

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Hypertension (HTN) is a prevalent condition, affecting approximately (approx.) 30% of the adult population worldwide. It has been estimated that 7.834 million deaths and 143.037 million disability-adjusted life years in 2015 could be attributed to HTN.1) Also, health-related quality of life for survivors decreases 30–50% following a major event, such as an acute myocardial infarction (MI), angina, or stroke.2) The American Heart Association estimated that coronary artery disease and stroke cost in the United States are United States Dollar (USD) 108.9 billion and USD 53.9 billion each year, respectively, including both direct and indirect costs.3)
Significant evidence has emerged on the benefits of early intervention and proper management for certain non-communicable diseases, including HTN. However, most hypertensive patients are asymptomatic, so that the awareness rate is often far below 50%.4) Therefore, routine screening for high blood pressure (BP) in adults is highly recommended worldwide, including U.S. preventive services task force recommendation statement.5) The high prevalence and need for long term management of HTN raise not only a clinical burden but also a substantial economic burden for patients, population health managers, and governments. Many countries carry out national health screening and emphasize the importance of screening HTN. The screening targets should be established based on each nation's HTN prevalence, healthcare system, socioeconomic status, and cost-effectiveness analysis (CEA).6) In Korea, the national health-screening program controlled by the government at a national level was launched in 1980. Korea is investing more than 700 billion KRW in the national health examination, and many large private medical institutions are expanding their screening competitively in national screening program.7) The national general health screening program of the Republic of Korea (Korean National Health Insurance Service [KNHIS]) provides a free biennial health examination to all KNHIS enrollees aged ≥40 years. It includes body measurements, including single BP measurement, blood and urine tests, chest radiography, and a self-administered questionnaire on health-related behavior.
Screening for HTN might be the most critical and cost-effective component of the general health screening, but only limited data are available on CEA of HTN screening for different target populations or different setting.8)9) Perhaps no one is against the need to measure BP in a health examination. However, it is necessary to discuss whether BP should be measured every year, whether it can be done every 2 years, such as a national examination, or whether different follow-up intervals depending on age will be more cost-effective. In addition, currently, KNHIS HTN screening has a two-step approach. That means if high BP was screened in the first visit, the examinee is recommended to confirm the BP in the second examination on the separate day. Of course, it is medically correct way, but the actual second check-up rate is low, so most of the examinees did not confirm their HTN or not diagnosis even after receiving health examination. According to the KNHIS's yearbook, the KNHIS examination rate increased gradually, with the first examination rate standing at 74.8% percent in 2014, but the second confirmatory examination rate was quite low of 38.2%. Therefore, there is an opinion that confirming the presence of HTN at a first examination might be more beneficial although there is some concern of false-positive diagnosis.
Thus, we evaluated the CEA of HTN screening in the KNHIS and suggested the optimal HTN screening strategy based on the CEA. Therefore, we compared the CEA of conducting a second confirmatory examination versus a non-executive alternative. In addition, because overall effectiveness of HTN screening can be affected by various assumptions, we conducted sensitivity analyses with different values for the key indicators.
METHODS
Ethical statement
The study protocol was reviewed and approved by the Institutional Review Boards with an exemption (E-2103-104-1205).
The cost of case finding
To compute the cost to find a new HTN patient, the probability of the new case detection was calculated by multiplying the annual incidence of HTN by the sensitivity of the examination.
Model structure
As a model cohort, we chose the Korea National Health and Nutrition Examination Survey (KNHANES) data. Currently, HTN screening of the Korean adults 40 years or older is mandatory and performed every 2 years. We also evaluated the cost-effectiveness of beginning screening at age 20. We ran our models separately for ten age-stratified and sex-stratified groups: men and women aged 40–49, 50–59, 60–69, 70–79, and over 80 years. The Korean population structure by age was determined based on the 2015 population census. The comparator groups are those with same age without HTN screening. Therefore, the age of the comparator group is same as the treatment group. Only difference is BP examination.
