

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Despite great advances in medicine, cancer continues to be one of the leading causes of death in developed countries. Recently, immunotherapy has been used with great success in previously resistant cancers. The idea of weaponizing the native immune system to fight disease has been explored for centuries, dating back to the early 17th century Qing dynasty when patients were inoculated with the variola minor virus to prevent smallpox.1) Applications to cancer treatment began in the late 19th century, when Dr. William Coley injected formulations of Streptococcus pyogenes into cancers to achieve remission.2) Modern tools have further enabled clinicians to identify specific “immune checkpoints” that tumor cells use to avoid the immune system, thus allowing the development of therapies to target these checkpoints and block tumor escape.
Immune checkpoint inhibitors (ICI) approved to treat cancer target three immune checkpoints: cytotoxic T-lymphocyte-associated antigen 4 (CTLA-4), programmed cell death receptor-1 (PD-1), and programmed cell death ligand-1 (PD-L1). By suppressing these checkpoints, ICIs can trigger immune system pathways to increase T cell activity and inhibit tumor cell survival.
As with most therapies, ICIs are not without risk. These agents have been associated with various immune-related adverse events (irAEs). The most common side effects include colitis, hepatitis, dermatitis, pneumonitis, and endocrinopathies. Cardiovascular toxicities are less common but are of paramount importance due to their potentially life-threatening presentation. As the use of ICIs continues to grow, physicians will have to become more familiar with the diagnosis, monitoring, and treatment of ICI-associated cardiotoxicities.
Go to : 
MECHANISMS
The native immune system uses various suppressive molecules and receptors to maintain normal T-lymphocyte function while preventing autoimmunity. Normally, T cells can identify non-self-antigens presented by antigen presenting cells (APCs) via costimulatory receptor B7 to the costimulatory receptor CD28 on T cells, leading to the activation of an immune response. A coinhibitory receptor on the T cells known as CTLA-4 inhibits the T cells and down-regulates the immune response. CTLA-4 has a higher affinity for costimulatory receptor B7 on APCs than the T cell costimulatory receptor CD28.
Tumor cells escape immune surveillance by utilizing these immune checkpoints. These specific checkpoints inhibit the activation of T cells through CTLA-4 and downregulate tumor cell apoptosis and conversion to regulatory T cells by binding of PD-1 and PD-L1 (Figure 1A). Due to the role of PD-L1 in B7 inhibition, there is also a shared characteristic between CTLA-4 and PD-1.
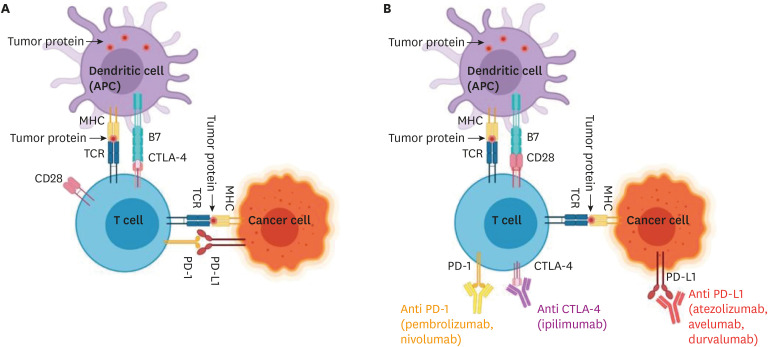 | Figure 1(A) Mechanism used by the tumor cells to evade the immune system. (B) Mechanism immune checkpoint inhibitors use to inhibit the tumor cells from evading the immune system.ACP = antigen presenting cells; CTLA-4 = cytotoxic T-lymphocyte-associated antigen 4; MHC = major histocompatibility complex; PD-1 = programmed cell death receptor-1; PD-L1 = programmed cell death ligand-1; TCR = T-cell receptor.
*Created with BioRender.com.
|
These immune checkpoints have been identified as targets to remove the inhibition of antitumor T cell responses. ICIs work mainly by binding and inhibiting these receptors, enabling activated immune responses against tumor cells (Figure 1B).
