

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Depression has become a serious concern worldwide.1 Additionally, in Korea, the lifetime prevalence of major depressive disorders reached 6.7% in 2011. It was especially higher in women, at 9.2%. Although this number is lower than those of the Western countries such as the United States of America, Italy, and France, it is higher than those of Nigeria and China, and is increasing every year.2 Therefore, early detection and intervention of depression in Korea is exceedingly important for preventing suicide,34 labor loss,56 and social costs78 caused by it. As the only divided country in the world, Korea maintains the conscription system; as of the 2012 Defense White Paper, there are 639,000 soldiers in South Korea.9 The hierarchical nature of the military organization and maladjustment due to forced enlistment in the military are likely to make Korean soldiers more vulnerable to depression.10 In fact, the one-year prevalence of major depressive disorder among Korean men aged 18–29 years was 1.4% in the 2006 National Survey on Mental Disorders,11 whereas, that of the Korean soldiers was higher at 2.3% in 2007.12 In Korea, the military service physical examination prior to enlistment limits the recruitment of mentally ill patients, however, the period of military service in Korea (18–29 years) corresponds to the age group with a frequent onset of depression.1314 Furthermore, it implicates soldiers with a predisposition to depression to develop clinical depression symptoms due to stress from the military environment. Therefore, the evaluation of depression for Korean soldiers needs to be carried out on a large-scale, and occasionally, even on the whole.
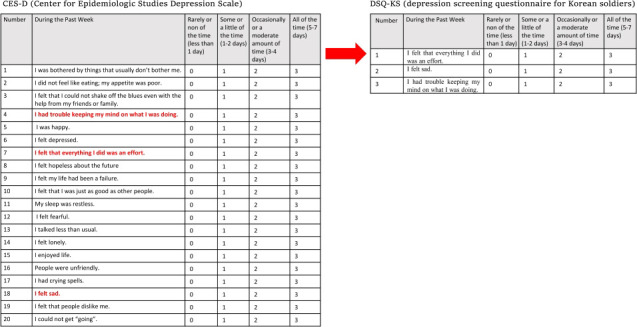
The Center for Epidemiological Studies for Depression Scale (CES-D) was developed as a representative depression measure for large-scaled epidemiological studies; its high reliability and validity were reported in various groups.15 However, it was cumbersome to implement CES-D with a total of 20 questions on every occasion; thus, its short versions were developed in previous studies.161718 However, in Korea, no such short form scale has been developed for the special circumstances of conscripted soldiers. In this study, deriving from the existing CED-D scale items, we aimed to develop and validate a simple yet highly predictive scale that can easily be applied to Korean soldiers.
Go to : 
METHODS
Participants
This study was carried out as part of a larger study titled ‘Epidemiological Study on the Prevalence of Depression in Military Service and a Search for High Risk Group Management’ conducted by the Chuncheon Mental Health and Welfare Center of Korea. Between September 1, 2012 to May 11, 2013, trained interviewers visited military units that had been approved for research beforehand. Before the interview began, the self-report questionnaires and informed consents were obtained and confirmed. The participants were explained that this interview could not identify the individual participants and that the outcome of this interview would not result in any disadvantage. Then, interviewers conducted face-to-face interviews and assessments with soldiers. A 1,310 soldiers from the army, air force and navy responded to the research interview.
Measurement
Demographic variables
In this study, socio-demographic data such as age, religion, marital status, and past psychiatric diagnoses as well as military service environment data such as ranks and troops were collected. Ages were categorized as under 19, 20, 21, and over 22 years old. Soldiers of the air force, army, and navy that constitute the Korean military system were included.