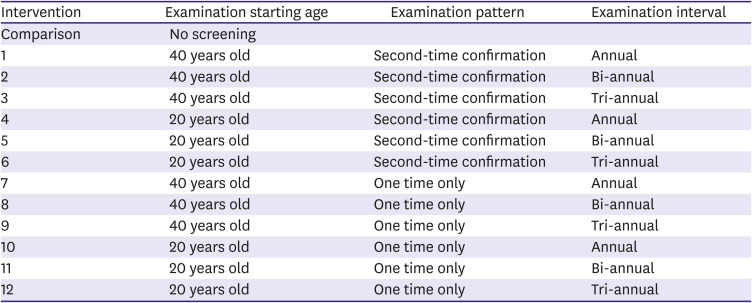
For HTN screening strategy, a Markov decision process model was employed to forecast the costs, complications, and health outcomes associated with HTN. Markov models are a popular form of decision-analytic models which characterize patient cohorts based on a finite number of mutually exclusive and exhaustive “health states”. Under the Markov property, membership of future health states depends only on the current health state, and not on the events that occurred before.10) Movement between health states is defined by “transition probabilities”, which determine the likelihood of a patient moving from one health state to another over a discrete period of time (the “cycle length”).10) Briefly, patients progress through a series of annual, age-specific transition probabilities, over their remaining lifetime, to determine whether they die, have a nonfatal cardiac event, or stay in the current health state. The decision tree for HTN screening compares the 12 HTN screening strategies to the no screening strategy (Table 1).
Table 1
Intervention scenarios and time horizon
In the Markov model, we took into account that people who were not hypertensive on entering the model might become hypertensive over time and incorporated periodic rechecking of BP for a designated time interval. After national health examination HTN screening, the examinees were divided into the suspected HTN and the normotension. Furthermore, the suspected hypertensive examinees went into the second confirmatory examination, either HTN confirmed or finally diagnosed with normotension, or directly took antihypertensive treatment without a confirmatory health examination. The examinees, who took the first screening and the second confirmatory examination, were divided into the treatment and the non-treatment group without medication. The structure of the decision tree on the screening and the treatment for HTN whether with the single screening examination only (Figure 1A) or with the first screening examination followed by the second confirmatory examination model (Figure 1B) were illustrated in Figure 1.
Figure 1
Decision tree and Markov model for estimating the cost-effectiveness of screening for HTN. (A) Structure of the decision tree with the single screening examination only. (B) Structure of the decision tree with the first screening examination and the second confirmatory examination. (C) Different health status in the Markov model.
CKD = chronic kidney disease; HTN = hypertension; MI = myocardial infarction.
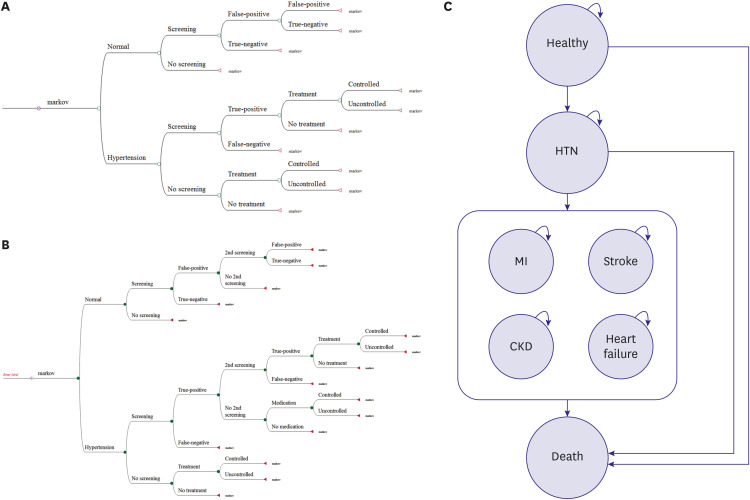
It was assumed that patients could remain in HTN state or move to either acute cardiovascular disease, including MI, stroke, chronic kidney disease (CKD), heart failure, or cardiovascular/non-cardiovascular death. From a stable cardiovascular disease state, patients can experience cardiovascular/non-cardiovascular death or stay in the same health state, or they may have a recurrence of cardiovascular disease and move to acute cardiovascular disease. A Markov simulation model was developed using TreeAge Pro (TreeAge Software, Williamstown, MA, USA). The complete model was illustrated in Figure 1C.
Probability of event
Screening would be performed by office BP measurement in the designated health care facilities. The examination rate was reported as 74.8% in a report from the KNHIS yearbook.11) However, the examination rate of the second confirmatory examination was as low as 38.2%. The sensitivity and specificity of the screening for HTN were estimated at 74.6% and 74.6%, which is derived from the comparison with ambulatory BP monitoring test as the gold standard.9) We assumed the sensitivity and the specificity of the second confirmatory examination as 1.00.