ICI induced cardiotoxicities are likely caused by the deactivation of CTLA-4 and PD-1, which are important in inhibiting T cell response in the cardiac muscle. Usually, these receptors suppress inflammation and prevent cardiac muscle injury associated with inflammatory processes.3)4)
In animal models, CTLA-4 deficient mice develop multi-organ lymphoproliferative diseases within a few weeks of life, including T cell myocarditis.5) Severe dilated cardiomyopathy with troponin autoantibodies were found after knocking out PD-1 receptors in mice.6) Another study evaluated the combination of anti CTLA-4 and anti PD-1 agents in cynomolgus monkeys. These agents stimulated CD4+ and CD8+ T cell infiltration of the monkeys' hearts. These animal studies suggest the important role of checkpoint receptors in regulating autoimmune responses in the heart and help to identify myocardial immune cell infiltration.7)
Similarly, investigations in humans have also revealed decreased thresholds for stimulation of T-cells to self-antigens in the heart.8) Endomyocardial biopsy specimens have shown myocardial T cell infiltration with immunohistochemical staining positive for PD-1 and PD-L1. Johnson et al.9) also found a potentiation of T cells targeting an antigen shared by both the heart and tumor. When T cell receptor sequencing of complementarity-determining region 3 (CDR3) on biopsies from the tumor, heart, and skeletal muscle specimens was performed, there were similar expression of muscle-specific transcripts and high-frequency T cell receptor sequences. The similarity of these tissue histopathologic findings seemed to suggest that T cells may respond to a common presenting antigen in different tissues possibly leading to the development of systemic autoimmune response.9)
ICIs have been found to play an important role in atherogenesis and coronary regulation. In animal studies, PD-1 has been found to promote the regression of proatherogenic T cell responses. Investigators have found that PD-1 knockout mice develop larger atherosclerotic lesions compared to wild type controls.10) This might be due to the ICIs effect on the regulation of proatherogenic T cell immunity by T cell activation causing increased production of interferon γ and tumor necrosis factor α leading to an increased risk of coronary thrombosis.11)
Human histologic studies of coronary vasculature have found differences of immune checkpoint expression in patients with coronary artery disease (CAD). Examination by flow cytometry on 76 patients with CAD and 25 patients without CAD found decreased expression of PD-1 and PD-L1 on peripheral mononuclear cells in the patients with CAD.12) Furthermore, the investigators found the expression of these receptors was remarkably low on T cells and myeloid dendritic cells in patients with CAD when compared to controls. These findings suggest the role of PD-1 and PD-L1 in the regulation of proinflammatory atherogenic signaling.12)
The pathophysiology of other ICI-associated CVAEs, such as hypertension is less clear. A potential mechanism may be related to the upregulation of T-regulatory cells. ICI inhibition allows the native immune system to be activated leading to increased systemic inflammation. Chronic arterial inflammation may contribute to arterial stiffness leading to hypertension in these patients.13)
Go to :
CARDIAC TOXICITY OF IMMUNE CHECKPOINT INHIBITORS MANIFESTATIONS
Myocarditis/cardiomyopathy
Myocarditis presents on a spectrum ranging from mild to severe disease. It can vary from asymptomatic elevations in cardiac biomarkers to symptoms suggestive of an acute coronary syndrome, heart failure exacerbation, or severe decompensation with multi-system injury leading to cardiogenic shock and death.9)14)15)16) The classification of myocarditis follows the clinical practice guidelines for the management of irAEs according to the American Society of Clinical Oncology.17)
The time to presentation of symptoms from receiving therapy varies, but median latency between receiving ICIs and developing myocarditis has been reported to be approximately 17 days (range, 13–64 days).9) However, there have been reports of myocarditis developing beyond 32 weeks after starting treatment.18)
Although traditional cardiac risk factors have not been clearly linked to the increased development of ICI-associated myocarditis, limited studies have shown that diabetes mellitus (DM), obstructive sleep apnea (OSA) and elevated body mass index (BMI) may lead to worse outcomes particularly in patients receiving combination therapy.19) There is conflicting evidence regarding previous cardiovascular disease as a potential risk factor for developing myocarditis. In a small case series of 24 patients, there was no clear cardiovascular disease or cancer-type predisposing patients to myocarditis.9) However, in a case series of 8 patients with myocarditis, 5 had cardiovascular disease before receiving ICIs.8)
The incidence of ICI-associated myocarditis is reported to be approximately 1–2%. In a registry derived from 8-centers, the overall incidence of myocarditis after ICI therapy was ~1% with approximately 0.5% with a major adverse cardiovascular event (MACE). Most of the reported myocarditis cases involved anti-PD-1 therapy with 1.3% using pembrolizumab and 0.4–0.6% with nivolumab use.20)21) The combination therapy of anti-PD-1/anti-CTLA-4 has been reported with even higher prevalence of myocarditis (2.4%) and has also been shown to present with more severe cases of myocarditis. In a study comparing the combination of nivolumab and ipilimumab versus single agent nivolumab, the rates of severe myocarditis were 0.27% vs. 0.06%, respectively.9) The low incidence and high mortality observed in myocarditis compared to other immune-related AEs may be due to the difficulty in diagnosis of myocarditis and the possibility of reporting bias.
