

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The age of onset of type 2 diabetes has decreased in the last decades and is driven by the global burden of obesity.12 Therefore, the incidence of type 2 diabetes is increasing among children, adolescents, and younger adults. Accumulating evidence has suggested that this early-onset diabetes, which refers to diabetes that develops in adults of < 40 years old, shows more aggressive phenotype resulting in the early development of complications34 when compared with late-onset diabetes. However, few studies have focused on the status, management, and prevention of complications of early-onset diabetes in younger adults aged 20–39 years.
Considering the longer life-span of young adults with early-onset diabetes, focusing on this particular population aged 20–39 years is critical for the reduction of medical and social burdens in the future. However, there are limited data on the characteristics and management of young Korean adults with diabetes.567 Therefore, further elucidation of the clinical characteristics of early-onset diabetes will provide basic and key information for proper diabetes management and policymaking for the younger adult population.
Thus, this study aimed to assess the clinical characteristics, socioeconomic status, management of diabetes, health behaviors, and mental health or psychological distress among young Korean adults with diabetes mellitus.
Go to : 
METHODS
Participants
This study was designed to clarify the clinical characteristics of early-onset diabetes and barriers to glycemic control in young Korean diabetic patients by the young adult diabetes study group. The young adult diabetes study group conducted this study in two different designs from October 2017 to October 2018 among five university hospitals in the Republic of Korea. One study design was a cross-sectional study that used questionnaires for assessing the socioeconomic status, general health, diabetes care, health behaviors, and mental health among four university hospitals. The other study design was a retrospective chart review of young adults with diabetes to assess their medication, laboratory data, and complications and concurrent comorbidities.
This study will focus on the general health care and socioeconomic factors among young adults with diabetes using the questionnaire. Study participants comprised young adults with an early-onset diabetes aged 20–39 years. Participants were selected (n = 225) who completed the questionnaire from four university hospitals (Konkuk University hospital, n = 12; Kangwon National University Hospital, n = 35; Ulsan University Hospital, n = 120; Soonchunhyang University Gumi Hospital, n = 58).
Assessment of clinical characteristics, socioeconomic status, management of diabetes, and health behaviors
Each questionnaire was developed for assessing the clinical characteristics (age, sex, type of diabetes, family history of diabetes, and the reason for diabetes diagnosis), socioeconomic status (education levels, employment status, occupational status, and income), management of diabetes (treatment of diabetes, admission history, diabetes complication, history of fundus examination, awareness of the value of hemoglobin A1c [HbA1c], and concurrent diseases), and health-related behaviors (drinking, smoking, physical activity, daily screen time, and eating habit) in this study.
Physical activity was assessed using the International Physical Activity Questionnaires (IPAQ) and categorical score was used. An overall total physical activity was calculated using the metabolic equivalent of task (MET) score, i.e., MET-minutes/week score, which can be computed as the total physical activity MET-minutes/week = sum of total (walking + moderate + vigorous) MET- minutes/week scores. Results can be reported in categories as category 1: inactive (< 600 MET × minutes per week), category 2: minimally active (600–3000 MET × minutes per week), and category 3: health-enhancing physical activity (HEPA) active (> 3,000 MET × minutes per week) physical activities. In the self-reported questionnaire, participants were asked to report on how many hours per day on average they played computer games, watched TV/DVD/internet material, and used the internet.
Assessment of mental health or psychological distress
The number of hours of sleep was assessed using the following question inserted into the self-reported questionnaire: “On average, how many hours do you sleep per night?” Sleep duration was further classified into three groups: short (< 6 hours), normal (6–8 hours), and long (≥ 9 hours).
Stress perception, depressed mood, and suicidal ideation were assessed for evaluating participants’ mental health. Stress perception was assessed using the following question: “How stressed are you on a daily basis?” “Extremely stressed” or “quite stressed” responses were classified as stress perception, and “a little bit stressed” and “hardly stressed” were classified as no stress perception. To assess depressed mood, participants were asked this question. “During the past year, have you felt feelings of sadness or hopelessness that persisted for at least two weeks and that disrupted your social life?” This question is included in the World Health Organization Composite International Diagnostic Interview (CIDI)-Short Form and subjects answered “yes” or “no” in response to whether they had experienced depression for two or more continuous weeks during the previous year.
Suicidal ideation was assessed by participants' positive answer to the following question: “During the past year, have you ever felt that you were willing to die?” A “yes” or “no” response was also used to determine whether the participants had suicidal thoughts. Screening, severity and diagnosis of depression were performed using the Korean version of Beck Depression Inventory (K-BDI) score.
