

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Intracranial aneurysms (IAs), which may lead to subarachnoid hemorrhage (SAH), are estimated to affect approximately 2% of the population worldwide.123 According to a report published by United Nations, the world's population is growing older, and the number of individuals ≥ 65 years is snowballing.4 In Japan, 23% of the total population was aged ≥ 65 years in 2019. It has been estimated that, by 2030, one in every three people will be ≥ 65 years, and one in five people will be ≥ 75 years. The increased elderly population is likely to play a major role in the increased prevalence of unruptured IAs (UIAs).156 Moreover, the widespread availability of non-invasive imaging has further increased the detection of UIAs.67 The management of UIAs in elderly patients is controversial because the treatment risk in patients with UIAs increases with advanced age and the presence of medical comorbidities.1 Elderly patients are particularly prone to postoperative complications due to comorbidities, high anesthetic risk, and slow recovery rates. However, the development of newer endovascular devices and increased surgical experience have reduced procedure-related risks associated with UIA treatment. Consequently, the age of treatment in elderly patients has also changed.
Several studies have assessed the treatment of UIA in elderly patients.89101112131415161718 However, only a few studies have compared the results of treatment by subdividing the age until the late old age, and a small number of studies have reported the cut-off point of age at which the perioperative risk of clipping and coiling increases. Therefore, we conducted a nationwide cohort study using Korea's National Health Insurance Service (NHIS) data that contains age-specific UIA clipping and coiling outcomes in early and late elderly patients to identify the age at which the perioperative risk of treatment increases.
Go to : 
MATERIALS AND METHODS
Data source
We conducted a retrospective cohort study using the National Health Claim Database, which was availed to us by the NHIS to investigate outcomes in patients who underwent clipping or coiling for UIA between 2004 to 2016. The NHIS is a nationwide universal insurance system in Korea responsible for the nation's health care and medical bills. The database consists of hospital records for 98% of the Korean population. Further, the NHIS operates a Severe Disease Registration System for which strict diagnostic criteria must be met for registration that supports patient's medical expenses. Accordingly, the NHIS database, which covers a single-ethnicity population of 50 million people, is well suited for this epidemiological study. We extracted data exclusively from tertiary referral general hospitals, general hospitals, and semi-hospitals to increase confidence in the medical data. Data from other medical institutions that were not clear were excluded.
Study population and cohort design
Using the International Classification of Diseases, 10th Revision (ICD-10) diagnostic codes, we collected data from patients with UIAs. We identified patients with UIA throughout the assessment period using I67.1 ICD code. Patients diagnosed with UIA were classified based on whether they underwent clipping or coiling. Clipping was specified using Korean Classification of Diseases procedure codes S4641 and S4642, and coiling was indicated using codes M1661 and M1662. Patients who had been diagnosed with brain trauma (e.g., S06–S09), brain tumor (e.g., C41.0, C75.2, C71, C79.3, D32.9-D333, D35.3, or D44.4), stroke (e.g., I60–I63), or experienced morbidity during the preceding 3-year period at any clinic or hospital were excluded to accurately identify and classify cases with new complications such as intracranial hemorrhage (ICRH) or cerebral infarction (CI) that occurred after clipping or coiling. To ensure a 5-year washout period (2004–2008) within the total period (2004-2016), we used data starting from 2009. Thus, the total period of assessment for the reconstructed cohort was 8 years (2009–2016). We assessed changes in the distribution according to the age of the patients and in treatment results over time by aggregating patients in the outcomes cohort into two time blocks. Each group that underwent clipping or coiling was reclassified into group 1, which included patients treated between 2009 and 2012, and group 2, which included patients treated between 2013 and 2016. These time blocks were established because the characteristics of patients do not change noticeably on a yearly basis and the assumption that outcomes might change due to changes in experience and technology.