Pericarditis/pericardial effusion
After ICI initiation, patients can develop pericardial effusions with or without pericarditis.24) ICIs have been reported to cause persistent pericardial and pleural effusions.25)26) In a study at MD Anderson Cancer Center, 1075 patients received ICI treatment between 2015–2017 with baseline echocardiograms demonstrating no pericardial effusions. After initiation of treatment, 78 patients (7.3%) developed pericardial effusions. These patients were found to have higher rates of mortality compared to those who didn't develop pericardial effusions, 58% versus 35%, respectively. A lower body surface area, history of heart failure, elevated troponin levels, low platelet counts, and hyperlipidemia were independent risk factors found to be significantly associated with a higher rates of pericardial effusion development.27)
The presence of a pericardial effusion is one of the supporting diagnostic criteria for myocarditis per the 2013 guidelines of the European Society of Cardiology.28) ICI-associated pericardial effusions may be due to underlying myopericarditis however, it is well known that many malignancies, especially lung, breast, and lymphomas, may independently be associated with pericardial effusions. Hence, patients with new or progressing pericardial effusions should be evaluated for ICI-induced myocarditis, which require additional diagnostic evaluations for confirmation.
Arrhythmias/heart block
Arrhythmia and heart conduction abnormalities are common AEs of ICIs; they include atrial fibrillation, ventricular tachyarrhythmias, and atrioventricular conduction disorders.29) Other electrocardiographic findings from ICI therapy include PR interval prolongation, and right or left bundle branch block.8)9)30) ICI-associated conduction abnormalities can be attributed to coexisting myocarditis due to immune cell infiltration in the conduction nodes, suggestive of T-cell-mediated cytotoxicity.9) This may not explain all cases of conduction abnormalities as was demonstrated in another study showing conduction disease without concomitant myocarditis in 13% of patients receiving ICI treatment.29)
When compared to conduction abnormalities due to other causes, ICI-associated conduction abnormalities are reported to cause worsening cardiovascular mortality (80% vs. 16%, respectively).29) Therefore, surveillance electrocardiograms (ECG) in patients who complain of symptoms of palpitations, dizziness, or syncope while receiving ICI treatment is recommended.
Acute coronary syndrome/coronary spasm
Effects of ICI treatment on coronary vasculature has also been implicated in limited reports. In a pharmacovigilance database of 820,571 patients receiving ICI therapy, 3,773 had immune related adverse events, of which 26 were reported as cardiovascular events. Among these 26 cases, 10 were reported as ACS with 4 cases of acute thrombosis seen on coronary angiography.31)
Inflammation of preexisting atherosclerotic disease from immune system activation has been known to trigger fibrous cap rupture, acute coronary thrombosis, and myocardial infarction. Release of pro-inflammatory cytokines also contribute to the destabilization of coronary lesions.11)
ICIs have also been reported to cause coronary spasm. In reported cases, after administration of ICI therapy, patients presented with chest pain on rest which improved immediately after receiving sublingual nitroglycerin, steroids, and immunomodulatory therapy.32) Coronary angiography demonstrated coronary spasm that resolved after intracoronary nitroglycerine injection. These patients had normal echocardiograms and no obstructive CAD.32)33) Although the exact mechanism of ICI induced coronary spasm is unknown, in the absence of atherosclerotic disease, ICIs have been postulated to cause a T cell-mediated coronary vasculitis.22)34)
Hypertension
ICI-associated hypertension (HTN) is a rare cardiotoxic event with few published reports. This CVAE has been noted in certain PD-1 (pembrolizumab, toripalimab, camrelizumab, sintilimab) and PD-L1 inhibitors (atezolizumab). In a phase 1 trial of pembrolizumab, 2 out of 101 patients developed HTN.35) In a 5-year follow-up study, only one additional case of HTN was reported.36) Early retrospective studies are consistent with these findings, reporting HTN in 1 out of 496 patients taking pembrolizumab, which occurred within 2 weeks of ICI therapy and resolved with systemic antihypertensive therapy.20) Three phase 3 trials comparing pembrolizumab vs. platinum-based chemotherapy did not document any ICI-associated HTN.37)38)39) The World Health Organization (WHO) global database of individual case safety reports from 1967 to 2018 revealed HTN and related end-organ damage in 198 out of 31,321 (0.63%) patients treated with ICIs.22)
Since 2018, recently approved PD-1 and PD-L1 inhibitors have documented higher rates of HTN. A retrospective single-center cohort study of toripalimab, camrelizumab, and sintilimab treatments found 13 out of 70 patients developed HTN.40) Atezolizumab was also found to have higher rates of HTN in two phase 1 trials where 11 out of 110 patients developed HTN.41)42)
Go to :
DIAGNOSIS
The diagnosis of ICI-associated myocarditis is based on clinical presentation and diagnostic testing including laboratory studies, cardiac imaging, and endomyocardial biopsy.