We referred to the prevalence rate, the treatment rate, and the control rate of HTN, as presented in Supplementary Tables 1 and 2. Briefly, the prevalence was about 26.5% (Supplementary Table 1). The health examination structure and age varied the treatment rates; the treatment rate was higher in those who completed the second confirmatory examination than those who did not take health examination at all or who took the first screening only (Supplementary Table 2). Furthermore, the control rates among the overall hypertensive population were 5.1% in 20–39 years old, 40.6% in 40–64 years, and 56.7% for those aged ≥65 years old.12)
The age-specific annual incidence of HTN was derived from the KNHIS-Health Screening Cohort (HEALS).13) The total annual incidence of HTN was about 2%, and the age-specific incidence was presented in Supplementary Table 3. We did not explicitly model repeated events.
The incidence rate of cardiovascular complications and the death rate from cardiovascular complications were also derived from the NHIS-HEALS (Supplementary Tables 4 and 5).13) We chose a composite cardiovascular outcome that included HTN (ICD-10 code, I10.x), CKD (N18.x), MI (I21.x–I24.x), stroke (I60.x–I67.x), and heart failure (I50.x).
Transitional probabilities between health states were obtained from published studies, as summarized in Supplementary Table 6. The probabilities were regarding disease occurrence, developing complications and death. In the model analysis, data on relative risk reduction of complication or death events from hypertensive patients who were receiving medication was also taken into consideration. Baseline probabilities for patients with uncontrolled HTN suffering cardiovascular diseases were derived from a model developed by Lovibond et al.9) Also, age-specific and sex-specific risk reductions with antihypertensive treatment were based on the meta-analysis reported by Law et al.14) We assumed that people with falsely diagnosed HTN gain no benefit from antihypertensive treatment and no harm from unnecessary treatment, which is the same presumption based on the paper by Lovibond, et al.9) A systematic review and meta-analysis comparing the risks associated with uncontrolled (which was assumed to be the same as a placebo scenario) and controlled HTN conducted by the Blood Pressure Lowering Treatment Trialists' Collaboration found that controlled HTN reduced stroke incidence by 30% (95% confidence interval, 0.57–0.85).15)
Costs
We conducted our analysis from a limited societal perspective considering both direct medical costs and indirect social costs. The direct costs associated with HTN were mainly derived from the claims data, including HTN outpatient treatment costs before cardiovascular events (hospital and clinic visits), hospitalization expenses of having cardiovascular events, and subacute care costs (home care and nursing home expenses) after discharge from hospital.
Costing data of BP screening was garnered using a standard questionnaire from medical institutions conducting the national general health screening program of the Republic of Korea.7) The median values of the BP measurement in the first examination and the second confirmatory examination were estimated at 14.8% and 26.3% of the total costs, which were corresponded to 1,083 KRW (approx. USD 0.88) and 4,093 KRW (approx. USD 3.33), respectively (median value).
The direct costs in each health status were obtained from a 2014 data of Health Insurance Review and Assessment Service-National Patient Sample (Supplementary Table 6).16)
Indirect costs included time, transportation, and caregiving costs, which were estimated as Supplementary Table 6. All the costs were expressed in KRW (one USD=1,229 KRW in 2020). We assumed no cost for adverse events of antihypertensive medication due to far better efficacy-versus-adverse events profiles. Discount rates were assumed to be 5%.
The utility of health status and quality of life
We attributed a baseline quality of life weight (utility; 0–1 scale, where 0=dead and 1=full health) based on the literature.9)17)18) According to the previous studies, the quality of life weight for a healthy state and hypertensive state was considered as 1, but that for CKD, MI, stroke, and heart failure was 0.85, 0.76, 0.63, and 0.61, respectively (Supplementary Table 6).
The results of the cost-utility analysis are expressed as the costs, QALY, and incremental cost-effectiveness ratio (ICER). Briefly, QALY is a numerical description of the value, which a medical service can provide a group of patients with similar medical conditions. For example, if an additional year of healthy life is worth a value of 1 (year), then a year of less healthy life is worth less than 1 year.19) ICER is the ratio of the difference in mean costs (cost of treatment–cost of no treatment) and mean effects (effect of treatment–effect of no treatment) between the strategies “treatment” and “no treatment”.20) In order to make costs and effects occurring at different times comparable, the model discounted lifetime costs and QALYs at an annual rate of 5%. Discounting is a method of calculation, which converts the value of future costs and effects into their present value.21) Lastly, tornado diagrams were drawn to display the influence of each model input parameter (TreeAge Pro; TreeAge Software).