Ethics statement
The study protocol was approved by the institutional review board of Kangwon National University Hospital (2017-09-008) and individually by the institutional review boards of each collaborating hospital. Written informed consent was obtained by all subjects when they were enrolled.
Go to :
RESULTS
Demographic and clinical characteristics of early-onset diabetes
Overall, 225 participants with early-onset diabetes were recruited from four university hospitals in South Korea. The characteristics of the participants are summarized in Table 1. The mean age of study patients was 33.1 ± 6.0 years, and the mean age at diagnosis was 29.2 ± 6.8 years.
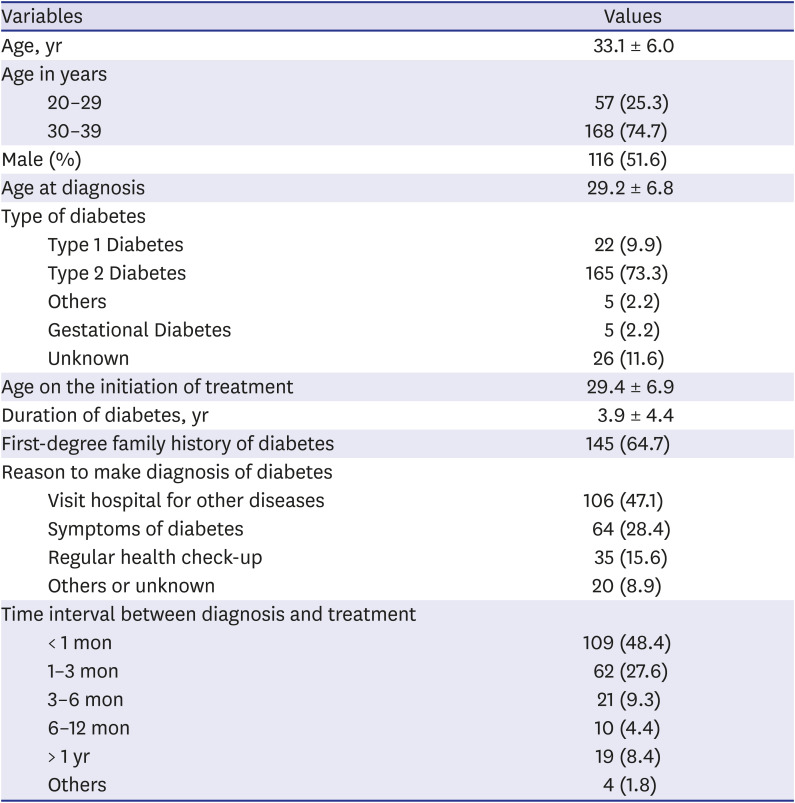
Table 1
Clinical characteristics of study participants (n = 225)
![]()
The number of patients with type 1 diabetes, type 2 diabetes, gestational diabetes, other types, and unclassified diabetes were 22 (9.9%), 165 (73.3%), 5 (2.2%), 5 (2.2%), and 26 (11.6%), respectively. Among them, 116 patients (51.6%) were men, and 145 patients (64.7%) had at least one first-degree relative with diabetes. The reason to undergo diagnosis for diabetes includes a hospital visit for another reason (n = 106, 47.1%), symptoms of diabetes (n = 64, 28.4%), regular health check-up (n = 35, 15.6%), and others, including unknown reasons (n = 20, 8.9%). The time interval between diagnosis and treatment was within three months in most cases (n = 171, 76%).
Most patients (n = 179, 79.6%) have a higher education level, such as college, university, and graduate school degrees (Table 2). The number of unemployed participants was 63 (28.0%), and most participants had a regular job (n = 102, 82.9% when compared with temporary jobs). The number of participants with an average monthly income < 1,500,000 won (low income) was 31 (15.5%).