Initial workup for patients with symptoms concerning for ICI-associated myocarditis should include a 12-lead ECG, serum troponin, brain natriuretic peptide (BNP), and echocardiogram. High clinical suspicion may require additional testing including cardiac catheterization with endomyocardial biopsy and/or cardiac magnetic resonance imaging (MRI).17)21)
The diagnosis of ICI-associated myocarditis in the setting of clinical symptoms with elevated cardiac biomarkers and/or new ECG findings such as frequent ventricular ectopy or heart block should also include at least one of the following criteria:
1) appropriate histopathological evidence on endomyocardial biopsy (EMB).
2) imaging features on cardiac magnetic resonance imaging (CMR) by Lake Louise Criteria.
3) new-onset wall motion abnormalities (WMAs) on echocardiography in the lack of other clear etiologies such as obstructive CAD.
Laboratory studies
Myocarditis is often initially suspected by disproportionate elevations in cardiac serum biomarkers. Although cardiac biomarkers are not highly specific for myocarditis, they are widely available and easier to obtain than most other cardiac tests. Thus, they are often useful as an early diagnostic study in the evaluation for suspected ICI-induced myocarditis. In a case control study, troponin T was elevated in 94% and NT-proBNP was elevated in 66% of ICI-induced myocarditis cases.21) In a separate case series, troponin I was elevated in 46% of cases, and BNP or N-terminal proBNP levels were elevated in 100% of cases.29) The level of troponin increase may depend on the timing of measurement as well as the severity of myocardial injury.43)
Currently, troponin is considered a marker for myocarditis however BNP is a marker of left ventricular (LV) dysfunction and acute cardiac stress. BNP has poor specificity as it may be elevated at baseline in cancer patients due to cancer-related inflammation.44) Cardiac troponin is commonly measured as troponin I or troponin T. Cardiac troponin T has been shown to occasionally be elevated from myositis. For this reason, troponin I may be helpful for correlating cardiac injury when overlap with myositis is present after ICI therapy.45)
The elevation of these biomarkers may also indicate a worse prognosis of the myocardial injury. In a case control study, the elevation of cardiac troponin T level was associated with a higher risk of CVAEs.21) Furthermore, the decrease in serum biomarkers may be helpful in following the clinical course of patients receiving anti-inflammatory treatment and heart failure therapy.46)
Electrocardiogram
Myocarditis may also cause disturbances of cardiac electrophysiology. When the inflammatory process reaches the conduction system, electrocardiographic changes may demonstrate intraventricular conduction delay, PR prolongation, or even advanced heart block.9) ICI-induced myocarditis may also present with many types of arrhythmias including atrial fibrillation and ventricular ectopy leading to ventricular tachycardia or fibrillation.29)
Transthoracic echocardiogram
ICI-associated cardiotoxicity may cause a reduction in the left ventricular ejection fraction (LVEF) which can account for approximately 46% of patients who develop myocarditis.47) Transthoracic echocardiography can reveal dilation of cardiac chambers, regional WMAs, or diffuse left-ventricular systolic dysfunction. However, a normal ejection fraction does not rule out ICI-associated myocarditis. Preservation of normal cardiac chamber sizes may be indicative of an acute process, while remodeling and dilatation may represent a subacute or chronic process.