Outcomes and study variables
According to operation year, both the clipping group and the coiling group were reclassified into group 1 and group 2. Patients aged < 60 were classified into individuals < 50 years old and those 50–59 years old. Patients ≥ 60 were classified within age groups defined using 5-year intervals. We defined “elderly” as the age of 65 years old or older, which was further separated into “early elderly” as those between 65 through 74 years old and “late elderly” as those over 75 years old.1920212223
To analyze perioperative complication incidence, the ICRH (e.g., I60–I62) such as intracerebral hemorrhage (ICH), SAH, subdural hematoma (SDH) or epidural hematoma (EDH), and CI (e.g., I63) within the 3-month period that followed surgery was analyzed according to treatment group and age. Regarding postoperative ICRH, only cases that underwent additional surgery for ICRH that involved hematoma drainage, craniotomy, or craniectomy, and those defined using the following codes: N0321-N0324, S4621, S4622, and N0333, were included in order to exclude clinically insignificant bleeding. To confirm the results one year postoperatively in these patients with perioperative ICRH or CI, the mortality rate and the moderate to severe disability rates during the 1-year period following surgery were analyzed. In Korea, patients with moderate to severe disabilities with a modified Rankin Scale (mRS) of ≥ 3 are assigned a disability rating. If patients have a disability rating, they receive significant financial support. Therefore, most patients with disabilities have a disability rating, and, therefore, accurate data regarding disability could be confirmed.
Data analysis
Data manipulation and extraction were performed using SAS software, version 9.4 (SAS Institute Inc., Cary, NC, USA). All statistical analyses were performed by a biostatistician from the Medical Research Collaborating Center in Seoul National University Bundang Hospital using R statistical software, version 2.8.1. Based on the 2009 demographic structure, the population distribution by age and gender from 2009 to 2016 was standardized to correct for demographic bias of the cohort relative to the structure of the national population. To compare each group, either a chi-square test or Fisher's exact test was used, and values of P < 0.05 were considered significant. The estimated breakpoint (EBP) was calculated using segmented regression analysis to identify the inflection point of the incidence rate according to age. In cases with insignificant EBP values, we noted the ages at which the incidence of complications was significantly higher than those in the younger age group. Only ages that were ≥ EBP were included to identify the age at which the incidence of complications rapidly increases.
Ethics statement
This study was approved by Institutional Review Board at Seoul National University Bundang Hospital (X-1810/498-903), which waived the requirement for informed consent due to the retrospective nature of this study.
Go to :
RESULTS
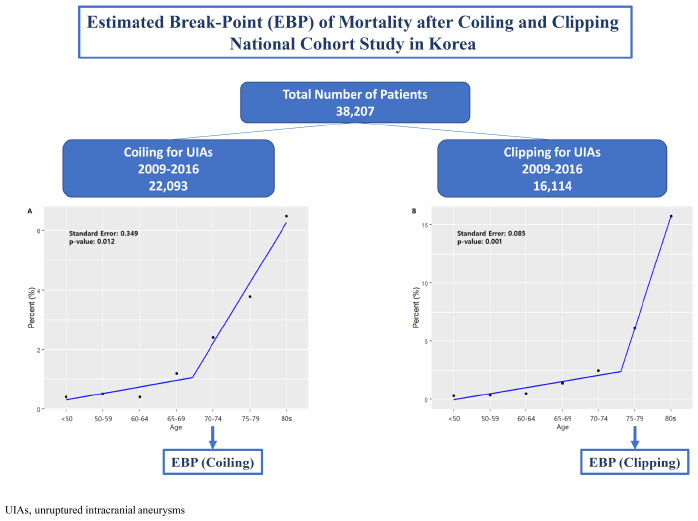
Throughout an eight-year period, a total of 38,207 patients were treated for UIA. Among these, 22,093 (57.8%) patients underwent coiling and 16,114 (42.2%) patients underwent clipping procedures. Among patients who underwent coiling, the proportion of patients over 70 years of age increased from 19.2% in group 1 to 21.3% in group 2. The proportion of patients over 70 years of age who underwent clipping increased from 12.2% to 15.3%. The proportion of patients over 75 years of age increased from 7.3% to 9.5% in patients who underwent coiling and increased from 3.3% to 4.7% in patients who underwent clipping (Table 1).
