

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Estrogen is a key regulator of bone metabolism affecting osteoblasts, osteocytes, and osteoclasts. Ultimately, estrogen decreases bone resorption, and maintains bone formation.1 Therefore, estrogen replacement therapy is recommended in postmenopausal women at high risk of fracture under 60 years of age or < 10 years past menopause.2 However, estrogen is associated with a risk of breast cancer or endometrial cancer, so selective estrogen receptor modulators (SERMs), which act as an estrogen agonist or antagonist depending on body tissue, have been developed. SERMs act as antagonists to the breast and endometrium, reducing the risk of breast cancer and not increasing the risk of endometrial cancer. While, SERMs act as an estrogen agonist in bone and have been widely used as a treatment for postmenopausal osteoporosis.3 However, SERMs are also associated with increased venous thromboembolism (VTE) risk, like estrogen. In Women's Health Initiative (WHI) randomized trials, menopausal hormone therapy increased the risk of stroke and VTE.4 Raloxifene was associated with an increased risk of fatal stroke and VTE in previous studies.56 Bisphosphonates (BPs) have been widely used until recently to treat osteoporosis. Because of the possibility of an increased risk of atrial fibrillation with BPs,78 there has been concern about the risk of VTE associated with the use of BPs. Therefore, studies have been conducted on the relationship between use of BPs and raloxifene, and risk of VTE.91011 In a Danish cohort study, alendronate and raloxifene carried the same risk for deep venous thromboembolism (DVT) and pulmonary embolism (PE).9 In Taiwan, the risk of VTE was similar between BPs users and raloxifene users.11 However, there are few reports on the association between VTE and osteoporosis pharmacological treatment in Koreans. Therefore, the aim of this study was to compare the VTE incidence and risk between BPs users and SERMs users in Korean patients with osteoporosis using the Korean National Health Insurance (KNHI) claims database.
Go to : 
METHODS
Study participants and design
This study was a retrospective cohort study. Data were obtained from the KNHI claims database between 2012 and 2016. KNHI service covers 100% of the Korean population. All clinics and hospitals submit patients' information on diagnostic and procedure codes according to International Classification of Diseases, 10th revision (ICD-10) for claim.
Between January and December 2012, women ≥ 50 years of age who were diagnosed with osteoporosis and who were first prescribed BPs or SERMs were enrolled in this study. Osteoporosis diagnosis was indicated by the ICD-10 codes M80.X, M81.X, or M82.X. Patients under 50 years old or who had been prescribed BPs or SERMs, or calcitonin a year before the index date were excluded. Patients diagnosed with cancer or Paget's disease between 2011 and 2016 were excluded. Further, patients who developed VTE within six months of the index date or died within one year of index date were excluded. The remaining individuals were divided into two groups (BP user group and SERMs user group). The SERMs user group was defined as patients who had been prescribed SERMs for at least eight weeks from the index date, had no drug changes from the index date to the end of the study, and had never taken BPs or calcitonin. Moreover, the BP user group was defined as patients who had been prescribed BPs for at least eight weeks from the index date, had no drug changes from the index date to the end of the study, and had never taken SERMs or calcitonin.
The primary outcome was the incidence of DVT or PE. Both groups were followed up for VTE or PE occurrence, death, or until December 31, 2016 (up to four years).
Definition of VTE
VTE included DVT, PE, and other thrombosis. VTE was defined as cases of disease codes (ICD-10 codes: I80.0, I80.2, I80.3, I26.0, I26.9, I82.0, I82.8, and I82.90) in discharge diagnosis, or cases of anticoagulants (warfarin, low molecular weight heparin [enoxaparin], and, heparin) and thrombolytics (urokinase, and alteplase) prescription one or more times during hospitalization, or cases of procedure code (ICD-10 codes: M6632, M6597, O2045, O0218, and O2059) during hospitalization, or cases of warfarin prescription in outpatients.