Speckle tracking has also been used to monitor cardiotoxicity in cancer patients receiving various treatments. Although global longitudinal strain (GLS) use in ICI therapy is limited, in a recent case control series, 101 cases with ICI myocarditis were found to have decreased GLS (14.1 to ±2.8) compared to 92 control subjects who received ICI but didn't develop myocarditis. In cases of both preserved or reduced LVEF, GLS was lower among confirmed myocarditis cases.48)
Cardiac magnetic resonance imaging and fluorodeoxyglucose-positron emission tomography computed tomography
When available, CMR is more sensitive than echocardiography for the detection of myocarditis as it provides tissue characterization with precise criteria for the diagnosis of myocarditis.49) The updated Lake Louise Criteria can be used to diagnose myocarditis if one of the main criteria or two supportive criteria are positive.
The main criteria include evidence of myocardial edema (either by regional elevated values by T2-mapping or high signal in T2-weighted images) or evidence of non-ischemic myocardial injury (either by regional elevated values by T1 mapping or presence of late gadolinium enhancement [LGE]). Supportive criteria include signs of pericarditis or systolic dysfunction with regional or global WMAs, although most cases maintain a preserved LVEF.8)49) Having both main criteria increase specificity, and in our institution, we require both to diagnose ICI-associated myocarditis with CMR.
A potential limitation of CMR lies in its sensitivity to detect ICI-associated myocarditis. In a case control study, CMR was able to detect myocardial edema in only one-third of cases.21) This was also shown in an international registry study, where the absence of LGE did not exclude ICI-associated myocarditis when compared to histological findings in endomyocardial biopsies. Also, presence of LGE did not predict cardiovascular outcomes in patients with confirmed ICI-associated myocarditis by biopsy.50)
When CMR is not available or contraindicated, a cardiac FDG-PET-CT may be performed to assess myocardial inflammation. The patient must be able to be on a high fat-low carbohydrate diet prior to the FDG-PET-CT for optimal imaging preparation. FDG-PET-CT findings may improve the sensitivity for mild or borderline myocarditis and increase specificity for chronic myocarditis.51) If a CMR (or FDG-PET-CT) is positive for myocarditis, diagnosis may be sufficient to proceed with treatment, but if the study is negative for myocarditis, the next step in the diagnostic pathway should be an endomyocardial biopsy.34)
Endomyocardial biopsy
Aside from autopsy, EMB is considered the gold-standard procedure to diagnose ICI-associated myocarditis. Given its invasive approach, it should be performed at high volume centers with experienced operators and interpretation of results performed by pathologists familiar with diagnosing myocarditis and/or heart transplant rejection. Pathologic diagnosis of myocarditis may be made based upon the Dallas criteria. Definite myocarditis is demonstrated with the presence of inflammatory cells in the myocardium with necrosis and/or degeneration of adjacent myocytes. Borderline myocarditis may be diagnosed when the infiltrate is sparse, or myocyte injury is not present. In a study of 38 cases of autopsy proven myocarditis, the sensitivity and specificity of EMB were 60 and 80%, respectively.52) The sensitivity of EMB may be limited due to the focal and transient nature of inflammatory cell infiltrates.52)53)54) Due to the patchy nature of inflammatory infiltrates, obtaining multiple samples (≥4) is recommended when performing EMB from either a right ventricular or LV approach. With this understanding, EMB results should be corroborated with clinical suspicion and other diagnostic tests such as CMR.
In a series of 35 cases with ICI-associated myocarditis, 11 had a cardiac biopsy or autopsy. Findings demonstrated patchy and diffuse lymphocyte infiltration within the myocardium with histopathologic findings of T cells, mainly CD4+ and CD8+, with mild to moderate fibrosis in the areas of inflammation.55) PD-L1 staining was positive on the membrane of cardiomyocytes however it is unknown whether PD-L1 staining is specific for ICI induced myocarditis or present in other forms of cardiac injury as well. Of note, there were no granulomas or giant cells as would be observed in acute allograft rejection after cardiac transplantation.
Go to :
MANAGEMENT
The management of ICI-associated cardiotoxicity begins with early hemodynamic stabilization and symptom mitigation. ICI cessation should be considered based on the type and severity of the CVAE.56) Steroids should be administered as first line therapy for most moderate-to-severe ICI-associated cardiotoxicity to alleviate the hyperactive T cell-associated immune response (Figure 2).
 | Figure 2Treatment algorithm of ICI-associated cardiotoxicity by symptom type.ACC = American College of Cardiology; AHA = American Heart Association; ICI = immune checkpoint inhibitor.