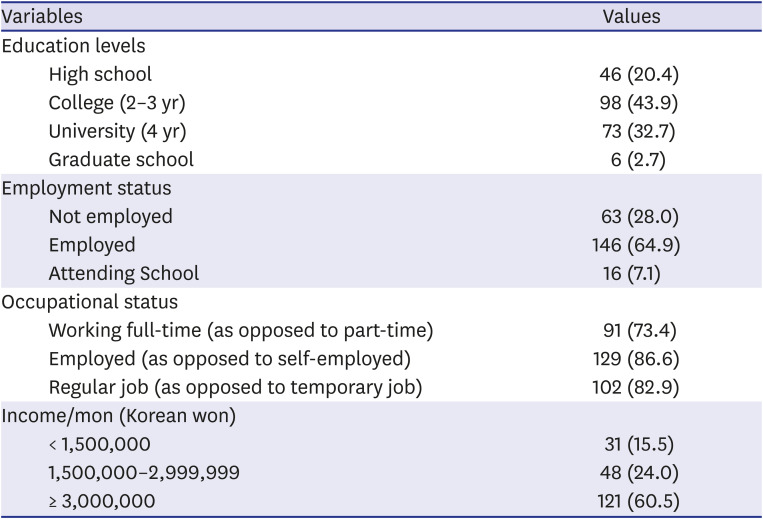
Table 2
Socioeconomic status of study participants (n = 225)
![]()
Management of early-onset diabetes
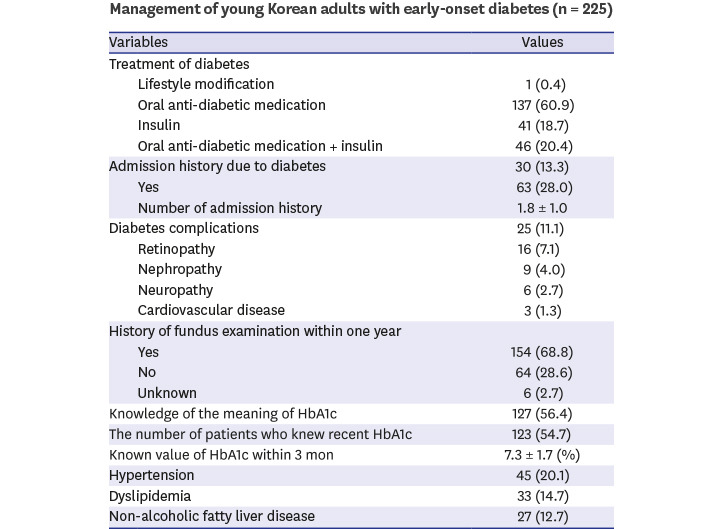
The management of diabetic participants is presented in Table 3. Most patients with early-onset diabetes (n = 137, 60.9%) received only oral anti-diabetic medication, and 18.7% of participants received only insulin therapy. The self-reported diabetes complication rate was 11.1%, and retinopathy was most common complication. Among the participants, 13.3% of patients had an admission history of diabetes management. More than two third of the patients (n = 154, 68.8%) had fundus examination within one year. More than half of the patients (n = 127, 56.4%) had the knowledge of HbA1c. The number of patients who knew their recent HbA1c value was 123 (54.7%); their mean HbA1c within three months was 7.3 ± 1.7 (%). Approximately 20.1% of patients had concurrent hypertension.
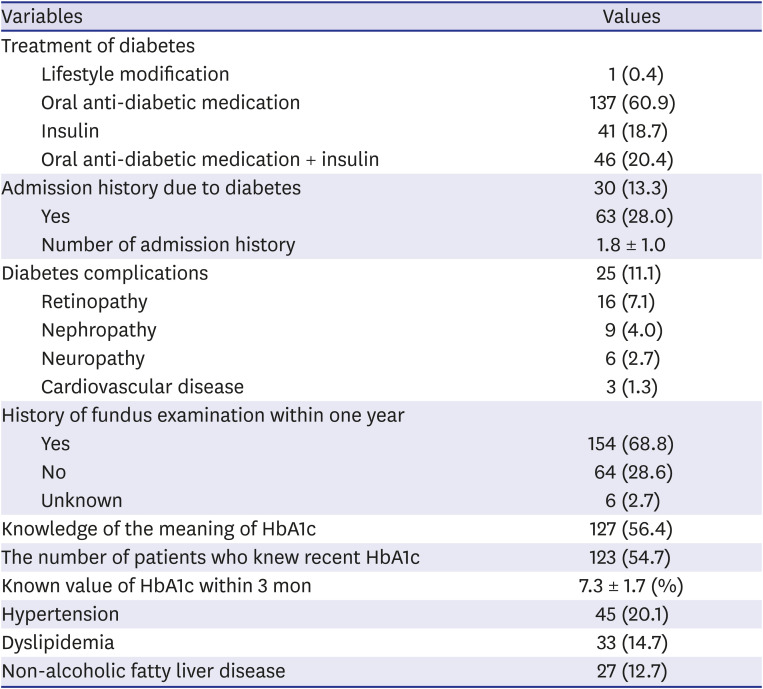
Table 3
Management of diabetes (n = 225)
![]()
Health-related behaviors of early-onset diabetes
More than half of the participants (55.4%) were non-smoker, and current smoker accounted for 30.4% and ex-smoker 12.4%. Considering the categorical IPAQ score, we found that 48 patients (24.5%) were physically inactive (category 1), 93 (47.4%) were minimally active (category 2), and 55 (28.1%) were in the HEPA category of physical activity. Men were more physically active than women (men 3,476.3 ± 4,274.0 METS vs. women 2,166.2 ± 3,992.5 METS, P = 0.028). Additionally, 26.5% of the participants had their daily screen time of ≥ 3 hours a day. For the breakfast eating frequency in a week, 32.7% (n = 73) never consumed breakfast, 24.7% rarely consumed breakfast (1–2 days/week), 16.1% consumed breakfast on some days (3–4 days/week), and 26.5% consumed breakfast on most days (5–7 days/week). Additionally, 60.5% of the patients were eating meals outside of the home for at least three days a week (Table 4). Younger men go out for eating more frequently (more than three times a week) than younger women (48.7% vs. 29.6%, P = 0.004).