Other covariates
Age, body mass index (BMI), smoking, and drinking data were obtained from health examination data. Past hospitalization history, duration of drug therapy, history of estrogen or glucocorticoid hormone replacement therapy, major osteoporotic fracture and comorbidities date were collected from claims data. Past hospitalization was obtained for the 12 months before index data. The duration of drug therapy was calculated by cumulative drug usage from the index data to the occurrence of primary outcomes or completion of the study (December 31, 2016). The history of estrogen replacement therapy for at least three months or long-term use of oral corticosteroids (prednisolone or an equivalent medication at dose ≥ 5 mg/day) over three months, and major osteoporotic fracture were investigated from index data to the occurrence of primary outcomes or completion of the study (December 31, 2016). Major osteoporotic fractures were defined by ICD-10 codes (S72.0, S72.1, S22.0, S22.1, S32.0, M48.4, M48.5, S52.5, S52.6, S42.2 and S42.3). Comorbidities were investigated from 12 months before index data to completion of the study (December 31, 2016). The included comorbidities were: varicose vein, inflammatory bowel disease (IBD), atrial fibrillation (AF), diabetes mellitus (DM), hypertension, dyslipidemia, rheumatologic diseases, renal diseases, stroke, and dementia. These diseases were defined by ICD-10 codes.
Statistical analysis
Baseline characteristics of the participants in BP and SERMs user groups are expressed as the mean ± standard deviation (SD) for continuous variables and as percentages for categorical variables. The demographic characteristics and other covariates were compared between the two groups by Student's t-test, Mann-Whitney U test, or χ2 test. The VTE risk in two groups was analyzed via multivariate Cox model. All data were analyzed using the SAS software ver. 9.1 (SAS Institute, Inc., Cary, NC, USA). A P value < 0.05 was considered to reflect significance.
Ethics statement
This study was approved by the Institutional Review Board (IRB) of Wonkwang University Sanbon Hospital (IRB No. WMCSB 201706–64). No informed consent was required from patients due to the nature of public data from KNHI claims database.
Go to :
RESULTS
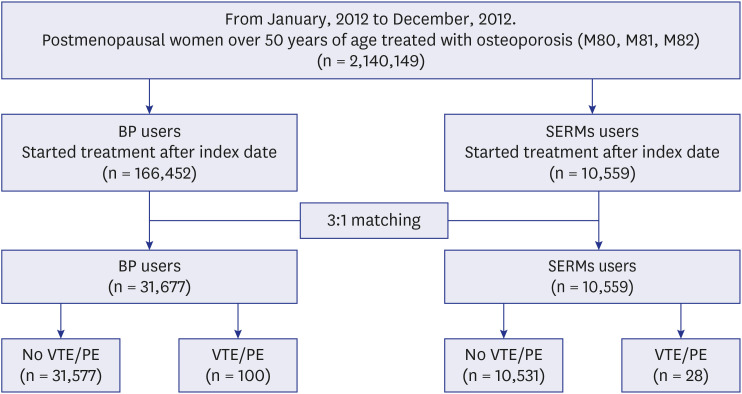
From January to December 2012, women over 50 years of age diagnosed with osteoporosis were extracted. Among them, 166,452 individuals were the first to use BPs after index data, and 10,559 individuals were the first to use SERMs. By 3:1 matching according to age, 31,677 individuals in the BP user group and 10,559 in the SERMs user group participated in this study and were monitored. One-hundred individuals were diagnosed with VTE in the BP user group, and 28 in the SERMs user group, during follow-up period (Fig. 1).
