

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Multidrug-resistant tuberculosis (MDR-TB) remains a major public health concern. An estimated 465,000 incident cases of MDR- or rifampicin-resistant (RR)-TB were recorded globally in 2019 and their burden remains stable.1 Treatment outcomes of MDR/RR-TB are still suboptimal; only 57% of MDR/RR-TB patients successfully completed treatment in 2017.1 Treating patients with MDR-TB is challenging due to the less effective and more toxic anti-TB drugs, long duration of therapy, and suboptimal patient adherence.2
Drug susceptibility test (DST) results of MDR-TB patients provide key information for choosing and designing the treatment regimen. Inappropriate regimens not only amplify drug resistance and reduce treatment success of patients, but also increase the risk of transmission of pathogens in the community.34 However, in the absence of individual DST results, recent representative anti-TB drug-resistance surveillance (DRS) data in a province or country are important to guide selection of the regimen.5 Also, as the proportion of MDR/RR-TB patients starting treatment with limited information about the resistance of molecular DST (e.g., Xpert MTB/RIF assay or line probe assay) increases, DRS data are becoming more important for selecting an empirical regimen before full DST results are obtained.
Several nationwide South Korean anti-TB DRSs have been employed for TB patients in the public sector between 1994 and 2004.6 Additionally, several hospitals and laboratories from the private sector have reported phenotypic DST results of TB patients.789 Although previous studies have helped clarify the status and trends of MDR-TB in South Korea, detailed information on additional drug resistance in patients with MDR-TB is lacking.
The authors of a previous study reported the patterns and trends of additional drug resistance in patients with MDR-TB in South Korea using phenotypic DST results collected from seven hospitals from 2010 to 2014.10 Since then, many changes have been made in the diagnosis and treatment of MDR-TB in South Korea: universal use of molecular DSTs, the introduction and increased use of new and re-purposed anti-TB drugs such as bedaquiline (BDQ), delamanid (DLM), linezolid (LZD) and clofazimine (CFZ), and changes in the MDR-TB treatment guidelines. These changes may have affected the status of drug resistance in MDR-TB patients. Therefore, the present study was conducted to update the patterns and trends of additional drug resistance in patients with MDR-TB in South Korea after 2014.
METHODS
Study design and data collection
This retrospective study was conducted at seven university-affiliated tertiary care hospitals in Busan, Ulsan, and Gyeongsangnam-do Provinces of South Korea. The hospitals that participated in this study were the same as in a previous study.10 Patients who were diagnosed with MDR-TB based on the phenotypic DST results between January 2010 and December 2019 were included in the study. Patients with unknown previous TB treatment histories and previously treated patients with unknown regimens or outcomes of their most recent courses of TB treatment were excluded. Duplicate inter-hospital patients were also excluded by checking each patient's initials and birth date. If a patient had more than one DST result, the earlier result was used. If a patient had DST results from both pulmonary and extra-pulmonary specimens, results from the pulmonary specimen were selected. Age, sex, history of TB treatment, type of specimen, date of specimen collection, and results of the phenotypic DST were collected from the medical records.
DST
Six hospitals sent Mycobacterium tuberculosis isolates for the phenotypic DST to the Korean Institute of Tuberculosis, which is a supranational reference TB laboratory, and one hospital sent isolates to the Green Cross Laboratory, a commercial reference laboratory. The workflow used and the references of the critical concentrations did not differ between the laboratories.
The DST was performed using the absolute concentration method and Lowenstein-Jensen medium. The drugs and their critical concentrations for resistance were as follows: isoniazid (INH), 0.2 and 1.0 μg/mL; rifampin (RIF), 40 μg/mL; ethambutol (EMB), 2.0 μg/mL; rifabutin, 20 μg/mL; ofloxacin (OFX), 2.0 μg/mL; levofloxacin (LFX), 2.0 μg/mL; moxifloxacin (MFX), 2.0 μg/mL; streptomycin (SM), 10 μg/mL; amikacin (AMK), 40 μg/mL; kanamycin (KM), 40 μg/mL; capreomycin (CM), 40 μg/mL; prothionamide (PTO), 40 μg/mL; cycloserine (CS), 30 μg/mL; p-aminosalicylic acid (PAS), 1.0 μg/mL; and LZD, 2.0 μg/mL. Pyrazinamide (PZA) susceptibility was determined using the pyrazinamidase test. Critical concentrations for resistance of AMK, KM, OFX, and MFX were changed during the study periods as follows: AMK and KM, 30 μg/mL in January 2014; OFX, 4.0 μg/mL in January 2016; and MFX, 1.0 μg/mL in August 2018. Tests for higher concentrations of INH (1.0 μg/mL as the critical concentration) and LZD have been available since late 2016.
