

 PDF
PDF Citation
Citation Print
Print



Coronavirus disease 2019 (COVID-19) is transforming our ordinary lives; its impact is also affecting the realm of education. Students have been allowed to go back to school only recently since COVID-19 infections decreased after two outbreaks.1 However, most courses at universities have continued to be conducted online since the first semester of 2020. In the beginning, both professors and students experienced much trial and error due to abrupt changes to online classes. The early glitches caused by the technical naivety of faculty members and lack of technical resources were soon resolved. Students, faculty, and institutions adapted rapidly, resulting in higher student satisfaction with online education. Now, online learning has been well accepted by teachers and students as a new, normal approach.
While theoretical lectures can be delivered somewhat flexibly, the anatomy laboratory cannot be optimally learned or taught online. In recent years, the use of various virtual reality (VR)-based anatomy education contents such as augmented reality, VR, and extended reality has been increasing. In particular, in the current pandemic situation, combining online synchronous lectures and VR-based anatomy programs has become a popular tool allowing students to learn anatomical structures while maintaining social distancing.23 However, previous studies have reported that VR-based education methods are less preferred by students and cannot replace on-site anatomy dissection.4 Besides being the best way to acquire knowledge of human body structure, students can learn teamwork and collaboration in small groups and improve their communication skills through interaction with peers and teachers during cadaver dissection. In addition, it is well-known that anatomy dissection laboratories provide an opportunity for students to develop their medical professionalism.567
When considering the advantages of a hands-on anatomy laboratory, it is argued that institutions and educators should make efforts to provide students with valuable experiences in anatomy laboratories despite the current difficult situation.8910 The decrease in the proportion of anatomy laboratories and the increase in the use of 3D models and medical images due to COVID-19 is common in many overseas universities.11 It is evident that online lectures and changes in anatomy laboratory are inevitable. This presents itself as an opportunity to advance methods of teaching anatomy, although most also agree that using an anatomy laboratory is an essential part of anatomy education.111213 Therefore, the authors' medical school finally decided to resume on-site anatomy dissection in mid-April 2020, while many medical schools in Korea continued to postpone anatomy dissection without a concrete reopening plan. This took place when the first COVID-19 surge subsided, and we safely finished the course by maintaining strict infection control measures.
Against our hope, we have faced a new 2021 academic year amidst COVID-19, and teachers have had to prepare the anatomy laboratories in a similar fashion to that of 2020. There were unresolved concerns and doubts about whether cadaver dissection in the on-campus laboratory could be conducted safely. If this was possible, what measures needed to be prepared and observed during the sessions? Against this backdrop, we wish to share our on-site anatomy laboratory experience during the COVID-19 pandemic. We describe the safety measures that were provided to students and how we have improved learning contexts over 2020 and 2021.
While the on-campus anatomy laboratory was suspended from late February to mid-April of 2020, students had to submit assignments using anatomy dissection videos or applications (E-Anatomy®, Complete Anatomy®) to compensate for the lack of cadaveric dissection. As the risk of COVID-19 infection increased along with the number of confirmed cases, online materials were used to help students learn anatomy structures according to the progress of theory lectures. On April 21, 2020, when the number of confirmed COVID-19 patients in Korea had decreased to approximately 10 per day, the authors' anatomy department decided to reopen an in-person dissection laboratory.
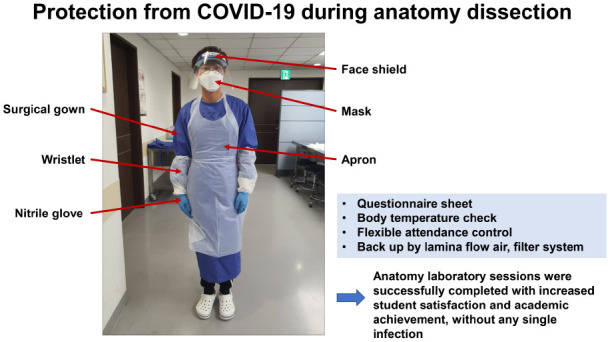
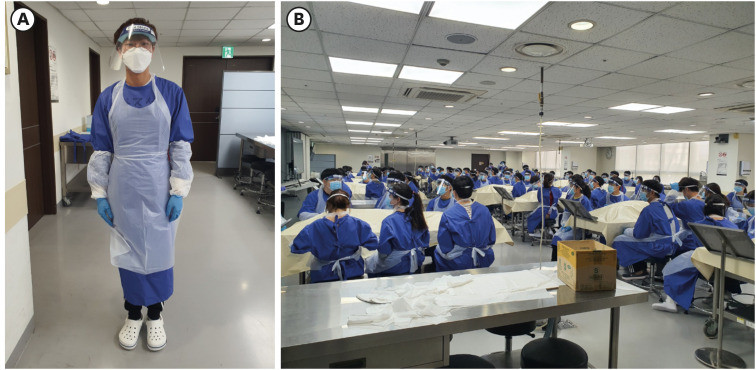
