

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Emergency departments (EDs) are vital elements of health care systems as they form the national medical safety net that provides emergency care, including diagnostic testing and medical stabilization, for all critically ill patients, regardless of their socioeconomic statuses.1 However, a substantial proportion of patients require urgent visit to EDs. Thus, the demand exceeds the availability of ED resources and, consequently, inter-hospital transfer (IHT) of patients between EDs occurs frequently.23 In 2010, in the United States, about 1.5% of the patients in EDs were transferred to other hospitals, and the annual number of patients with transfer admissions increased.4
Clinically essential transfers for specialty care, such as urgent percutaneous coronary interventions for acute myocardial infarction, are important for improving patient care, but patient preference and convenience are other major reasons behind IHTs.567 The potential risks of IHT are disruption of care, miscommunication among medical providers, and missing medical information.78 Given the inherent risks and complex processes, IHTs for ED admission have become a burden to ED physicians, especially in high-level EDs.910
Many previous studies have demonstrated that patients who are transferred show worse outcomes, incur higher medical costs, and require higher medical resource utilization than those who are not transferred.78111213 New strategies are needed to reduce the number of potentially avoidable IHTs and improve the emergency care system. Understanding the characteristics of patients who have undergone IHT is critical for designing effective strategies, especially in cases of double-transfer, i.e., transfer from a medical facility and retransfer to another medical facility. However, this subgroup of patients is understudied at the national level. In this study, we aimed to evaluate the prevalence of IHT in the EDs and to compare the characteristics and ED utilization patterns between patients who undergo single and double transfers between high-level EDs in South Korea using a nationwide prospective database system.
METHODS
Study design and population
This nationwide cross-sectional study used prospectively collected data for 2016–2018 from the National Emergency Department Information System (NEDIS). Since more than 98% of the total national EDs were included in this system, the NEDIS was a reliable source of ED information.14 The quality of the data of NEDIS is maintained by a government-funded national ED control organization. EDs in South Korea are classified into three categories according to hospital function and size: Level I, regional emergency medical centers; Level II, local emergency medical centers; and Level III, local emergency medical institutes. A total of 399 of 401 (99.5%) EDs throughout South Korea are part of the NEDIS: all of the 36 Level I regional emergency medical centers, all of the 117 Level II local emergency medical centers, and 246 of the 248 Level III local emergency medical institutes. The demographic and clinical data of patients were recorded automatically in real time from each ED to the database of the National Emergency Medical Center (NEMC), a representative of the Ministry of Health and Welfare, which qualifies the data.14 Especially, Level I and II emergency medical centers (153 of 401, 38.2%) are obligated to enter specific and reliable clinical data with a low rate of missing data.14 The statistical yearbook of emergency medical service by the NEMC also used the data from Level I and II emergency medical centers.
All the patients admitted to the high-level EDs, defined as Level I and II emergency centers, between 2016 and 2018 were identified. Among them, we included the patients who were transferred to other medical facilities from high-level EDs. We categorized the patients into two groups: single-transfer and double-transfer groups. The single-transfer group included the patients who visited the ED directly or were referred to the ED from outpatient clinics of the same hospital and were subsequently transferred to other medical facilities. The double-transfer group included those patients who were referred to the ED from other medical facilities and were subsequently transferred to a second ED. The characteristics and ED utilization patterns were compared between the two groups.