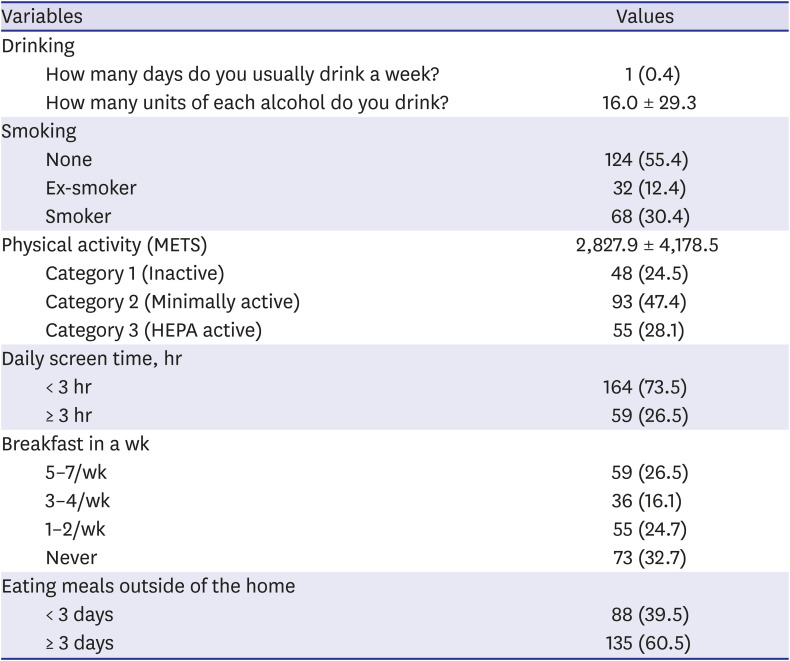
Table 4
Health-related behaviors of study participants (n = 225)
Values are expressed as mean ± standard deviation or number (%).
HEPA = Health-Enhancing Physical Activity.
![]()
Mental health of early-onset diabetes
Majority of the patients (75.7%) slept for 6–8 hours a day, and 17.1% slept for < 6 hours a day. Half of the patients (n = 109, 48.9%) showed moderate to severe stress perception, and 9.0% answered experiencing depression for two or more continuous weeks.
Among the 225 participants, 12 (5.3%) had suicidal ideation, and 7 (3.1%) had suicidal planning during the previous year. Based on the K-BDI score, 44 (21.4%) patients suffered from moderate to severe levels of depression (Table 5). Women frequently suffered from moderate to severe levels of depression than men (28.3% vs. 15.0%, P = 0.020).