Sensitivity analysis
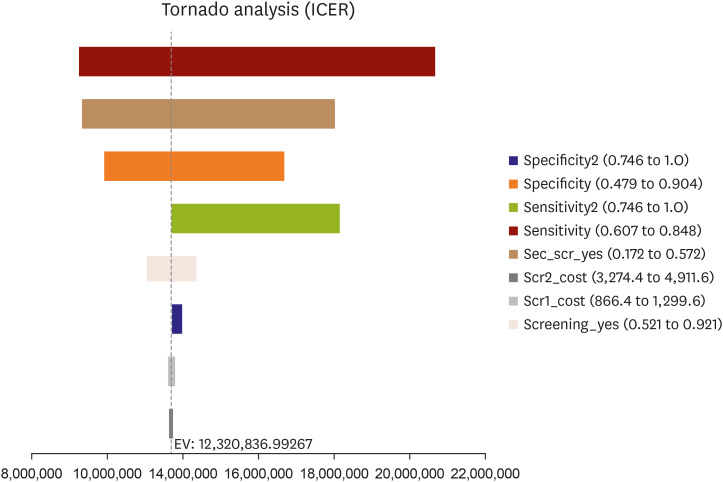
Uncertainty arises because many assumptions are made when estimating the clinical and cost variables used in the analysis model. Therefore, to explore the impact of uncertainty, we performed sensitivity analyses. One-way sensitivity analysis results were presented using a tornado diagram based on the examination cost, the sensitivity/the specificity, and the examination rate of the first and the second confirmatory examinations. We put different values for the examination cost, and the examination rate of the first and the second confirmatory examinations. We also changed the sensitivity/the specificity of the second confirmatory examinations from the current value 1.00 to the input estimates of the first screening examination.
RESULTS
To find one new HTN case, relatively small amount of cost was incurred for the adults aged 40 years or older, and it tends to decrease for older groups: 70,552 KRW (approx. USD 57) for 40–44 years old, 70,551 KRW (approx. USD 57) for 45–49 years old, 41,890 KRW (approx. USD 34) for 50–54 years old, 32,695 KRW (approx. USD 27) for 60–69 years old, 26,284 KRW (approx. USD 21) for 70–79 years old, 29,788 KRW (approx. USD 24) for 80–84 years old, and 29,784 KRW (approx. USD 24) for over 85 years old. However, relatively higher costs of case finding for younger adults are incurred: 446,763 KRW (approx. USD 364) for 20–29 years old, and 167,555 KRW (approx. USD 136) for 30–39 years old.
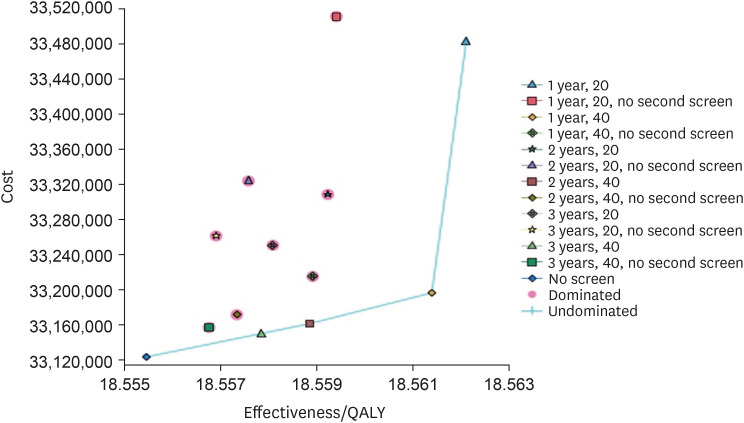
The ICER values for the first screening examination with the second confirmatory examination in the adults 40 years or older every 2 years and the same strategy for the adults 20 years or older every 2 years compared with no screening were 12,171,974 KRW (approx. USD 9,904) and 51,988,319 KRW (approx. USD 42,301), respectively. Among the 12 examination strategies, the ICER values of three strategies of the first screening examination with the second confirmatory examination in adults aged 40 years or older every 3 years, 2 years, or annually were 10,170,333 KRW (approx. USD 8,275), 13,246,000 KRW (approx. USD 10,778), and 19,922,000 KRW (approx. USD 16,210), respectively, which are cost-effective at a Korea willingness-to-pay threshold of 30,000,000 KRW (approx. USD 31,363)/QALY (Korea gross domestic product per capita in 2018, extracted on 6 April 2020 from OECD.Stat) (Figure 2). When we performed the CEA from a payer's perspective which considers only the direct medical costs, the ICER values of the first screening examination with the second confirmatory examination in adults aged 40 years or older or older every year, and the same strategy in adults aged 40 years or older or older were cost-effective at a willingness-to-pay threshold of KRW 30 million/QALY.