Minimum inhibitory concentrations (MICs) for BDQ and DLM were measured using 7H9 broth medium and the serial two-fold dilution method. The ranges of the concentrations prepared for BDQ and DLM were 0.03125–4.0 mg/L, and 0.00625–0.8 mg/L, respectively. Tests for the MICs of BDQ and DLM have been available since mid-2018.
Definitions
MDR-TB was defined as TB that was resistant to at least INH and RIF. Patients were classified based on a history of TB treatment as follows: new patients, have never been treated for TB or have taken anti-TB drugs for < 1 month; previously treated patients, received 1 month or more of anti-TB drugs in the past.11 Previously treated patients were further classified by the outcomes of their most recent treatment course, such as relapse, treatment after failure, and treatment after loss to follow-up.11 The first-line anti-TB drugs were INH, RIF, EMB, and PZA. SM was considered the first-line drug if it was used to treat drug-susceptible TB; otherwise, it was regarded as a second-line drug. Drug use was defined as the use of an anti-TB drug for 1 month or more in the past.
Statistical analysis
Data are presented as medians with interquartile ranges (IQRs) for continuous variables, and as numbers with percentages for categorical variables. Continuous variables were compared using the Mann-Whitney U test or Kruskal-Wallis test, and categorical variables were compared using the Pearson's χ2 test or Fisher's exact test. The χ2 test for trends was performed to evaluate annual trends in drug resistance and the proportion of patients eligible for the treatment regimen. All tests were two-tailed, and a P value < 0.05 was considered significant. Statistical analysis was performed using SPSS Statistics, version 22.0 software (SPSS Inc., Chicago, IL, USA).
Ethics statement
The study protocol was reviewed and approved by the Institutional Review Board of Pusan National University Hospital (approval No. H-2005-009-090). The need for informed consent was waived given the observational retrospective nature of the study. Our study had no effect on the diagnosis or treatment of patients. Patient information was anonymized and de-identified before analysis.
RESULTS
Patient characteristics
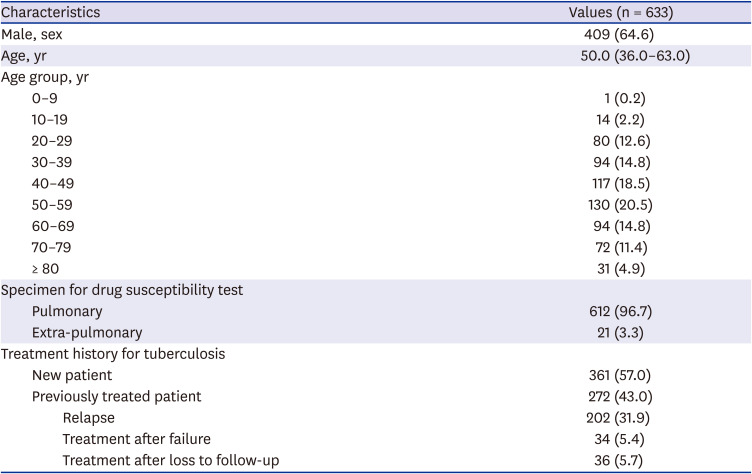
After the criteria defined above were applied, a total of 10,557 culture-confirmed TB patients were screened during the study period. Of them, 633 (6.0%) had MDR-TB and were included in the final analysis. Table 1 lists the baseline characteristics of all MDR-TB patients. Their median age was 50.0 years (IQR, 36.0–63.0) and 64.6% were male. None of the patients had a human immunodeficiency virus infection. The age groups of 40–49 and 50–59 years accounted for the largest proportion of patients. With regard to TB treatment history, 57.0% of all patients were new patients. The proportion of new patients among total patients did not change during the study period. Among 272 previously treated patients, 212 (77.9%) had been treated with first-line anti-TB drugs, and 60 (22.1%) with second-line anti-TB drugs. There were significant differences in the proportions of outcomes of the most recent treatment course between the patients previously treated with first-line drugs and those previously treated with second-line drugs (P < 0.001): relapse (84.9% vs. 36.7%); treatment after failure (6.6% vs. 33.3%); and treatment after loss to follow-up (8.5% vs. 30.0%).