The baseline characteristics of study individuals are shown in Table 1. The mean follow-up period was 1,644 ± 137 days in the BP user group and 1,624 ± 144 days in the SERMs user group. The mean age was 64.1 ± 8.1 years in the BP user group and 63.8 ± 8.1 years in the SERMs user group. Mean BMI was 23.71 ± 3.10 kg/m2 in the BP user group and 23.53 ± 3.10 kg/m2 in SERMs user group. More obese individuals and drinkers were present in the BP user group than the SERMs user group (P < 0.001 and P = 0.013, respectively). More individuals had estrogen replacement therapy for at least three months in the SERMs user group (P < 0.001). More individuals had DM, dyslipidemia, renal disease, rheumatologic diseases, and dementia in the SERMs user group (P < 0.05). Inflammatory bowel disease was more commonly observed in the BP user group (P = 0.001). During the follow-up period, more major osteoporotic fractures occurred in the BP user group (P < 0.001), while more had past hospitalization history in the SERMs user group (P < 0.001)
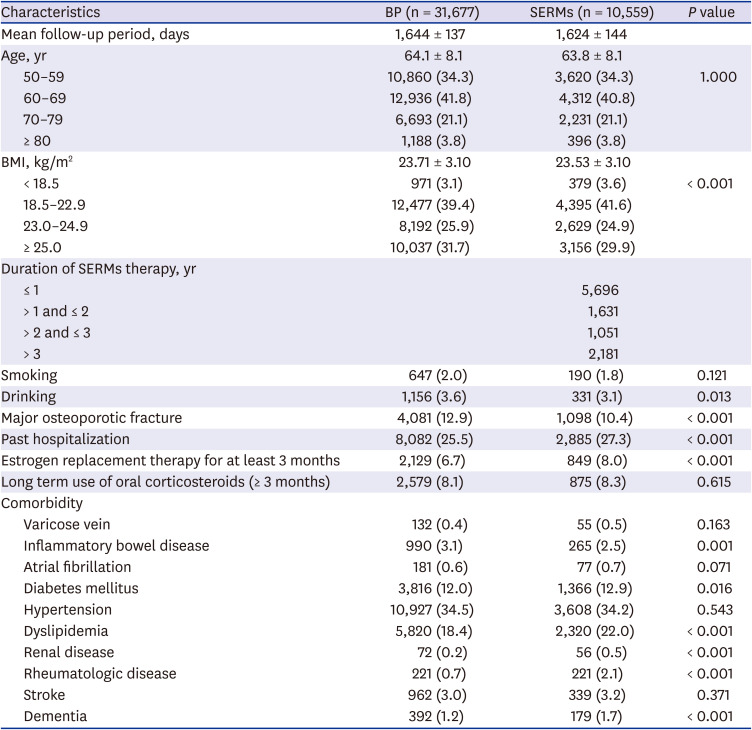
Table 1
Baseline characteristics of the study subjects
Data are shown as mean ± standard deviation or number (%). By Student's t-test or Mann-Whitney U test, χ2 test.
BP = bisphosphonate; SERMs = selective estrogen receptor modulators, BMI = body mass index.
![]()
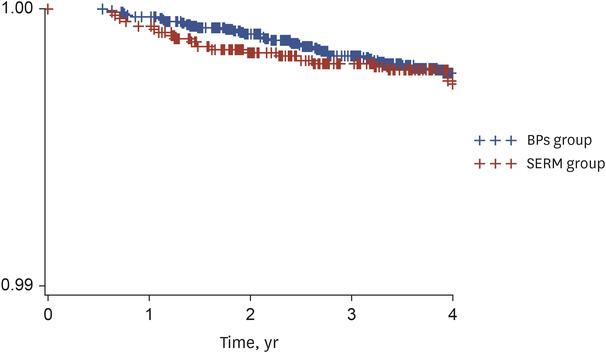
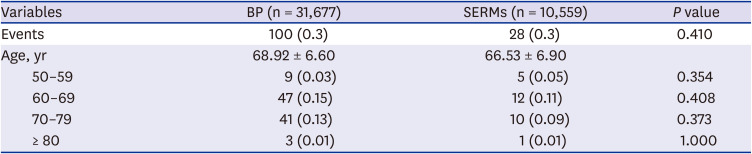
The incidence of VTE between the two groups was not different (Table 2). Kaplan-Meier curves for comparing time to VTE in the SERMs and bisphosphonate groups is shown in Fig. 2.
