | Cine, LGE | None | JSSOG (2015) | 39 | 24 | 1 | 10 | 98 | 29 |
| Orii et al.111) | 2020 | Japan | 50 | 1.5T | Cine | None | HRS (2014) | 3 | 1 | 5 | 41 | 38 | 98 |
| T2WI | 6 | 2 | 2 | 40 | 75 | 95 | |||||||
| LGE | 8 | 10 | 0 | 32 | 100 | 76 |
CMR = cardiac magnetic resonance imaging; FN = false negative; FP = false-positive; HRS = Heart Rhythm Society; JMHW = Japanese Ministry of Health and Welfare; JSSOG = Japanese Society of Sarcoidosis and Other Granulomatous Disorders; LGE = late gadolinium enhancement; MR = magnetic resonance; NA = not available; PET = positron emission tomography; T2WI = T2-weighted imaging; TN = true negative; TP = true positive.
![]()
Table 6
Diagnostic performance CMR in combination with FDG PET to detect cardiac involvement in patients with sarcoidosis
| Author | Year | Countries | No. | Fasting time | CMR scanner | CMR protocol | Diagnostic criteria (years) | TP (n) | FP (n) | FN (n) | TN (n) | Sensitivity (%) | Specificity (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Matoh et al.58) | 2008 | Japan | 3 | ≥5 | 1.5T | Cine, LGE | JMHW (1993) | 2 | 0 | 0 | 1 | 100 | 100 |
| Ohira et al.59) | 2008 | Japan | 21 | ≥6 | 1.5T | Cine, LGE, T2WI | JMHW (1993) | 8 | 8 | 0 | 5 | 100 | 38 |
| Soussan et al.66) | 2013 | France | 35 | ≥4 | 1.5T | Cine, LGE, T2WI | JMHW (1993) | 10 | 10 | 0 | 15 | 100 | 60 |
| Yokoyama et al.71) | 2015 | Japan | 26 | ≥18 | NA | LGE | Modified JMHW (2006) | 26 | 0 | 0 | 0 | 100 | - |
| Yalagudri et al.77) | 2017 | India | 11 | NA | NA | LGE | HRS (2014) | 11 | 0 | 0 | 0 | 100 | - |
| Wicks et al.92) | 2018 | UK | 51 | ≥12 | Hybrid PET/MR 3.0T | Cine, LGE | Modified JMHW (2006) | 30 | 13 | 3 | 5 | 91 | 28 |
| Divakaran et al.83) | 2019 | USA | 7 | ≥4 | 3.0T | Cine, LGE | Explanted heart histology | 1 | 3 | 0 | 3 | 100 | 5 |
| Sgard et al.85) | 2019 | France | 80 | NA | 1.5T | Cine, LGE, T2WI | Modified JMHW (2006) | 18 | 18 | 4 | 40 | 82 | 69 |
| HRS (2014) | 36 | 0 | 4 | 40 | 90 | 100 | |||||||
| Okune et al.91) | 2020 | Japan | 74 | ≥18 | 1.5T | Cine, LGE | JSSOG (2015) | 39 | 26 | 1 | 8 | 98 | 24 |
| Orii et al.111) | 2020 | Japan | 50 | 1.5T | 1.5T | Cine, T2WI, LGE | HRS (2014) | 8 | 10 | 0 | 32 | 100 | 76 |
CMR = cardiac magnetic resonance imaging; FDG = fluorodeoxyglucose; FN = false negative; FP = false-positive; HRS = Heart Rhythm Society; JMHW = Japanese Ministry of Health and Welfare; JSSOG = Japanese Society of Sarcoidosis and Other Granulomatous Disorders; LGE = late gadolinium enhancement; MR = magnetic resonance; NA = not available; PET = positron emission tomography; T2WI = T2-weighted imaging; TN = true negative; TP = true positive.
![]()
Go to :
COMPUTED TOMOGRAPHY
The disadvantage of MRI is that it is contraindicated for patients with MR unsafe implantable devices or implantable devices. In patients with non-ischemic cardiomyopathy unable to undergo CMR, cardiac computed tomography (CT) can also be used to perform delayed enhancement imaging.112) CT may be advantageous due to its comprehensive systemic evaluation of sarcoidosis. After whole-body scanning, a delayed cardiac scan could be consequently performed even in patients with implantable devices. We reported that the image quality of delayed iodine contrast-enhanced CT (DE-CT) sufficiently allows for the assessment of hyper-enhanced myocardium in patients with or without implantable devices.102)113) DE-CT can also delineate the extent of CS with an accuracy comparable to that of LGE-CMR. 102)
Figure 5 shows a representative case before and after implantation of a cardioverter-defibrillator following DE-CT. Since the contrast noise ratio of DE-CT was relatively lower than CMR, reader experience is required to visually assess the DE-CT results. As observed in 18F-FDG PET,38) objective texture analysis of myocardial DE-CT showed a similar diagnostic value and higher reproducibility for differentiating between CS and non-CS patients compared to visual assessment.114)
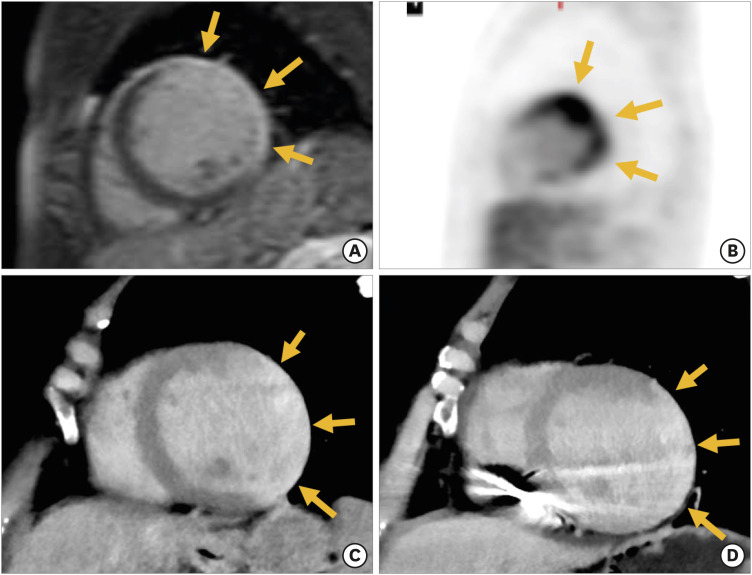 | Figure 5Arrhythmia was detected in a woman in her 50s. Abnormal enhancement and uptake are shown in the left ventricular lateral wall with late gadolinium enhancement of CMR and 18F-fluorodeoxyglucose positron emission tomography/computed tomography (A and B, arrows). DE-CT also highlights the abnormal enhancement in the lateral wall, seen in the CMR (C, arrows). The patient was diagnosed with active cardiac sarcoidosis and was implanted with an ICD to prevent ventricular tachycardia. DE-CT after ICD implantation reveals abnormal enhancement in the lateral wall, as seen previously (D, arrows). Although there were metal artifacts mainly at the septum due to the ICD leads, we were able to compare the 2 images and confirm that the lesion was not worsening over time.CMR = cardiac magnetic resonance imaging; DE-CT = delayed iodine contrast-enhanced computed tomography; ICD = implantable cardioverter-defibrillator.
|
Go to :
 XML Download
XML Download