Clinical variables
In this study, the Korean version of the Mini International Neuropsychiatric Interview (K-MINI) was used as a diagnostic tool to identify clinical depression (major depressive episode, MDE).1920 It can be implemented in about 15 minutes with simple training. In the case of major depressive disorder, the Kappa value, the sensitivity, and the specificity were 0.71, 0.83, and 0.91, in the order given.19 The CES-D questions were employed as preliminary items for the depression scale we were developing. The 20-item CES-D, developed by the National Institute of Mental Health, is rated on a 4-point (0–3) Likert scale and is used for large-scale epidemiological studies. A validation study conducted in Korea defined the cut-off value to be 21 points for effectively detecting depressive symptoms during screening.21 In this study, the CES-D was implemented on all soldiers to derive its individual items that had the most significant correlation with clinical depression in the group. The suicide risk assessment item of the Korean version of the Composite International Diagnostic Interview was utilized to evaluate the participants' suicide risk.2223 Information regarding whether or not they had been experiencing suicidal ideations, plans, and attempts throughout their lifetimes or merely for the current month was examined using structured interviews. If they experienced any of the three symptoms, they were defined as having suicidality. The Stress Response Inventory (SRI) was used to assess the participants' stress. It is a self-reported five-point (0–4) Likert scale that examines the emotional, somatic, cognitive, and behavioral responses to stress.24 In this study, a 26-item modified short form was employed.25 In addition, the Barratt Impulsiveness Scale (BIS), which is rated on a four-point Likert scale (1–4), was utilized to evaluate the participants' impulsiveness.26 It was translated in Korean in 1992 and assesses impulse in three subcategories with nine, eight, and six items for non-planning, motor, and cognitive impulsivities, respectively.27 Finally, the Lubben Social Network Scale-6 (LSNS-6) was used to examine the participants' social support. It consists of six items that are rated on a six-point (0–5) Likert scale; the total score is 30 points. Furthermore, three items are about relations with relatives and friends. The higher the score, the higher the social support.28
Statistical analysis
Firstly, descriptive statistics were calculated for age, the type of troop, class, marital status, religion, past psychiatric diagnosis, and CES-D, BIS, SRI, and SNS scores of the participants. Subsequently, Pearson's correlation analysis between each of the CES-D's 20 items and MDE was performed using K-MINI's diagnosis as a yardstick. In this analysis, three to five items with the highest correlation coefficient were derived, and a scale comprising three items was determined through panel discussion. We named it as the ‘Depression screening questionnaire for Korean soldiers’ (DSQ-KS). Subsequently, Cronbach's alpha analysis was performed on the DSQ-KS to assess its internal consistency. A principal component analysis was conducted to confirm its factor structure. Furthermore, the area under the curve (AUC) value, obtained by performing the receiver operating curve (ROC) analysis, was conducted. To confirm the discrimination validity, the DSQ-KS's total score (of three items) was considered as an independent variable and the diagnosis of major depressive disorder as a dependent one. Simultaneously, the cut-off value, sensitivity, and specificity were calculated. To check the concurrent validity, a χ2 test between depression and suicidality based on the cut-off score of the DSQ-KS, and an independent t-test to examine the average difference between the BIS, SRI, and LSNS-6 scores according to depression levels were conducted. Finally, the characteristics of the group that was screened as positive for depression on the CES-D scale; however, negative on the DSQ-KS scale were compared.
Ethics statement
The study was conducted with the approval of the Bioethics Committee of the Armed Forces Medical Research Institute (approval No. AFMC-12-IRB-071). In this study, informed consents were obtained from the individual participants. Participants also had the right to veto the study participation.
Go to :
RESULTS
Of the soldiers interviewed, 1,006 with CES-D results were included in the final analysis. The participants' characteristics are presented in Table 1. In all, 70% of the participants were 20 and 21 years old. The ratio of the army, air force, and navy was relatively even. Among the participants, the proportion of the first private and corporal soldiers was the highest, and all, except one, were unmarried. Overall, 9.4% reported lifetime suicidality, and 4.6% had ongoing MDEs. In addition, the averages of the main variables CES-D, BIS, SRI, and LSNS-6 are shown in Table 1.