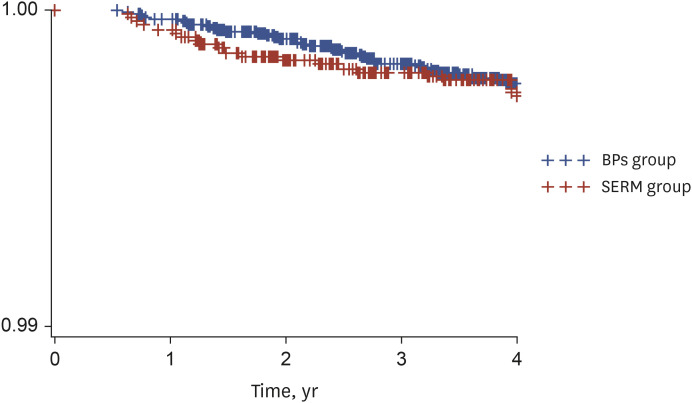 | Fig. 2Kaplan-Meier curves for comparing time to VTE and PE in the SERM and bisphosphonate groups.VTE = venous thromboembolism, PE = pulmonary embolism, SERM = selective estrogen receptor modulator, BP = bisphosphonate.
|
Table 2
Incidence of venous thromboembolism in patients with osteoporosis treatment
Data are shown as number (%). By χ2 test.
BP = bisphosphonate, SERMs = selective estrogen receptor modulators.
![]()
Table 3 shows the hazard ratios (HR) of risk factors for VTE by multivariate Cox model. The HR for VTE was 0.72 (95% confidence interval [CI], 0.40–1.28) in the SERMs group compared to BP group. As age increased, the HR for VTE increased except 80 years of age or older. The HR for VTE was 3.77 (95% CI, 2.07–6.86) in 60–69 years of age, 5.88 (95% CI, 3.14–11.02) in 70–79 years of age, and 2.61 (95% CI, 0.83–8.19) in ≥ 80 years compared to the 50–59 years group. BMI, drinking, smoking, and past hospitalization history did not affect VTE development. Major osteoporotic fracture increased the risk of VTE (HR, 1.77; 95% CI, 1.16–2.70). The risk of VTE increased in participants with atrial fibrillation (HR, 3.31; 95% CI, 1.35–8.11) and rheumatologic disease (HR, 3.61; 95% CI, 1.22–10.6), but other comorbidities did not affect VTE development. Estrogen replacement therapy increased the risk of VTE (HR, 3.40; 95% CI, 2.01–5.73). Glucocorticoid replacement therapy did not increase the VTE risk significantly. Age, BMI, duration of SERMs therapy, smoking, drinking, fracture, and comorbidities did not affect VTE development. However, past hospitalization (HR, 2.24; 95% CI, 1.02–4.92), estrogen replacement therapy (HR, 5.75; 95% CI, 2.29–14.39), and glucocorticoid replacement therapy (HR, 2.71; 95% CI, 1.05–7.0) increased risk of VTE in the SERM group (Table 4).