*Insufficient evidence to support safety of rechallenging ICI therapy. †Secondary treatments include: infliximab (not to be used in moderate to severe heart failure), anti-thymocyte globulin, mycophenolate mofetil, tacrolimus, intravenous immunoglobulin, plasmapheresis.
|
In ICI-associated myocarditis, ICI treatment should be discontinued to minimize morbidity and mortality.56) High-dose corticosteroids should be administered as recommended by the ASCO/National Cancer Control Network (NCCN) guidelines. Patients should start 1–2 mg/kg of prednisone, intravenously or orally. In severe or refractory cases 500–1,000 mg of intravenous methylprednisolone daily may be administered.17) Upon clinical stabilization, treatment is completed with oral prednisolone at 1 mg/kg daily tapered over 4–6 weeks.34) We recommend the same approach for patients presenting with myopericarditis, which has been shown to be efficacious in limited reports.57)
Second line treatments for steroid refractory patients include infliximab,17)34)58) anti-thymocyte globulin (ATG),18)59)60) tacrolimus,61) intravenous immunoglobulin (IVIG),58)62)63)64)65)66)67) plasmapheresis,58)68)69)70)71)72) and mycophenolate mofetil (MMF).73)74) However, the efficacy of these treatments is primarily illustrated in anecdotal reports and not corroborated through controlled studies.
Infliximab is a chimeric monoclonal antibody that binds to and neutralizes tumor necrosis factor-α, a key cytokine that modulates the body's immune response. For this reason, Infliximab is often utilized in a variety of autoimmune diseases, as well as ICI-associated colitis and pneumonitis. Recent reports document successful use in myocarditis, but physicians should be wary of its contraindications in moderate-to-severe heart failure (NYHA III-IV) at doses greater than 5 mg/kg which have been associated with increased hospitalizations, morbidity, and death.75)76)
ATG and tacrolimus are commonly used treatments in cardiac allograft rejection that have been repurposed for use in ICI-associated myocarditis. ATG is an animal derived antibody that directly targets human T cells, while tacrolimus inhibits calcineurin, a molecule that promotes development of T cells. Some cases of ICI-associated myocarditis have shown some benefit with the addition of ATG or tacrolimus as second line treatments with steroids. As in cardiac allograft rejection they are believed to deplete multifocal lymphocytic and histiocytic infiltrates.59)60)
IVIG is derived from the plasma of human donors and treats inflammatory disorders through the interaction of the exogenous antibodies with the recipient's immune pathways. The immunoglobulins are thought to act through a combination of T/B cell, complement pathway, cytokine and Fc Receptor inhibition. IVIG has had some success as second line therapy in both early and late onset ICI-associated myocarditis, with improvement of reduced ejection fraction, new arrhythmias and WMAs.63)64)65)66) Although steroid monotherapy continues to be the most common initial treatment, some reports using the initial combination of steroids and IVIG has been shown to be well tolerated for patients with mild-to-moderate myocarditis.63)
Plasmapheresis may be used after failure of IVIG therapy or may be started as its own second line therapy following steroid treatment failure. Plasmapheresis is an extracorporeal treatment that selectively removes abnormal cells or substances in the blood. For ICI-associated myocarditis, this includes targets such as autoantibodies or the offending medications. In one case, serum levels of Pembrolizumab were shown to drop from 10,200ng/mL to 3340ng/mL after 2 cycles of plasma exchange.68) This is owed to the fact that antibodies, such as Pembrolizumab, are excellent targets as they are primarily intravascularly distributed in the body. This treatment has produced recovery of baseline cardiac function in several reported cases.68)69)70)71)72)
Interestingly, initiation of steroids and IVIG or plasmapheresis may be strongly considered when patients present with a combination of myasthenia gravis, myositis and myocarditis. These constellation of immune events are quite common in ICI-associated myocarditis, with patients often presenting with ptosis, muscle weakness, and elevated troponins.65)66)67)70)72)77)78) In the overlap of these symptoms, patients have benefited receiving steroids with either IVIG or plasmapheresis on presentation.65)66)70) Rituximab, a monoclonal antibody which targets the CD20 surface antigen of B cells, is another treatment which may also be useful in myocarditis patients presenting with myasthenia gravis. In a small case series it was shown to be effective in six of nine patients presenting with ICI-associated myasthenia gravis.79) Thus, rituximab may be a preferred secondary treatment option in ICI-associated myocarditis patients presenting with myasthenia gravis.