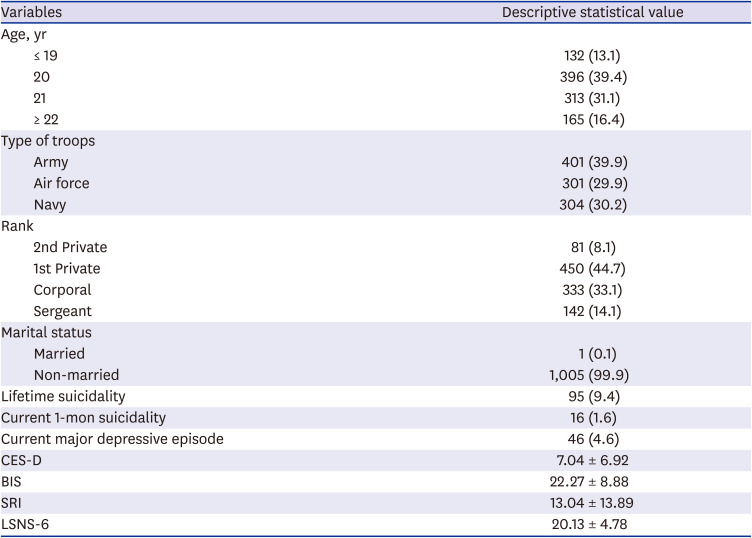
Table 1
Characteristics of participants (n = 1,006)
Categorical variables were presented as number (%), while continuous variables were presented as mean ± standard deviation.
CES-D = the Center for Epidemiological Studies for Depression Scale, BIS = Barratt Impulsiveness Scale, SRI = Stress Response Inventory, LSNS-6 = Lubben Social Network Scale-6.
![]()
In the correlation analysis between the MINI's MDE diagnosis and each of the 20 CES-D items, 7, 18, 4, 20, and 6 were derived based on the order of correlation coefficient (Table 2). In all, three items, namely 7, 18, and 4, were selected mutually through a panel discussion involving two psychiatrists and an epidemiologist, reflecting the development aim of constructing as simple a scale as possible.

Table 2
Correlations between diagnosed major depressive episode and items of CES-D (only 5 items with higher correlation coefficient were listed)
Items were presented in the order of the highest coefficient.
CES-D = the Center for Epidemiological Studies for Depression Scale.
Three items with high correlation coefficients were displayed in bold.
![]()
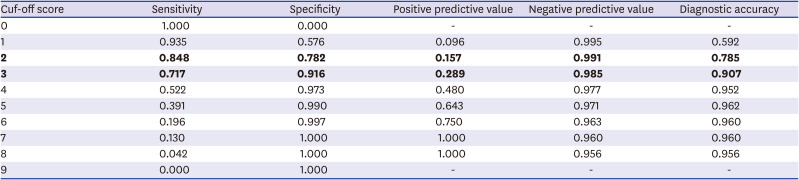
As a result of the factor analysis on the scale consisting of three items, a factor was derived (variance: 64.2%). Among the three items, the communality was 0.5 or more and the factor loading was 0.7 or above (Table 3). The Cronbach's alpha value of the DSQ-KS scale was 0.720. In the ROC analysis using K-MINI's MDE diagnosis as the gold standard, the AUC value was 0.891 (Fig. 1). When the cut-off score was defined as 2 points, the sensitivity and specificity were 84.8% and 78.2%, respectively. At this time, the positive predictive value was 15.7%, while the negative one was 99.1%. On the other hand, when the cut-off score was defined as 3 points, the sensitivity and specificity were 71.7% and 90.4%, respectively. The positive and negative predictive values were 28.9% and 98.3%, respectively (Table 4).

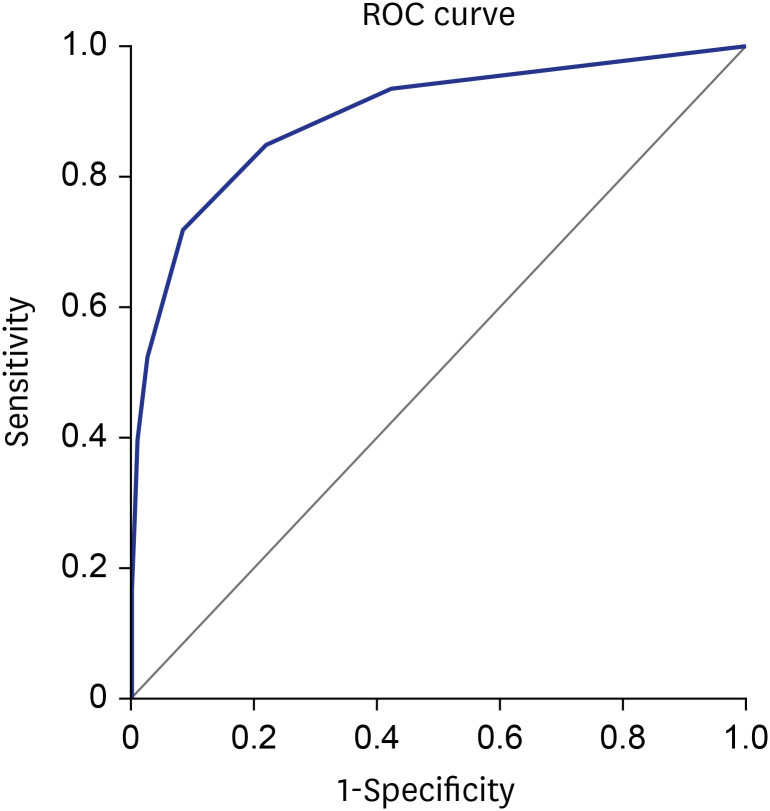 | Fig. 1ROC analysis of depression screening questionnaire for Korean soldiers with clinical depression as gold standard. The area under the curve is 0.891.ROC = receiver operating curve.