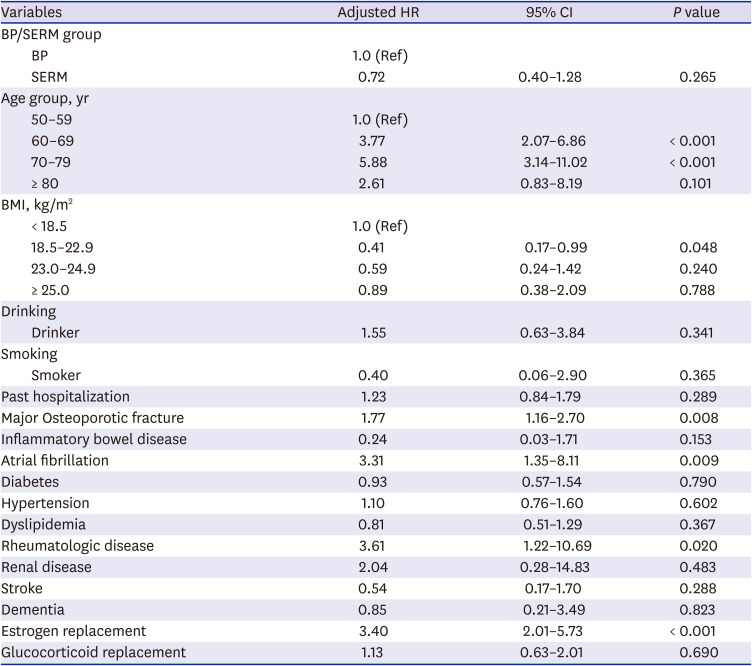
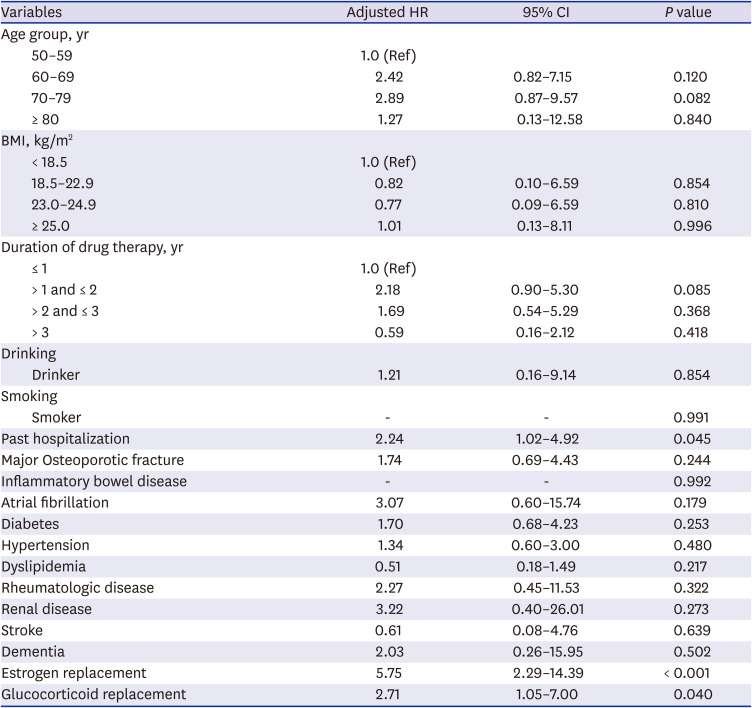
Table 3
Comparison of HR of venous thromboembolism among various risk factors
By multivariate Cox model, adjustment for age, BMI, drinking, smoking past hospitalization, major osteoporotic fracture, history of glucocorticoid or estrogen therapy, and comorbidities.
HR = hazard ratio, CI = confidence interval, BP = bisphosphonate, SERM = selective estrogen receptor modulator, BMI = body mass index.
![]()
Table 4
Comparison of hazard ratio of venous thromboembolism among various risk factors in SERM group
By multivariate Cox model, adjustment for age, BMI, drug of SERM therapy, drinking, smoking, past hospitalization, major osteoporotic fracture, history of glucocorticoid or estrogen therapy, and comorbidities. By Cox proportional hazard model, adjustment for age, BMI, past hospitalization, major osteoporotic fracture, duration of drug therapy, history of glucocorticoid or estrogen therapy, and comorbidities.
SERM = selective estrogen receptor modulator, HR = hazard ratio, CI = confidence interval, BMI = body mass index.
![]()
Go to :
DISCUSSION
Oral contraceptive (OC) use disrupts the balance between the coagulation system and the anticoagulant pathways. OC use increased plasma levels of fibrinogen, prothrombin, coagulation factors VII, VIII, and X and decreased the factor V levels.121314 OC-induced protein S and tissue factor inhibitor reduction could increase activated protein C, resulting in VTE.15 There was no increase of VTE in women using progestogen-only contraceptives. The increased risk of VTE and stroke in patients using SERMs could be explained by these estrogen effects. Currently, SERMs are contraindicated in patients with a history of VTE, when long-term absolute bed rest is required, before and after surgery.