Re-initiation of ICI therapy is generally not recommended for ICI-associated myocarditis. For asymptomatic patients who have had complete clinical recovery, cardiologists and oncologists may consider rechallenging, but currently there is sparse data to support and guide these recommendations.
Treatment of other ICI-associated CVAEs including heart failure, acute coronary syndromes, arrhythmias and HTN may not require steroids and are centered around conventional cardiac therapy. ICI-associated heart failure often occurs in the setting of myocarditis, such that treatment similarly begins with suspension of ICIs17) and management of ICI-associated myocarditis. Management of heart failure and acute coronary syndromes should follow guidelines outlined by the American College of Cardiology/American Heart Association (ACC/AHA). These include intravenous diuretics, inotropes, afterload reduction and guideline directed medical therapy (ACE-Is, angiotensin II receptor blockers, beta blockers, spironolactone) for heart failure.80) In steroid refractory patients, caution is again warranted with infliximab in patients with moderate-to-severe heart failure. For acute coronary syndromes or coronary spasm, urgent cardiac catheterization with percutaneous intervention and anti-thrombotic therapy may be indicated.81)82)
Treatment of ICI-associated arrhythmias also begins with suspension of ICIs. Permanent cessation of the ICI can be coordinated between the cardiologist and oncologist on a case-by-case basis, depending on the clinical severity and response to treatments. Otherwise, following the ACC/AHA guidelines for supraventricular and ventricular arrhythmias are indicated. Bradyarrhythmias and advanced atrioventricular blocks may require temporary or permanent pacemaker placement.83)84)
Lastly, new onset HTN can be generally managed with blood pressure medications in most patients. Given the unknown time course of HTN on prolonged ICI therapy, the established blood pressure goals by age group are appropriate. However, if the blood pressure remains stable without end-organ damage, cessation of ICI therapy is generally not required in these patients. Steroids can be administered in both ICI-associated arrhythmias and HTN if symptoms are resistant to maximal therapy or signs of end-organ injury occur.
Go to :
EMERGING THERAPIES
New targeted therapies under investigation include CTLA-4 agonists (abatacept) and CD52 antibodies (alemtuzumab). CTLA-4 agonists negate the immunostimulatory effects of PD-1, PDL1 and CTLA-4 inhibition by decreasing CD28/B7 T cell co-stimulation upstream.85) Abatacept is more commonly used in rheumatologic disease but targeting this pathway in ICI-associated myocarditis has been shown to be effective in animal studies and limited human case reports. Mouse models of ICI-associated myocarditis had significant decreases in myocardial immune infiltrates to near baseline after 14 weeks of treatment with abatacept.86) These mice also had significant mortality reduction compared to the untreated control group. Two case reports have described abatacept use in fulminant refractory ICI-associated myocarditis. The first case prescribed abatacept following the failure of steroids and MMF,87) while the other case used steroids and plasmapheresis.88) Due to lack of treatment response in both cases, abatacept was administered resulting in significant improvement of troponin levels, ventricular hyperexcitability and myositis symptoms (muscle weakness, facial paralysis).22)87)88) Abatacept is also well tolerated. A controlled trial (n=3,210) of abatacept in rheumatoid arthritis found 51.8% adverse events in the treatment group vs. 46.4% in the placebo group.89) The most frequent reported side effects were headache, nausea, and upper respiratory tract infections, leading to discontinuation in 3.3% of abatacept treated patients vs. 2.0% of placebo treated patients.90) Of note, all biological disease-modifying anti-rheumatic drugs (bDMARDs) carry a low risk of malignancy which can be of some concern to oncologists (0.22% incidence rate during treatment), however, abatacept has not been associated with an overall increased risk of cancer compared to other bDMARDs. Analyses by specific cancer type did show an increased odds ratio for melanoma (1.58 [95% confidence interval, 1.17–2.08]) when compared to other bDMARDs.90)
Another potential treatment that has been investigated for use in ICI myocarditis is Alemtuzumab, a CD52 monoclonal antibody that activates complement pathways of T cell depletion. It is effective in treatment of refractory transplant myocarditis which shows similar histopathological features of lymphocytic infiltration as found in ICI-associated myocarditis.91) In a case report of treatment resistant ICI-associated myocarditis,78) a 71-year-old woman presenting with myositis -myasthenia gravis syndrome and myocarditis received methylprednisolone, MMF, plasmapheresis and rituximab which failed to clinically improve her condition. Alemtuzumab was given as a single dose, resulting in resolution of her cardiac arrhythmias, ventricular dysfunction and abnormal lab findings. Given its limited reported use in ICI-associated myocarditis treatment, additional clinical trials will be needed to characterize efficacy and adverse events. In the interim, all second line treatments should be closely monitored for potential side effects including worsening heart failure, increased risk of infection and tumor growth.92)