Data collection
We extracted the following demographic and clinical data of the patients transferred to the EDs from the NEDIS dataset: age, sex, insurance type, ED presentation date, mode of ED arrival, causes of ED visits, primary diagnosis code at ED discharge, length of stay in the ED, type of medical facility transferred to after ED management, and reason for ED transfer. The insurance type was categorized as follows: national health insurance, government-sponsored health insurance (GSHI), private insurance including automobile insurance and industry insurance, and others/unspecified.15 GSHI was designed to relieve the financial burdens of patients with limited income and resources and reduce health disparity. The patients with GSHI were charged minimal co-payments for healthcare services, similar to the Medicaid program in the United States.15 We recorded the primary ED diagnoses using the Korean Classification of Diseases, 7th Revision (KCD-7), updated by the Statistics of Korea and released by the Health Insurance Review and Assessment Service.16 The KCD-7 is based on the International Classification of Diseases, 10th edition, and was nearly identical to it.16 When the patients had cancer codes as their primary diagnosis code (C00–C97), we assumed that they visited the ED for cancer-related problems.17 The Korean Triage and Acuity Scale (KTAS) is a 5-level triage scale, which is a modified version of the Canadian Triage and Acuity Scale, that helps ED physicians to prioritize patient care requirements.18
Statistical analysis
Continuous variables were presented as medians (interquartile ranges) according to their non-normal distribution in the Kolmogorov-Smirnov test. Categorical variables were expressed as absolute numbers (percentages). The comparisons of the demographic and clinical characteristics between the transfer and retransfer groups were performed using the Mann-Whitney U test for continuous variables and the χ2 test for categorical variables. Two-sided P values < 0.05 were considered statistically significant. All statistical analyses were performed using SPSS version 21.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
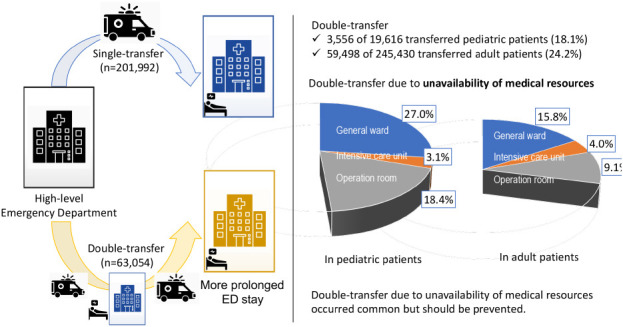
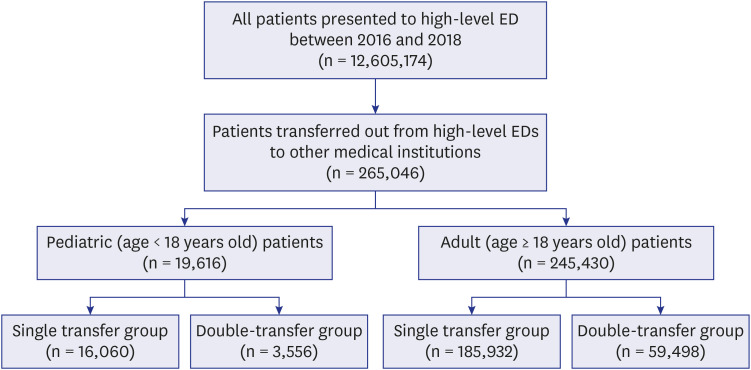
Between 2016 and 2018, 12,605,174 patients visited Level I and II EDs for medical care. Over a 3-year period, 265,046 (2.1%) were transferred from EDs to other medical facilities (Fig. 1). Among the 19,616 pediatric patients, 3,556 (18.1%) patients were transferred from their current ED and further retransferred to another ED, and among the 245,430 adult patients, 59,408 (24.2%) patients underwent double transfers. The absolute number of patients who underwent double transfers increased by 18.0%, from 19,518 in 2016 to 23,025 in 2018.