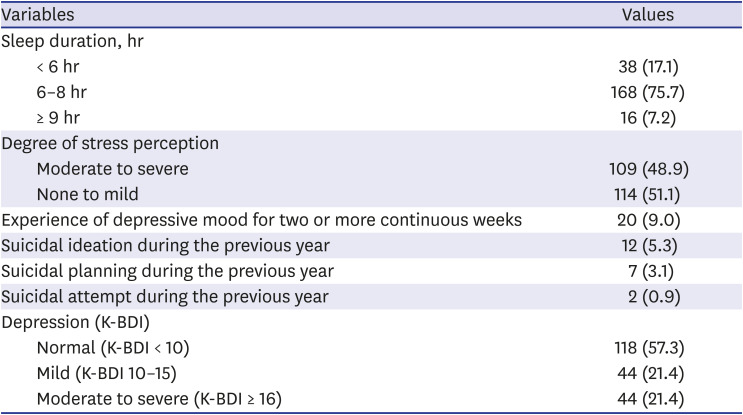
Table 5
Mental health of study participants (n = 225)
![]()
Go to :
DISCUSSION
Our study demonstrated that 13.8% of early-onset diabetic patients were classified as other types or unknown diabetes with mostly type 2 diabetes (73.3%); participants had a strong family history of diabetes (64.7%), and the majority (76%) of the younger adults started their treatment within three months of diagnosis in Korean outpatient clinics in four University hospitals. Approximately, 11.1% of the participants had diabetic complications, and approximately half of the participants (56.4%) had knowledge of HbA1c. Additionally, 39.1% of the participants received insulin injections including oral anti-diabetic medications, and 18.7% received only insulin treatment; 30.4% were smokers, and only 28.1% were in category 3 (HEPA active) physical activity. Moreover, 26.5% of the participants had a screen time of >3 hours. About one third of the participants never had breakfast (n = 73, 32.7%), and more than half of the participants (n = 135, 60.5%) went out to eat for at least three times a week, suggesting the lifestyle characteristics of modern young adults in Korea. Our study provides a comprehensive description of demographic and clinical characteristics, management of diabetes, health behaviors, and mental health characteristics of younger adults with diabetes in Korea.
The management status of diabetes in younger adults might vary from the primary care clinics to university hospitals in Korea. In our study, most participants started their treatment within three months from the diagnosis, and approximately half of the study patients had sufficient knowledge of HbA1c and their recent HbA1c levels, and 68.8% of the patients had fundus examination within one year in outpatient clinics at four university hospitals. Recent study showed that the overall status of type 2 diabetes management, including HbA1c levels, blood pressure, and serum lipid levels, was suboptimal in primary care clinics in Korea.8 According to this report, the screening rates for diabetic nephropathy and retinopathy within the past one year in 2,915 patients with type 2 diabetes were 28.4%, and 23.3%, respectively, at primary care clinics when compared with 87.8%, and 49.7%, respectively, at tertiary hospitals in Korea.8
In young healthy Japanese men, repeated breakfast skipping was shown to induce abnormal glucose fluctuations.9 In a nationally representative prospective cohort among US adults, skipping breakfast was associated with a significantly increased risk of cardiovascular mortality.10 Another study demonstrated that skipping breakfast increased postprandial hyperglycemia and impaired insulin response after lunch and dinner in individuals with type 2 diabetes.11 Altogether, growing evidence suggest the importance of eating breakfast as a simple way to promote better glucose control and cardiovascular health. In Korea, the frequency of having breakfast in individuals aged < 42 years is 41.7% when compared with 72.6% in individuals aged ≥ 42 years,12 suggesting the need for healthy nutritional approach in younger adults. Younger adults with diabetes are known to have higher stress, higher levels of diabetes-related distress, depressive symptoms, and poor self-management, such as less physical activity.13 Another study on type 2 diabetic adolescents with a mean age of 15.4 years in the US showed that poor dietary intake, less exercise habits, and nonwhite race were significantly associated with poorer glycemic control even after adjusting for covariates.14 Education of healthy lifestyle modification should be the cornerstone of treatment of diabetes in younger adults.
There are many difficulties and challenges in the management of diabetes in young adults. First, it is challenging to differentiate type 2 diabetes from type 1 diabetes and other types, such as monogenic diabetes in young adults.215 There is no clear-cut definition to differentiate type 1 diabetes and type 2 diabetes, and the classification of diabetes could be changed after months or years to ascertain diabetes classification and would be labelled as ‘diabetes—undetermined’. According to a study in Sweden,16 75% of all newly diagnosed diabetic patients aged 15–34 years were classified as type 1 diabetes, 19% as type 2 diabetes, and 6% as secondary diabetes or were classified as uncertain by their physician; however, at follow-ups, 71% were classified as type 1, 21% as type 2, and 8% as secondary or uncertain,16 suggesting the difficulties in classifying diabetes in young adults. Hence, it is essential to re-classify the type of diabetes with follow-up C-peptide and glutamic acid decarboxylase antibody measurements when the clinical course or characteristics is not typical in the young adult population.17
Second, the pathophysiology of early-onset diabetes is heterogeneous and not well-clarified and may be different from late-onset diabetes. According to a Chinese study, there was a low prevalence of metabolic disorders, insulin resistance, and severe insulin secretion dysfunction in 342 admitted patients with early-onset diabetes diagnosed at 15–45 years old than in 296 admitted patients with late-onset diabetes diagnosed at > 45 years old, suggesting a low β-cell function as a key factor in the development of early-onset diabetes.18 Another study suggested that early-onset type 2 diabetes was associated with a strong genetic predisposition of β-cell dysfunction in the Chinese Han population19 and gene variants related to decreased acute insulin secretion in Pima Indians.20 Obese white participants with early-onset type 2 diabetes demonstrated marked insulin-resistance with a marked loss of β-cell function than control participants matched for age and obesity, and surprisingly, there were no metabolic improvements in either study group to a 3-month aerobic exercise intervention.21 Further study is necessary to elucidate the genetic or physiological mechanism related to the early development of diabetes and to make effective interventions for improving β-cell function and glycemic control in young adults.