Table 1
Baseline characteristics of patients with multidrug-resistant tuberculosis
Pattern and trend of additional drug resistance
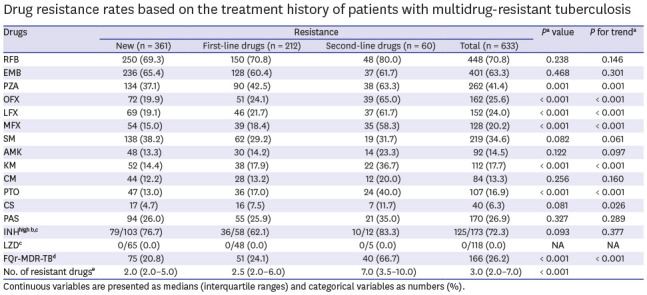
Table 2 lists the rates of additional drug resistance among all MDR-TB patients. All patients had additional resistance to a median of three drugs (IQR, 2.0–7.0) (excluding INH, RIF, a higher concentration of INH, and LZD). The resistance rates of the drugs in groups A and B according to the World Health Organization (WHO) guidelines were as follows12: any fluoroquinolone ([FQ]; OFX, LFX, or MFX; 26.2%), LZD (0.0%), and CS (6.3%). The resistance rates for drugs in group C were: EMB (63.3%), PZA (41.4%), SM (34.6%), PAS (26.9%), PTO (16.9%), and AMK (14.5%). Seventy-two patients (11.4%) had extensively drug-resistant (XDR)-TB (based on a previous definition: TB resistant to any FQ and at least one of three second-line injectable drugs [CM, KM, or AMK], in addition to MDR). The resistance rates of PZA, FQ, KM, and PTO were higher in previously treated patients than in new patients. During the 10-year study period, the resistance rate of PZA tended to increase, whereas that of PAS tended to decrease. However, no significant changes in the trends in resistance were observed to any of the other drugs (Table 3).
Table 2
Drug resistance rates based on the treatment history of patients with multidrug-resistant tuberculosis
Continuous variables are presented as medians (interquartile ranges) and categorical variables as numbers (%).
RFB = rifabutin, EMB = ethambutol, PZA = pyrazinamide, OFX = ofloxacin, LFX = levofloxacin, MFX = moxifloxacin, SM = streptomycin, AMK = amikacin, KM = kanamycin, CM = capreomycin, PTO = prothionamide, CS = cycloserine, PAS = p-aminosalicylic acid, INH = isoniazid, LZD = linezolid, FQr = fluoroquinolone-resistant, MDR = multidrug-resistant, TB = tuberculosis, NA = not applicable.
aComparison of new patients, patients previously treated with first-line drugs and patients previously treated with second-line drugs; bHigher concentration of isoniazid (critical concentration of 1.0 μg/mL); cNumber of resistant patients/total tested patients (%); dMultidrug-resistant tuberculosis resistant to any fluoroquinolone (ofloxacin, levofloxacin or moxifloxacin); eExcluding isoniazid, rifampin, a higher concentration of isoniazid, and linezolid.
Table 3
Trends in the rate of additional drug resistance in patients with multidrug-resistant tuberculosis
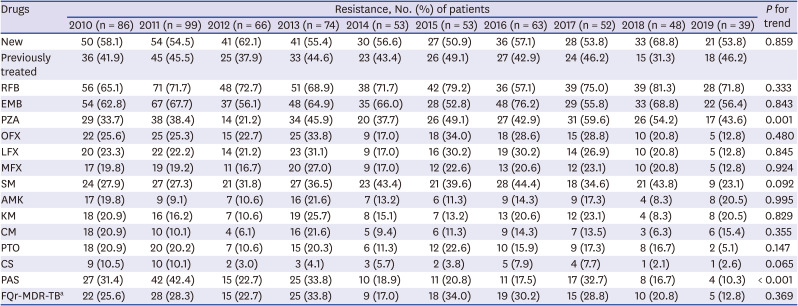
RFB = rifabutin, EMB = ethambutol, PZA = pyrazinamide, OFX = ofloxacin, LFX = levofloxacin, MFX = moxifloxacin, SM = streptomycin, AMK = amikacin, KM = kanamycin, CM = capreomycin, PTO = prothionamide, CS = cycloserine, PAS = p-aminosalicylic acid, FQr = fluoroquinolone-resistant, MDR = multidrug-resistant, TB = tuberculosis.
aMultidrug-resistant tuberculosis resistant to any fluoroquinolone (ofloxacin, levofloxacin, or moxifloxacin).