Characteristics of the transferred patients
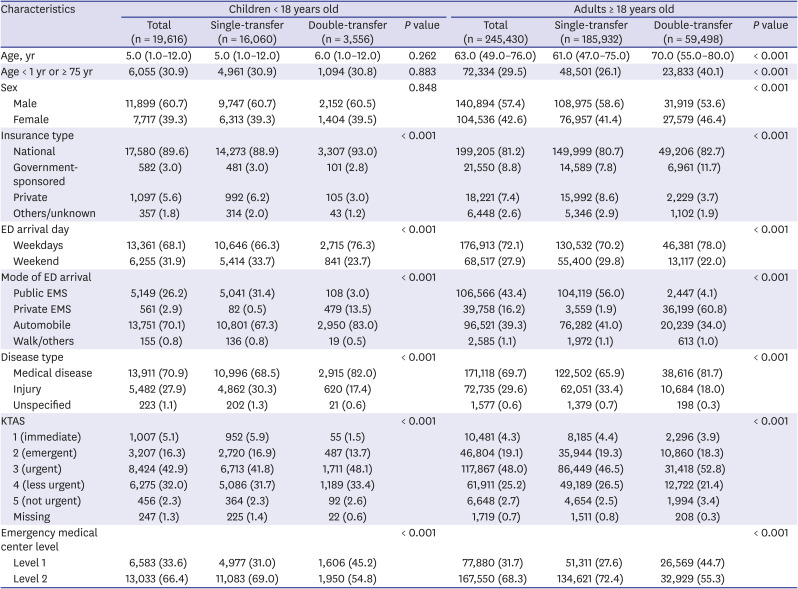
The baseline characteristics of the patients in the single-transfer and double-transfer groups are presented in Table 1. For pediatric patients, the median age was 5 years, with a male-to-female ratio of 3:2, which showed no significant difference between the groups; for adult patients, the double-transfer group consisted of a higher proportion of older patients (median, 61.0 vs. 70.0 years old, P < 0.001) than the single-transfer group, and the former comprised a higher proportion of women than the latter (41.4% vs. 46.4%, P < 0.001). ED visits for medical illness were more frequent, and the proportion of patients who needed immediate or emergent care, i.e., KTAS 1 or 2, was lower in the double-transfer group than in the single-transfer group. Double transfers more frequently occurred in Level 1 EDs than in the EDs of other levels, accounting for 45% of the transfers in both pediatric and adult double-transfer groups.
Table 1
Comparison of the characteristics of the patients in the single-transfer and double-transfer groups
ED utilization patterns of the transferred patients
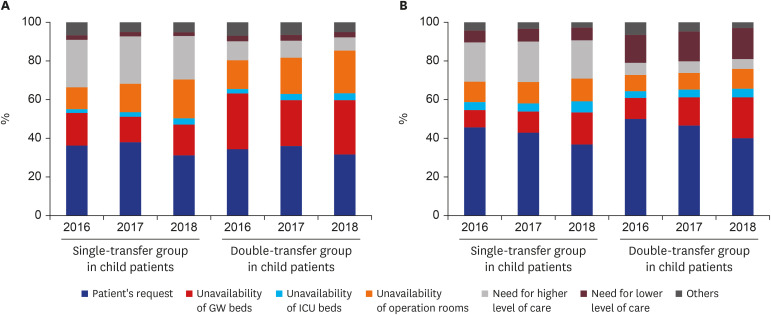
The length of ED stay was prolonged in the double-transfer group among both pediatric (median, 141.0 vs. 208.0 minutes, P < 0.001) and adult populations (median, 189.0 vs. 308.0 minutes, P < 0.001) (Table 2). The proportion of prolonged ED stay of > 12 hours was nearly 2-fold higher in the double-transfer group than in the single-transfer group (children, 4.8% vs. 9.3%; adults, 12.1% vs. 26.2%). Specialty acute care hospital was the most common type of medical facility that the children were transferred to. In the double-transfer group of adults, community hospital was the most common type of medical facility that the patients were transferred to (40.8%), followed by general hospital (34.5%), and specialty acute care hospital (20.4%). The reasons for transfer were different between the single-transfer and double-transfer groups, but patient request was the most common reason. For children, approximately half of the patients (n = 1,725, 48.5%) were retransferred due to the unavailability of medical resources including general ward beds (27.0%), intensive care unit (ICU) beds (3.1%), and operation rooms (18.4%). A total of 17,195 adult patients (28.9%) were also retransferred due to the unavailability of medical resources including general ward beds (15.8%), ICU beds (4.0%), and operations room (9.1%).