Third, the earlier onset of diabetes indicated longer exposure to hyperglycemia, resulting in greater lifetime risk of diabetic complications, and the phenotype of early-onset diabetes is known to be more aggressive than late-onset diabetes, leading to premature development of complications.3 These challenges make it harder to control and manage diabetes in young adults. Thus, it is crucial to fully understand the natural history of diabetes, development of complications or mortality in young adults.22 Recently, accumulating data have suggested that type 2 diabetes in young adults have a higher risk of complications and mortality.22232425 A previous study reported that patients with type 2 diabetes and with the age of onset between 15–30 years had more frequent diabetes complications and less favorable cardiovascular disease risk factors than patients with type 1 diabetes and with a similar age of onset.26 In the same study group, early-onset type 2 diabetes diagnosed between 15–30 years of age showed more severe albuminuria and neuropathy than late-onset type 2 diabetes diagnosed between 40–50 years of age.27 Another study demonstrated that early-onset diabetes diagnosed below 40 years of age had a high lifetime risk for retinopathy irrespective of diabetes type.28
Some studies have reported that low socioeconomic status (SES) was related to a higher risk of type 2 diabetes and diabetic complications.293031 A study with 672 young adults with type 2 diabetes aged 20–40 years in Japan reported low SESs such as junior high school graduates, patients receiving public assistance, those with low income, or no employment were associated with a greater likelihood of developing type 2 diabetes complications.30 In a German study, SES was an independent factor for low renal function in type 2 diabetic patients.31
The prevalence rate of depression is known to be much higher in people with type 2 diabetes (17.6% vs. 9.8%) than in people without diabetes.32 The comorbidity of diabetes mellitus and depression has a negative impact on both diabetes self-care and cognitive function, possibly increasing the worse overall clinical outcome, medical cost, and mortality.3334 In our study, half of the patients showed moderate to severe stress perception, and 21.4% of patients suffered from moderate to severe levels of depression, suggesting that mental distress or depression might be frequently comorbid in young adults with diabetes. Undetected or untreated depression may prohibit an individual's ability to successfully manage glycemic control and hinder their adherence to treatment or self-care activities. In contrast, diabetes mellitus itself may increase the risk of depression or depressive symptoms.34 Therefore, it is a critical component of effective health management to prevent, recognize, and treat depression properly in the context of caring for young adults with diabetes.
Our study has several limitations. First, it was a cross-sectional questionnaire-based study with a relatively small study population. Second, there was a lack of objective anthropometric measurement or biochemical data of younger adults with diabetes. Third, our study population involved outpatients of university hospitals; hence, it may not be representative of other diabetic patients treated in primary clinics. Additionally, participants tended to be of a high SES to visit university hospitals, where the medical cost is much more expensive when compared with primary clinics.
Understanding the demographic, socioeconomic, and clinical characteristics of young adults with diabetes and clarification of the natural course or disease entity of young adults with diabetes should be preceded to suggest the effective strategies for the prevention of early-onset diabetes and their related complications. Elucidation of individual risk factors such as genetic and environmental factors and the optimal treatment guidelines, including lifestyle modification and mental health management, necessitate clinical intervention studies to explore more effective and evidence-based protocols for improving preventive and therapeutic measures in young adults.
In conclusion, early-onset diabetes was associated with a strong family history, early insulin treatment, poor health behaviors and frequent mental depression. These findings suggest the necessity of health policies for improving health behaviors and mental distress.
Go to :
 XML Download
XML Download