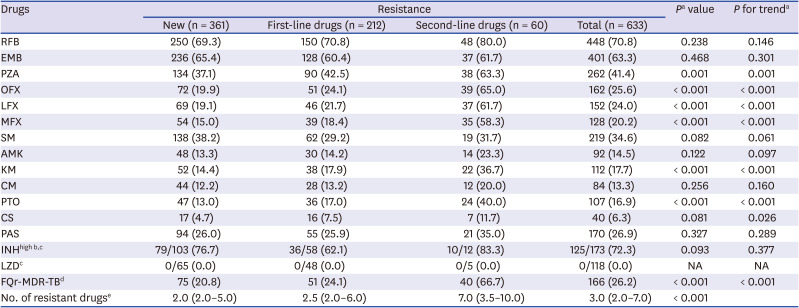
Table 4 compares additional drug resistance rates between FQ-susceptible and FQ-resistant MDR-TB. All drugs except SM, a higher concentration of INH, and LZD had higher rates of resistance in patients with FQ-resistant MDR-TB. The number of additional resistant drugs (excluding INH, RIF, a higher concentration of INH, and LZD) was significantly higher in FQ-resistant MDR-TB than in FQ-susceptible MDR-TB (median of 9.0 vs. 2.0).
Table 4
Comparison of resistance patterns between patients with fluoroquinolone-susceptible and resistant multidrug-resistant tuberculosis
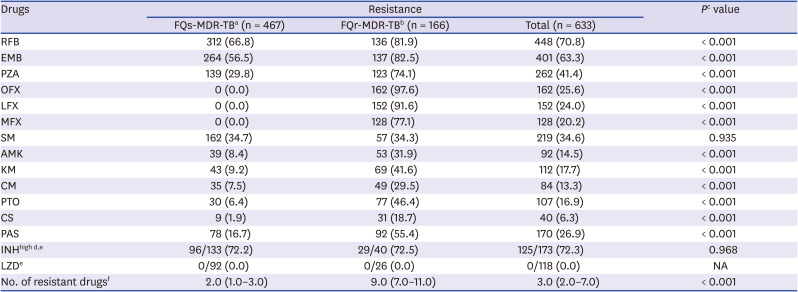
Continuous variables are presented as medians (interquartile ranges) and categorical variables as numbers (%).
RFB = rifabutin, EMB = ethambutol, PZA = pyrazinamide, OFX = ofloxacin, LFX = levofloxacin, MFX = moxifloxacin, SM = streptomycin, AMK = amikacin, KM = kanamycin, CM = capreomycin, PTO = prothionamide, CS = cycloserine, PAS = p-aminosalicylic acid, INH = isoniazid, LZD = linezolid, FQs = fluoroquinolone-susceptible, FQr = fluoroquinolone-resistant, MDR = multidrug-resistant, TB = tuberculosis, NA = not applicable.
aMultidrug-resistant tuberculosis susceptible to all fluoroquinolones (ofloxacin, levofloxacin, and moxifloxacin); bMultidrug-resistant tuberculosis resistant to any fluoroquinolone (ofloxacin, levofloxacin or moxifloxacin); cComparison of patients with fluoroquinolone susceptible and resistant multidrug-resistant tuberculosis; dHigher concentration of isoniazid (critical concentration of 1.0 μg/mL); eNumber of resistant patients/total tested patients (%); fExcluding isoniazid, rifampin, a higher concentration of isoniazid, and linezolid.