Table 2
ED utilization between the patients in the single-transfer and double-transfer groups
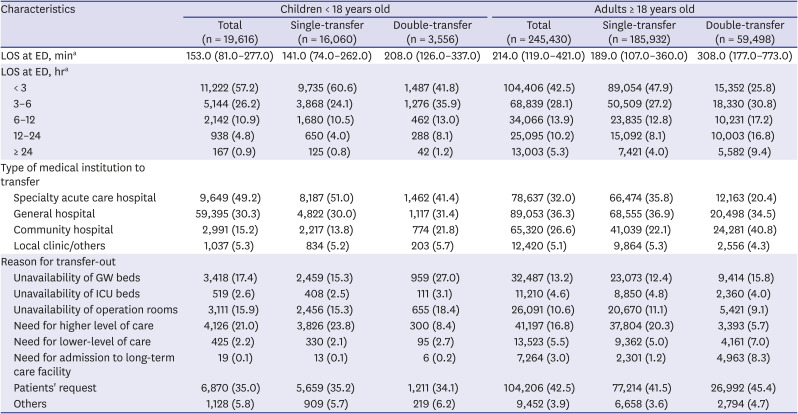
LOS is presented as median with interquartile ranges and categorical variables are presented as numbers (percentage). All the variables showed significant differences with P value < 0.001.
ED = emergency department, GW = general ward, ICU = intensive care unit, LOS = length of stay.
aLength of emergency department stay was not calculated for 3 and 21 patients in the child and adult cohorts, respectively.
For pediatric patients, the proportion of transfers due to the unavailability of operation rooms increased by 77.9% in the single-transfer group, from 11.3% in 2016 to 20.1% in 2018, and by 47.0% in the double-transfer group, from 14.9% in 2017 to 21.9% in 2018 (Fig. 2A). For adult patients, the proportion of transfers due to patients' requests decreased by approximately 20% in both groups, whereas the proportion of transfers due to the unavailability of medical resources increased during the same period in both the groups (Fig. 2B).
ED diagnoses of the transferred patients
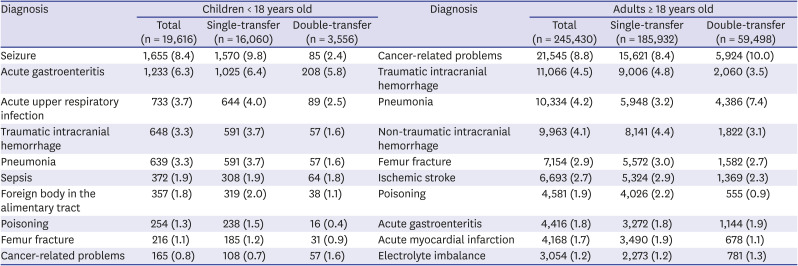
The ED diagnoses at discharge were classified according to the KCD-7 codes (Table 3). The pediatric patients who presented with injury or poisoning (27.1%), unclassified symptoms (20.4%), and diseases of the digestive system (13.6%) accounted for a major proportion of the groups. For adult patients, injury or poisoning (29.0%) was the most prevalent diagnosis, followed by diseases of the circulatory system (14.2%) and the digestive system (13.4%). The 10 top ED diagnoses are presented in Table 4. The most common ED diagnosis in pediatrics was seizures (9.8%), followed by acute gastroenteritis (6.4%) and acute upper respiratory infection (4.0%) in the single-transfer group; it was acute gastroenteritis (5.8%), followed by acute upper respiratory infection (2.5%) and seizures (2.4%) in the double-transfer group. The most common ED diagnosis was cancer-related problems for adult patients in both single-transfer (8.4%) and double-transfer (10.0%) groups. Traumatic intracranial hemorrhage (4.8%) and non-traumatic intracranial hemorrhage (4.4%) were the second and third most common diagnoses for adult patients in the single-transfer group, whereas pneumonia (7.4%) was the second most common diagnosis for those in the double-transfer group.