Figure 2
ICER of 21 different strategies for hypertension screening.
ICER = incremental cost-effectiveness ratio; QALY = quality adjusted life year.
One-way sensitivity analyses showed that the main drivers for the ICER results were the sensitivity of the first screening examination, followed by the examination rate of the second confirmatory examination (Figure 3). If the second confirmatory examination was not included in the strategies, the specificity of the first screening examination influenced the ICER results (Supplementary Figure 1).
DISCUSSION
The main result of this study was that the routine BP measurement in the national health examination program was a very cost-effective public health strategy. Base case analysis showed that less than 71,000 KRW (approx. USD 58) was required to find one new HTN case by the HTN screening examination for a general population over 40 years old, and the costs became less following the increase of the examinees' ages. Second, the optimal HTN screening strategy based on the CEA was the first screening examination with the second confirmatory examination in the adult population over 40 years per 3 years. If the purpose of the BP examination during the national health examination was not to achieve the minimal cost, but to improve the health level of the target population as much as possible within the range of the willingness-to-pay level, the first screening examination with the second confirmatory examination in adults aged 40 years or older per every year might be more effective. The reason why the strategies to adopt the second confirmatory examination adding the cost has been more cost-effective, is that the CEA was not just the cost of the screening, but also evaluated the effect of the cardiovascular prevention by adequately diagnosing HTN and rendering the early treatment. Third, the main drivers for the ICER results were the sensitivity of the first screening examination, followed by the examination rate of the second confirmatory examination. Also, if the second confirmatory examination was not included in the strategies, the specificity of the first screening examination influenced the ICER results.
According to the KNHANES, the prevalence of HTN in Korean adults has been stable at 30%. The rates of awareness, treatment, and control of HTN have shown substantial improvements until 2009, however, reached a plateau, and no significant improvements have been observed since 2013.22) Particularly, the young population have shown suboptimal management status.23) While the prevalence of HTN among young adults has increased, the awareness and treatment rates remain low, warranting routine health screening.24)
Previously, several studies evaluated the impact of BP screening. Combining BP screening and self-care education for the elderly population over 65 years old at primary care institutions resulted in a 9% reduction in cardiovascular hospitalization, mainly due to an 11% reduction in hospitalization with MI.25) In Taiwan, adults who took the nationwide periodic health examinations had 72% higher probabilities of antihypertensive treatment, suggesting the benefit of promoting early treatment.26) National Health Service Health Checks program in England reported similar findings that a universal primary prevention program identified a substantial risk factor burden in a population without known cardiovascular disease and suggested early prevention effect in HTN. Regarding CEA, the elderly health examination program in Taiwan was reported to save costs and increase life significantly compared with non-participants.27) In contrast, in adolescents in the United States, population-wide lifestyle modification education such as salt reduction might be more effective than the routine BP screening.28) As presented, previous studies on HTN screening mainly evaluated the partial transition rate to early treatment and did not adequately evaluate the CEA of routine BP screening in the general adult population. Moreover, most studies regarding HTN screening evaluated the clinic-based population-oriented health examination, not government-initiated BP measurement in the general population. However, the cost-effectiveness analyses of HTN screening as a part of national health examination for the general adult population have been limited, especially no data in Korea.