Go to :
SURVEILLANCE
There is currently no unified approach in monitoring patients starting ICI therapy. Recommended surveillance strategies have been proposed utilizing best available data. For example, ECG and troponin monitoring of 76 patients on combination ipilimumab and nivolumab by Lee Chuy et al.93) was not able to detect any myocarditis. However, in patients whom physicians suspect higher risk or greater clinical consequences of myocarditis, case-by-case evaluation for surveillance is reasonable. Johnson et al suggests a baseline ECG and weekly testing of troponin levels during weeks 1 to 3 for patients receiving combination immunotherapy.9) In the majority of patients receiving ICIs who have normal baseline ECG and LVEF prior to treatment, clinical education and monitoring of symptoms is a reasonable approach. The surveillance for high risk patients may include more frequent echocardiogram monitoring for changes in LV function and/or strain, especially in patients with an abnormal LV function at baseline.94) We have proposed a surveillance strategy for patients initiating ICI therapy as seen in Figure 3. With the increased use of ICI therapy, better monitoring and risk stratification will be needed to determine patients suitable for increased surveillance.
 | Figure 3Surveillance and Evaluation of ICI cardiotoxicity.ECG = electrocardiography; FDG = fluorodeoxyglucose; ICI = immune checkpoint inhibitor; LVEF = left ventricular ejection fraction; MRI = magnetic resonance imaging; NT pro-BNP = N-terminal pro B-type natriuretic peptide; PET/CT = positron emission tomography/computed tomography; TnI = troponin I.
*Patients with diabetes mellitus, obstructive sleep apnea, elevated body mass index, abnormal LVEF on baseline echocardiography, previous cardiovascular disease or combination therapy (including chemotherapy with cardiovascular side effect).
|
Less severe side effects, such as HTN, may not require monitoring outside of routine clinic visits and home blood pressure measurements. Upon development of symptoms, more extensive workup as outlined above is carried out and directed by a consultant cardiologist.
Go to :
PROGNOSIS
In contrast to its low incidence, ICI-associated myocarditis has generally been associated with high rates of morbidity and mortality. Data from the Bristol-Myers Squibb registry reported a mortality rate of 33%.9) A multicenter registry reported that 46% of patients diagnosed with myocarditis experienced a MACE, defined as the composite of cardiovascular death, cardiogenic shock, cardiac arrest and hemodynamically significant complete heart block.21) This was supported in another study from the WHO database which also reported a mortality rate of 46% in all cases of severe ICI-associated myocarditis.23)
Go to :
CONCLUSION
ICI cardiotoxicity is a rare but potentially lethal complication of cancer immunotherapy. Despite the growing use of ICI treatments, our recognition of CVAEs remains based upon clinical suspicion and diagnostic tests with limited sensitivity. Risk factors such as DM, OSA, and a high BMI have shown potentially worse outcomes with ICI-associated myocarditis. Further translational research into the mechanisms of myocardial injury is needed to better identify more specific biomarkers for diagnosis.
Screening and surveillance of patients is crucial prior to ICI therapy. Clinicians should promptly recognize new symptoms and initiate workup based on the type and severity of the adverse effects. Currently available cardiac biomarkers and imaging are helpful in establishing diagnosis but exhibit low sensitivity and may often warrant invasive testing with an endomyocardial biopsy for confirmation. Prompt treatment is centered around high dose corticosteroids with second line therapies being reserved for patients refractory to steroids.
ICI-associated CVAE diagnosis and management is challenging, often requiring expert consultation from those familiar with cardio-oncology practice. Although current guidelines are based on expert opinion and limited case series, investigations are ongoing to establish best practice. Until then, it is important for clinicians to understand the common clinical syndromes of ICI-associated myocarditis and surveillance strategies for monitoring patients receiving ICI therapy. With increased familiarity and education, cardiologists and oncologists can work together to safely deliver what has become the standard of care treatment for previously untreatable advanced malignancies.
Go to :
 XML Download
XML Download