Table 3
Classifications of emergency department diagnoses according to Korean Standard Classification of Diseases, 7th revision
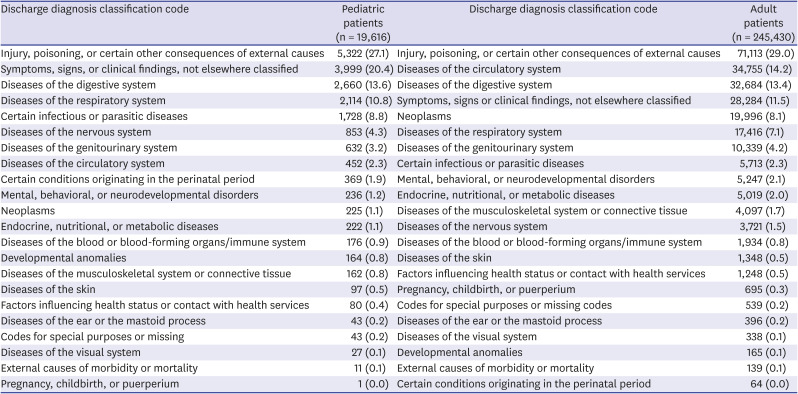
Table 4
Most common emergency department diagnoses in patients in the single-transfer and double-transfer groups
DISCUSSION
This population-based study in South Korea found that more than 1 in 6 transferred pediatric patients (18.1%) and approximately 1 in 4 transferred adult patients (24.2%) were retransferred from EDs to other EDs. The patients in the double-transfer group stayed in the EDs for long durations, with 1 in 10 pediatric patients (9.3%) and 1 in 4 adult patients (26.2%) staying for more than 12 hours in the ED. Patient request was the most common reason for transfer in both single-transfer and double-transfer groups, but unavailability of medical resources, including general ward beds (pediatric patients, 27.0%; adult patients, 15.8%), ICU beds (pediatric patients, 3.1%; adult patients, 4.0%), and operation rooms (pediatric patients, 18.4%; adult patients, 9.1%), were other common reasons for double transfers. Medical diseases such as cancer-related problems (10.0%) and pneumonia (7.4%) were the top two ED diagnoses in adult patients in the double-transfer group.
ED transfers should be conducted carefully, considering the increased risks and costs. The gaps in communication and coordination during the transfers would lead to treatment delays and even dire consequences. In our study, 2.1% (n = 265,046) of the patients who presented to high-level EDs underwent IHTs, and this figure is nearly similar to the rate of IHTs in the US (1.5–1.8%).419 However, the double-transfer patients accounted for over 20% of all the transferred patients in our study, and this figure was approximately 10-fold higher than the proportion reported in a previous study about IHT in patients with sepsis and septic shock in the US.20
Double transfers occurred approximately 1.5-fold more frequently than single transfers in Level 1 EDs, and the patients in the double-transfer group were usually transferred to lower-level EDs. The data suggest that the patients in the double-transfer group were unnecessarily transferred the second time from EDs in high-level hospitals and that inappropriate transfer decisions were made at the time of the first hospital transfer, which could have been prevented.20 Additionally, our study demonstrated that patient request was the most common reason for transfer. Although the reason for the transfer could be recorded differently depending on the physician on duty or the hospital's policy, such a high proportion implied that inappropriate decision-making was prevalent.