In this CEA, the primary determinant of HTN screening was the accuracy of the BP measurement. The complexity of the BP measurement is that the accuracy was not dependent on the device or the technique but dependent on the examinee's factors such as emotional stress and insufficient resting/stabilization before measurement. Therefore, HTN guidelines recommended the repeated measurement to exclude the false-positive diagnosis of HTN, e.g., white coat HTN. KNHIS examination adopted the second confirmatory examination strategy for the suspected HTN cases in the first screening examination. However, the problem was the low examination rate below 40%. The rest 60% of the suspected cases went two opposite directions. One direction was to visit the medical clinics directly, spending one's own medical cost for HTN confirmation or treatment. The other direction was not to make any confirmatory process or starting treatment but remain in uncontrolled HTN case. Both directions might cause more cost than the HTN screening program at the KNHIS examination. This complexity of the BP measurement well explained why the main drivers for the ICER results were the sensitivity and the specificity of the first screening examination and the examination rate of the second confirmatory examination. As the sensitivity and the specificity of BP measurement cannot be increased to a certain level because the primary determinant is the examinee's factor, not the examiner's factor, KNHIS examination has a strategy of the repeated measurement in the second examination in a separate day. The results of this study indicated that increasing the examination rate in a second confirmatory examination was essential for maximizing the cost-effectiveness of the HTN program.
There was another strategy to confirm the BP by applying the ambulatory BP monitoring in the first screening visit instead of the separate visit because the adherence of the second visit was universally low. Ambulatory BP monitoring is considered as the best single method for diagnosing HTN as recommended in U.S. preventive services task force recommendation statement, even though it causes potential harms associated with sleep disturbance, discomfort, and restrictions in a daily activity besides its costs.5) Lovibond et al.9) suggested that ambulatory monitoring was the most cost-effective strategy for the diagnosis of HTN for men and women of all ages. The main reason is that ambulatory monitoring as a diagnostic strategy for HTN after an initial raised reading in the clinic would reduce misdiagnosis and save costs. Cost savings counterbalance additional costs from the ambulatory BP monitoring from better-targeted treatment. However, the cost of the ambulatory BP monitoring strategy was much higher than the cost shown in this study. Of course, it is unfair to compare the findings of two CEAs performed in different health systems and medical costs. Notwithstanding, the findings of this study suggested that the second confirmatory examination, if being achieved with a high examination rate, could be a practical examination strategy with a higher cost-benefit ratio, especially in low income, low labor cost.
Currently, interests in the screening and management of HTN in younger adults are growing. While the prevalence of HTN among young adults has increased, the awareness and treatment rates remained low.24) Early detection and management of elevated BP in young adults could prevent future cardiovascular events, thus the Korean Society of Hypertension announced the 2020 motto focusing on HTN in the younger generation: 'the earlier, the better' at the beginning of the year.29) It is true that the second confirmatory examination rate was less than 40%, especially in younger population. Therefore, the current national health examination BP screening does not work in confirm HTN in younger population. However, our study showed that an opinion that confirming the presence of HTN at a first examination is not cost-effective due to the considerable risk of false-positive “white coat” HTN. Therefore, we think ambulatory BP monitoring after an initial raised reading in the clinic would be more effective for younger age group rather than to encourage to visit the secondary confirmatory visit, which might be warranted to evaluate in cost-effective analysis in the future.
Our study has several limitations. Firstly, although we tried to utilize national health statistics, some input values were derived from the previous studies done in a different health system. That might not reflect the situation and the effects of the national health examination. Second, this study indicated the examinee's characteristics, such as age, greatly influenced the cost-effectiveness. Among various patients' factors, the BP levels might be the most important determinant of the sensitivity and specificity of HTN diagnosis. If we considered the BP levels in the first examination in this CEA, the results might have more implications in the clinical aspect. However, we could not take the BP levels into account because of the lack of data. Third, we considered four major cardiovascular complications. Although HTN is the crucial risk factor of these cardiovascular complications, other factors such as diabetes mellitus, smoking, or obesity can also influence the outcome. Conversely, other cardiovascular complications, including peripheral arterial disease, can also exert health impact. These factors were not analyzed in this study. The last but essential limitation of this study is that the event rates were derived from the claim data mainly based on the medication prescription. So, there was a possibility of the overestimation of the event rate. The results might overestimate the cost-effectiveness of HTN screening.
In conclusion, HTN screening in a part of the national health examination program was cost-effective, especially in adults over 40 years old. The optimal HTN screening strategy based on the CEA was the first screening examination with the second confirmatory examination in the adult population over 40 years per 2–3 year intervals. The lower ICERs, despite the high prevalence of HTN in Korea, seemed to be attributable to the lower costs of screening and treatment. The study has an important implication for health policymaking as well as the clinical aspect.
 XML Download
XML Download