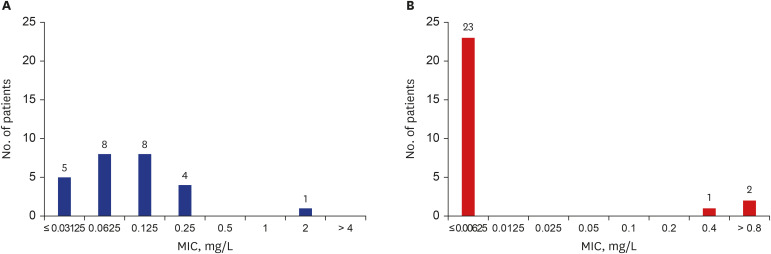
MICs of BDQ and DLM
Twenty-six patients had MIC results for BDQ and DLM. Fig. 1 presents the overall MIC distribution of the patients. When an interim critical concentration of 0.25 mg/L was applied for BDQ resistance,1314 one patient (3.8%) was resistant to BDQ. When the interim critical concentration of 0.016 mg/L was applied for DLM resistance,13 three patients (11.5%) were resistant to DLM; the results remained unchanged if 0.06 or 0.2 mg/L was applied as the critical concentration of DLM resistance.1516 One BDQ-resistant patient had a history of treatment failure with a BDQ- and CFZ-containing regimen. Among the three patients resistant to DLM, one had never been treated for TB in the past, and the remaining two patients had histories of TB treatments with first-line anti-TB drugs only.
Eligibility for the treatment regimen
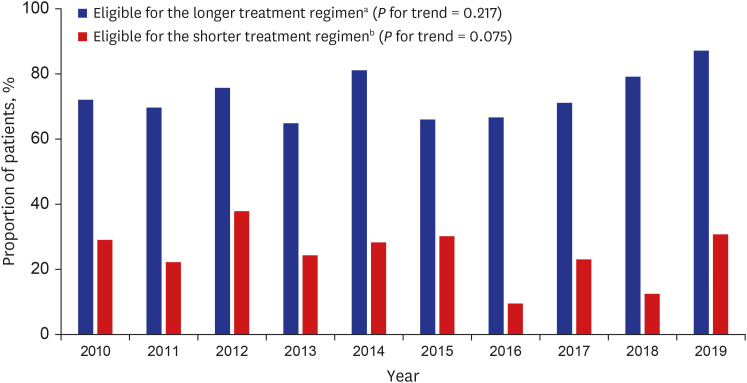
Of all patients, 458 (72.4%) were susceptible to all FQs and CS. Assuming that these patients were also susceptible to BDQ, LZD, and CFZ, they would be eligible for WHO's longer treatment regimen without drug modification.12 In total, 447 patients (70.6%) were eligible for the WHO's shorter all-oral BDQ-containing regimen after applying the inclusion criteria of “MDR-TB patients who have not been exposed to treatment with second-line drugs for more than 1 month, and in whom resistance to FQs has been excluded.”12 However, if the strict inclusion criteria, “MDR-TB patients without resistance to a medicine in the shorter regimen” were applied,12 only 157 patients (24.8%) were fully susceptible to all FQs, PTO, EMB, and PZA, and thus were eligible for the shorter regimen (even if all patients were assumed to be susceptible to both BDQ and CFZ). Fig. 2 presents the annual trends in the proportion of patients eligible for the longer and shorter (with strict inclusion criteria) regimens, respectively. The proportion did not change during the study period.
Fig. 2
Annual trends in the proportions of patients eligible for the World Health Organization longer and shorter multidrug-resistant tuberculosis treatment regimens.
aPatients susceptible to all fluoroquinolones and cycloserine (assuming all patients are also susceptible to bedaquiline, linezolid, and clofazimine); bPatients fully susceptible to all fluoroquinolones, prothionamide, ethambutol, and pyrazinamide (assuming all patients are also susceptible to bedaquiline and clofazimine).
DISCUSSION
In the present study, additional drug resistance of MDR-TB patients was not only high for companion drugs but also for FQ, a core second-line anti-TB drug. The resistance rate did not exhibit a decreasing trend for most anti-TB drugs during the study period. More than half of all MDR-TB patients were classified as new patients, and this proportion did not decrease over time. These findings are not different from those of a previous study,10 suggesting that inappropriate treatment and management of MDR-TB patients is not improving in South Korea.