The transfer of patients in need of specialized services was relatively low in our cohort, accounting for approximately 20% in the single-transfer group and less than 10% in the double-transfer group. Transfer for specialized care for specific medical conditions such as trauma, poisoning, and myocardial infarction is unavoidable, and timely transfer in such medical conditions can improve the outcomes.20212223 Consistent with previous studies, injuries and poisonings were the most prevalent ED diagnoses in our study.2122 Traumatic intracranial hemorrhage, poisoning, and femur fracture were the major diseases in both pediatric and adult patients, but double-transfer occurred more frequently in adult groups. We hypothesized that the involvement of specialized specialists, such as pediatric neurosurgeons, pediatric orthopedic surgeons, and pediatric general surgeons, and the high risk of medical malpractice lawsuits on post-transfer outcomes in pediatric patients enhance the scope for appropriate transfers. Moreover, these patterns implied that the development and establishment of regional networks can improve the transfer practices and, ultimately, the optimization of medical resources.21
Our study highlights that unavailability of medical resources was the major reason for transfers in the double-transfer group, meaning inappropriate transfers could cause harm in these patients. There should be seamless communication and coordination between the ED physicians who decide to transfer the patients and those who receive the patients to prevent redundant transfers.9 The low absolute number and proportion of transferred patients, especially those who underwent double transfers among the total patients in the ED suggests that IHT is not an urgent problem, but such transfers can burden not only the ED or emergency medical systems because of potential medical errors and depletion of available resources but also the patients and national insurance systems at large because of increased costs.21 Therefore, policymakers and planners who design health systems should focus on these subgroups and consider systematic interventions to improve IHT strategies for ED admission.
The NEDIS was established in 2003 to improve the quality of the national emergency medical care system. The NEMC analyzed the NEDIS data, including the status of ED use, the proportion of urgent patients, and their outcome, stratified by regions to establish national and regional emergency medical system implementation plans and to identify the shortcomings of the emergency medical systems. However, some revisions in the NEDIS data-sharing protocol would provide valuable information to emergency physicians, investigators, and policymakers. For instance, the investigators cannot determine the ED use pattern at the patient level. Although the NEDIS collected and managed the information, it did not provide the specific hospital information about where the patient was transferred to or from and about specific procedures such as embolization and endoscopic interventions during the ED stay.
This study has several limitations. First, the NEDIS data did not provide patient's details in a serial order regarding the information of the first medical facilities and post-transfer outcomes. We could not differentiate between the patients who underwent double-transfer and multiple transfers or determine the reason for the first-transfer in the double-transfer group. The possibility of overlap between single- and double-transfer groups should be acknowledged because some patients in the single-transfer group could have been transferred to another hospital, i.e., double-transfer. Furthermore, duplications of cases in the double-transfer group are also possible when they underwent multiple transfers. Moreover, we could not determine whether double-transfer was associated with worse outcomes or higher medical costs than single-transfer. Second, we could not analyze the interventions or procedures in the ED, which could lead to the overestimation of inappropriate transfers, i.e., transfers due to the unavailability of medical resources. For instance, the patients with cancer at long-term care facilities accidentally remove their percutaneous tubes for ascites drainage and are transferred for a reinsertion of the tube. After the tube insertion in the ED, they are retransferred to a long-term care facility. Such cases could contribute to the high proportion of cancer-related problems (10%) in adult patients in the double-transfer group. Third, we used the primary diagnosis code at ED discharge. However, the diagnosis codes do not reflect the severity of the illness and the coding sequences have inter- and intra-rater variability among hospitals and physicians. Finally, our study used the national data of South Korea, and the utilization patterns of EDs vary across countries and healthcare systems. We did not include the patients who presented to Level III local emergency medical institutes owing to missing data. However, the predominant disease in patients who underwent IHTs showed similarities with previous studies from other countries and suggest the generalizability of the characteristics among these patients.821
In summary, this nationwide cohort study highlights that approximately 1 in 4 patients (23.8%) who were transferred from the ED to other medical facilities underwent double-transfer. Patient's request and unavailability of medical resources were the two most common reasons for transfer. Emergency physicians who would transfer and receive the patients should communicate and coordinate. In addition to the improvement in clinical practices, some specific interventions for transfer decision-making process at EDs, such as enhanced regionalization of specialty care hospitals, standardization of transfer guidelines, and limited telemedicine applications, should also be considered by the committee of emergency physicians and policymakers.
 XML Download
XML Download