|
Table 3
Factor analysis of depression screening questionnaire for Korean soldiers (one factor was derived from principal component analysis)
| Items | Communality | Factor loading | Variance, % |
|---|---|---|---|
| I felt that everything I did was an effort. | 0.699 | 0.836 | 64.210 |
| I felt sad. | 0.598 | 0.773 | |
| I had trouble keeping my mind on what I was doing. | 0.630 | 0.794 |
![]()
Table 4
Cut-off score and corresponding sensitivity, specificity, positive predictive value, negative predictive value and diagnostic accuracy of depression screening questionnaire for Korean soldiers
![]()
In the test for concurrent validity, the group at risk of depression with a DSQ-KS cut-off score of ≥ 2 had a significantly greater lifetime suicidality (16.9% vs. 7.7%) (P < 0.001) and current 1-month suicidality (1.2% vs. 0.1%) (P = 0.049). Furthermore, as compared to the other group, this group showed higher scores in the BIS (26.61 ± 8.80 vs. 21.69 ± 8.21) (P < 0.001) and SRI (26.35 ± 16.70 vs. 9.65 ± 9.70) (P < 0.001), however, lower ones in the LSNS-6 (18.41 ± 4.76 vs. 20.43 ± 4.62) (P < 0.001). This result was consistent even when the cut-off was applied as 3 points (Table 5).

Table 5
Concurrent validity between DSQ-KS and other mental health index
Categorical variables were presented as number (%), while continuous variables were presented as mean ± standard deviation.
DSQ-KS = depression screening questionnaire for Korean soldiers, BIS = Barratt Impulsiveness Scale, SRI = Stress Response Inventory, LSNS-6 = Lubben Social Network Scale-6.
![]()
When the cut-off of DSQ-KS was presented as 2 points, none of the participants who were under the cut-off score (2) was screened as ‘Positive for depression screened by CES-D,’ which was based on the CES-D score with 21 as the cut-off score. On the other hand, when the cut-off was set at 3 points, there were seven participants who were found to be positive for the CES-D and negative for the DSQ-KS. Moreover, one participant was actually diagnosed with an MDE in the K-MINI (Table 6).

Table 6
Characteristics of the 7 participants who were screened as ‘depression’ in the Center for Epidemiological Studies for Depression Scale, but not in DSQ-KS when ‘3’ was chosen as cut-off score
There was no one who was screened as ‘depression’ but not in DSQ-KS when ‘2’ was chosen as the cut-off score.
DSQ-KS = depression screening questionnaire for Korean soldiers, MDE = major depressive episode, BIS = Barratt Impulsiveness Scale, SRI = Stress Response Inventory, LSNS-6 = Lubben Social Network Scale-6.The information of the participant who was negative in DSQ-KS but positive in CES-D was displayed in bold.