Some previous studies reported that BPs were associated with a high risk of AF and atrial flutter than placebo.71617 The possible mechanism was explained by increased release of inflammatory cytokines. However, BPs were not associated with a higher risk of AF in other clinical trials,181920 and there was no evidence of increased risk of VTE. It is still controversial, but AF is considered as a possible side effect when BPs are prescribed in clinical practice.
As a result of our study, SERMs did not significantly increase the risk of VTE compared to BP in Korean patients with osteoporosis. This finding could be explained by the lower prevalence of VTE in Asians compared to Western populations21 and a selection bias that SERMs were avoided in the VTE high-risk group. Whereas, age, fracture, atrial fibrillation, rheumatoid disease, and estrogen replacement therapy increased the risk of VTE. With aging, comorbidities would increase and physical activity decrease, which might affect VTE development.22 Those over the age of 80 may not have been statistically significant, because a small number of participants were included in this study. Fracture induces immobilization, which could increase the risk of VTE.23 Atrial fibrillation, rheumatoid disease, and estrogen replacement therapy are associated with a hypercoagulable state.2425 In the subgroup analysis conducted only with the SERMs group, past hospitalization history, estrogen, and glucocorticoid replacement therapy increased the risk of VTE. Considering the yearly increasing incidence of VTE in the Korean population,26 SERMs are not recommended in the high risk group for VTE, e.g. those with immobilization or a hypercoagulable state.
In our study, some differences were found between the BP group and SERMs group. Estrogen replacement therapy for at least three months was more common in the SERMs group. This might be because SERMs are commonly used early in menopause. The difference of comorbidities between the BP group and SERMs group might reflect prescription preferences in special patient groups. In patients with IBD, oral agents could cause gastrointestinal discomfort and gastrointestinal absorption could be decreased. As a result, they may prefer intravenous agents and more BPs prescription could be preferred. Because BPs would be avoided in renal disease, such patients may have more SERMs prescriptions. A higher incidence of dyslipidemia could be explained by the benefit of improving lipid profile via SERMs. SERMs, which are taken daily, may have been preferred in patients with dementia, because BPs have weekly or monthly dosage forms. The results show that DM, rheumatologic diseases, and past hospitalization history were more common in the SERMs group than BP group, which is in contrast to the previous findings that SERM users had less comorbidities.2728 However, another study in Korean women with osteoporosis reported that the raloxifene group had a higher prevalence of rheumatologic and autoimmune diseases.29 The reason was explained by the higher proportion of tertiary health care institutions among these patients, because raloxifene was more commonly prescribed by clinicians in the tertiary referral hospitals.29 Our result could be explained by same reason, but considering the relationship of rheumatoid disease and increased coagulability, further analysis is needed. There may have been a tendency to be more obese because there were more drinkers in BP group than SERMs group. The higher incidence of major osteoporotic fracture in the BP group could be explained by the tendency to prescribe BP rather than SERMs first in people with a higher risk of fracture.
There are some limitations in this study. First, because of using claims data for patient information, the available data were limited. The data of diagnosis, procedure, and pharmacologic prescription were collected by review of ICD-10 code and drug principal component codes. Moreover, the claims data were not always in accordance with actual clinical practice. Second, potential confounding factors might not be ruled out because demographic data were insufficient, and comorbidities were identified by ICD-10 codes in the claim data.
Nevertheless, this study has strengths. Osteoporosis itself might be associated with an increased risk of VTE due to fracture, pain, and immobilization.9 Further, the patients with osteoporosis are often older and have several comorbidities that could affect VTE development. Therefore, it is meaningful to confirm if the risk of VTE increases after taking osteoporosis medications. Finally, this is the first large-scale study on the effect of SERMs on VTE development in Korean population.
In conclusion, SERMs did not increase the risk of VTE compared to BPs in Koreans with osteoporosis, after adjustment for confounders. However, past hospitalization history, estrogen, and glucocorticoid replacement therapy increased the risk of VTE in the SERMs user group. Therefore, SERMs are not recommended in patients with high risk for VTE.
Go to :
 XML Download
XML Download