The following strategies were applied to reduce the risk of COVID-19 infection during the face-to-face dissection laboratory sessions. First, the timetable was adjusted to minimize the face-to-face class days. Previously, after a theoretical lecture on one topic, 110 students were organized into 20 groups, and the anatomy laboratory was conducted for 3–4 hours. During the COVID-19 pandemic, the number of days that students had to attend school was minimized, and the content for 2–3 laboratory classes was completed in one day, for 6–12 hours. Total anatomy laboratory hours were reduced to 85 hours in 2020 and 88 hours in 2021, down from 96 hours in 2019 (2020: limbs 20 hours, back 5 hours, thorax 9 hours, abdomen and pelvis 21 hours, head and neck 30 hours; 2021: limbs 24 hours, back 5 hours, thorax 9 hours, abdomen and pelvis 20 hours, head and neck 28 hours). Second, a strict infection management protocol was applied to every class attendee. For checking body temperature, respiratory symptoms, and any possible infection exposure, passing through the entrance system of the Korea University Anam Hospital was recommended. Additionally, the students were required to submit a checklist which included their current body temperature, whether they met a confirmed infected patient, or if they had visited a highly affected area. If students had any suspicious symptoms, they were allowed to rest at home or visit the hospital after reporting it to their teaching assistant in advance. In the case of students who had suspicious symptoms while attending the laboratory, a COVID-19 test was conducted at the hospital infection control office. Personal protective equipment (PPE), including a full body-covering laboratory gown, apron, wristlets, dental masks for respiratory protection, face shields, and nitrile gloves (Fig. 1) was provided to each student. Most of the PPEs were discarded after use in each laboratory class. As face shield was washable and apron, wristlets, nitrile gloves were worn over the laboratory gown, these two were re-used during the semester. Third, in the laboratory, a negative pressure system, an air conditioning system, and six air purifiers equipped with high-efficiency particulate air filters were operated to their maximum to minimize the possibility of possible contagion.
The 2020 dissection laboratory continued for three months until the final examinations for the semester concluded on July 16. Although there were many concerns when the dissection laboratory resumed for the first time, it operated safely in both 2020 and 2021. Appropriate PPE significantly helped to protect the students and faculty, and online teaching materials provided in advance enabled faster and more efficient dissection. In laboratory classes, students showing symptoms of infection such as fever and sore throat were advised to rest at home to prevent contact with other students. For the test, an extra lecture room or an outdoor tent was prepared so that the symptomatic students could take the test. Students were able to have hands-on experience in conjunction with online anatomy theory classes. By using and reviewing what they learned during the class, they were able to understand human anatomy more effectively. The combination of online lectures and face-to-face dissection laboratory sessions led to improved student achievement in anatomy lecture and laboratory tests, and student satisfaction was also high.14
Although the face-to-face dissection laboratory session was safely conducted over the pandemic period, we have faced challenges and limitations. The decreased total anatomy laboratory hours may have limited students' knowledge gain of detailed anatomical structures. To compensate for this problem, the teaching assistants undertook to ensure that students' dissection procedures progressed smoothly without skipping important steps by asking more questions and checking the progress of the dissections in a step-by-step fashion. Consequently, the physical and mental fatigue of the students and the assistants has increased exponentially.15 In 2021, the laboratory schedule was re-adjusted to mitigate this issue: face-to-face dissection sessions were increased to twice a week, and each session was completed within 4–8 hours compared to 10 hours per session in 2020. Increasing the number of attendance days has not been without burden, but given the practical experience of 2020, we assumed that safe practice would be possible with the changes. Although no one was infected during the face-to-face dissection sessions, it cannot be said that our infection control methods completely prevented COVID-19 infection risk. A large group session with 110 students and several assistants in a closed space will inevitably increase the risk of infection. To avoid crowding, the entrance was made through the doors located at both ends of the lab, and PPE was provided in front of each door. Also, we did not check the attendance at the beginning of the class. Further dividing students into 2–3 groups and allocating separate dissection laboratory times to them would be a safer way of preventing infection.
We would like to suggest: first, breaking down smaller groups and cohort management for safer face-to-face anatomy dissection; second, more human resources, including teaching and administrative staff members, should be hired to prepare for similar future situations; and third, introducing diverse online learning materials which supplement anatomy laboratories. In conclusion, the dissection laboratory may be cautiously resumed with the provision of sufficient PPE and a ventilation system as the number of the COVID-19 confirmed cases continues to decline and stabilize.
 XML Download
XML Download