![]()
Go to :
DISCUSSION
This study attempted to develop the DSQ-KS, a simple and valid scale for Korean soldiers based on the CES-D items that has been widely used in the existing epidemiological studies. The results of this study indicated that the three items of the DSQ-KS were appropriately loaded with a single factor, indicating unidimensionality. The Cronbach's alpha value is generally considered to be ‘acceptable’ if it is between 0.70 and 0.95,29 and that of the DSQ-KS was 0.720. When considered together with the result of factor analysis, the DSQ-KS demonstrated reliable internal consistency, and three items can be considered as evaluating depression as a homogeneous concept. The AUC value was 0.891, suggesting that it is a ‘good to excellent test’ for diagnosing clinical depression in the Korean soldier group.30
Regarding the cut-off score of the DSQ-KS, scores of 2 and 3 points were suggested. There was a trade-off between sensitivity and specificity in each cut-off score. Therefore, the score of the DSQ-KS can be applied differently depending on the characteristics of the target group, the prevalence of depression, and the purpose of the screening survey. Since the positive and negative predictive values of the scale vary according to the prevalence rate of the target group,31 using a 2-point cut-off score for a military soldier group whose depression prevalence rate is higher than that of the general population group9 may be appropriate for heightening negative predictive value. However, this study's findings indicated that the negative predictive value at 2 and 3 cut-off points was 99.1% and 98.5%, respectively, with no significant difference. Therefore, the situation of the target group at the time of applying the DSQ-KS is the most important consideration in selecting the cut-off score. For example, when there is psychological trauma due to a safety accident in the unit, it is recommended to implement the cut-off score as 2 points, while 3 points is recommended for the routine follow-up survey. In this study, two cut-off scores (2 and 3) were all significantly associated with suicide,34 impulsivity,32 and social support.33 These phenomena have been reported to have a profound relationship with depression. The concurrent validity of the DSQ-KS could be verified as the presence of depression screened by the DSQ-KS was significantly related to those phenomena.
When the cut-off was defined as 3 points, the sensitivity decreased to 71.7%. However, when the seven participants who were positive for the CES-D and negative for the DSQ-KS were analyzed, there was only a single clinical depression case, and even that participant showed lower levels of impulsivity and stress than the average of the group. In addition, the participant had lifetime but not current suicidality. Furthermore, the CES-D score was 21 points corresponding to the cut-off score. Therefore, even when the cut-off is defined as 3 points, the DSQ-KS can be evaluated as showing consistent predictive power and accuracy as the CES-D.
The clinical significance of this study is that we developed and validated a highly accurate scale having using only three items to predict clinical depression in Korean soldiers. It can be useful in future military-related mental health promotion projects, and it is expected to contribute to including patients with depression that have not been identified into treatment settings. In addition, recently, the Korean military approved the use of smart phones to soldiers in the unit, so the developed scale can be used as an app, which can be helpful for the soldiers to self-diagnose their depression status. Through these attempts, the developed scale can ultimately serve as a cornerstone for improving the overall diagnosis and treatment of depression among soldiers.
On the other hand, the limitation of the DSQ-KS is that the 3 items of the scale do not include all domains of symptoms constituting depression. According to the DSM-5, an official diagnostic criterion for mental disorders, five or more of a total of nine symptoms and a period of two weeks of experiencing those symptoms or more must be met for the diagnosis of MDE.34 Therefore, a high score on the DSQ-KS cannot necessarily have the same inference as clinical depression. However, its three items, namely, ‘I had trouble keeping my mind on what I was doing’ (CES-D No. 4), ‘I felt that everything I did was an effort’ (CES-D No. 7), and ‘I felt sad’ (CES-D No. 18), are items representing symptoms of depression related to cognition, somatic, and emotions, respectively. In addition, according to the results of the statistical analysis, these items predicted clinical depression with substantial accuracy; thus, it has been considered that they can be sufficiently useful as a screening tool. However, after being screened by the DSQ-KS, the final diagnosis of depression must go through a clinical evaluation process.
In addition, since the DSQ-KS was validated in a special group (Korean soldiers), it is difficult to apply it to other heterogeneous groups. This is because it did not consider the generalizability, mostly for easy application and interpretation in the Korean soldiers' group, which was of utmost importance in the development goal. However, the number of soldiers in the Korean military itself constituted a large group, with hundreds of thousands of people, and the importance of screening depression in this group was especially important due to the characteristics of the age and closed military environment that render soldiers vulnerable to depression. Therefore, the DSQ-KS can be considered as a screening tool that meets these needs.
In conclusion, in this study, we developed a three-item short form scale to screen depression in Korean military soldiers, and also confirmed its reliability and validity. The scale developed through this study can play a great role in clinical practice and research related to military mental disorders in the future.
Go to :
 XML Download
XML Download