Because injectables are no longer considered the core drugs to treat MDR-TB, the classification of MDR-TB was simplified to FQ-susceptible or FQ-resistant MDR-TB (the latter is so-called pre-XDR-TB).17 In other words, FQ has increased in importance as a core drug for treating MDR-TB. In our study, the proportion of FQ-resistant MDR-TB among all patients was 26.2%, which is comparable with the global estimate of 20.1%.1 Furthermore, the proportion did not decrease during the study period. FQ-resistance in MDR-TB patients may be due to the widespread uncontrolled use of FQs in the community because FQs are widely used for various infectious diseases.18 Also, suboptimal TB treatment with an FQ-containing regimen and inappropriate patient management may generate and amplify FQ resistance in MDR-TB patients at the individual level.19
The treatment outcomes of patients with FQ-resistant MDR-TB are poor.2021 One of the main reasons for this is the difficulty building an effective treatment regimen due to the high rate of resistance to other drugs. In our study, patients with FQ-resistant MDR-TB had additional resistances to a median of nine drugs. To improve the treatment outcomes of patients with FQ-resistant MDR-TB, it is important to provide an effective empirical treatment regimen based on DRS data and the patient's treatment history until full DST results are obtained. Rapid detection of FQ resistance is also essential for a positive outcome in MDR-TB patients. However, a rapid molecular DST for FQ resistance (e.g., line probe assay for second-line drugs; GenoType MTBDRsl) is not yet widely available in South Korea. The universal use of this rapid test in routine practice is urgently needed. The recently developed Xpert MTB/XDR assay may be promising.
In our study, 72.4% of patients were eligible for the WHO's longer MDR-TB treatment regimen.12 However, this percentage may have been overestimated because only FQ and CS resistance was considered for eligibility. Although resistance to BDQ, LZD, and CFZ was expected to be low as these drugs have not been widely used to treat MDR-TB in South Korea, resistance can occur in the absence of antimicrobial exposure.22 Although standard critical concentrations have not been established, several studies have reported the primary resistances of BDQ, DLM, and CFZ with interim critical concentrations.22232425 In our study, among the 26 patients with MIC results for BDQ and DLM, one and three patients were considered to have resistance to BDQ and DLM, respectively. None of the three DLM-resistant patients had previously been treated with a DLM-containing regimen. These results may be due to true primary resistance, but they may also be due to incomplete DST methods or critical concentrations. Reliable and reproducible DST methods should be established, particularly for new and repurposed anti-TB drugs that are now defined as core drugs. The wide use of these drugs without the support of accurate DST methods will inevitably increase resistance rates.
The WHO recently updated the guidelines for a shorter MDR-TB treatment regimen in which injectables are replaced with BDQ.12 In our study, only 24.8% of patients were eligible for the shorter regimen with strict inclusion criteria. The most common reason for exclusion was resistance to PZA or EMB. However, recent studies have suggested that initial resistance to companion drugs in the shorter regimen (e.g., PZA, EMB, or PTO) has no or minimal effect on treatment outcomes of MDR-TB patients if their isolates are susceptible to core drugs.2627 Also, the phenotypic DST for several drugs, such as EMB and PTO, may not be reliable and reproducible.12 Further investigations are needed to clarify these issues. Until clear evidence of inclusion for the shorter regimen is established, an individualized longer regimen based on DST results is a reasonable choice in the South Korean context.
Primary drug resistance is an indicator of the effectiveness of a TB control program. It reflects suboptimal treatment and management of TB patients and the spread of the pathogen under inappropriate infection control. In our study, more than half of all MDR-TB patients were classified as new patients, and this proportion did not decrease over time. In addition to providing an effective treatment regimen for MDR-TB patients, a comprehensive TB control program that encompasses diagnosis, prevention, patient management, and infection control measures is needed to reduce the transmission of and victims of this difficult-to-treat pathogen.
Our study had several limitations. First, our results were based on regional data derived from seven private hospitals and may not represent the general South Korean population. However, according to the 2019 nationwide notification data, 15.3% of all TB cases in South Korea were reported in our province, and 96.9% of all TB cases were reported from private sectors.28 Second, all hospitals that participated in the study were university-affiliated tertiary care hospitals, so referral or selection bias may have been involved. However, the majority of MDR-TB patients in South Korea are transferred to and treated at tertiary care hospitals. Third, critical concentrations for several drugs changed during the study period, and tests for LZD and higher concentrations of INH could not be performed during the entire study period, which may limit the interpretation of the results.
In conclusion, the proportion of new patients and rates of additional drug resistance in MDR-TB patients in South Korea were high and did not decrease during a 10-year period. Effective treatment for MDR-TB patients in South Korea will require the widespread use of a rapid molecular DST for FQ and the introduction of reliable DST methods for core second-line anti-TB drugs, as well as analyses of nationwide DRS data collected using standardized methods.
 XML Download
XML Download