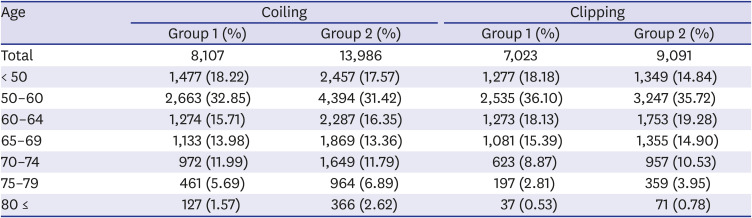
Table 1
Total number of patients underwent coiling and clipping for unruptured intracranial aneurysms
![]()
Postoperative ICRH
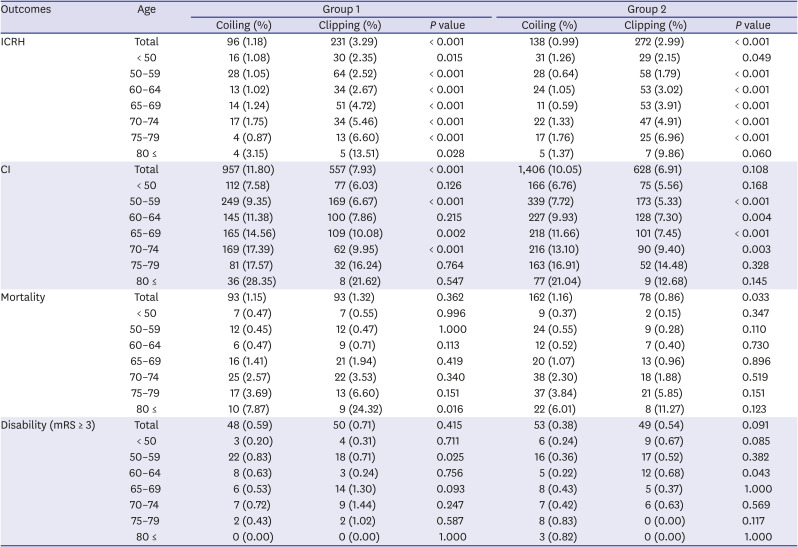
The incidence of ICRH, requiring a secondary operation, within 3-month patients who underwent coiling and clipping within group 2 was 0.99% and 2.99%, respectively. Among these, the ratio of SAH or ICH-related ICRH was 95.7% in the coiling group and 62.9% in the clipping group. On the other hand, only SDH or EDH occurred in 4.3% and 37.1% of patients, respectively. These values were significantly greater after clipping for patients of age groups except those aged ≥ 80 years. In group 2, the incidence of ICRH was 1.13% and 4.81% in patients aged ≥ 65 years that underwent coiling and in those that underwent clipping, respectively. The incidence of ICRH was 1.65% and 7.44%, respectively, in those aged ≥ 75 years (Table 2). The EBP of the incidence of ICRH in patients that underwent clipping was 75 years, and the incidence of ICRH significantly increased in patients aged ≥ 75 years (P = 0.015, standard error [SE] 0.229). Similarly, the EBP of the incidence of SAH or ICH-related ICRH in patients who underwent clipping was 75 years (P = 0.028, standard error (SE) 0.305). The incidence of SDH or EDH without SAH or ICH after clipping was significantly higher in patients aged ≥ 75 years than that in younger patients (P < 0.001, relative risk (RR) 3.56, 95% CI 2.18–5.54) despite non-significant EBP. Even though the EBP was determined to be non-significant (P = 0.079, SE 0.470) in the coiling group, the incidence of ICRH in patients aged ≥ 75 years was significantly higher than that in younger patients (P = 0.013, RR 1.81, 95% CI 1.12–2.89). In addition, the incidence of SAH or ICH in patients aged ≥ 75 years was also significantly higher than that in younger patients (P = 0.039, RR 1.57, 95% CI 1.00–2.36) (Fig. 1A and B). On comparing groups 1 and 2, we found no significant difference in the incidence of ICRH in the coiling group and the clipping group (Table 3).
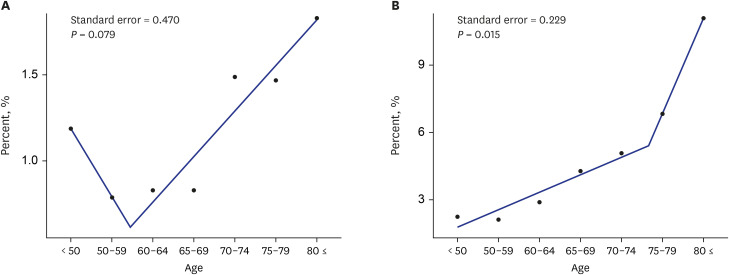 | Fig. 1The EBP of the incidence of ICRH in patients that underwent clipping was 75 years, and the incidence of ICRH significantly increased in patients aged ≥ 75 years (P = 0.015; B). However, there was no significant EBP determined for patients of the coiling group (P = 0.079; A).EBP = estimated breakpoint, ICRH = intracranial hemorrhage.
|
Table 2
The comparison of treatment outcomes for unruptured intracranial between coiling and clipping
![]()
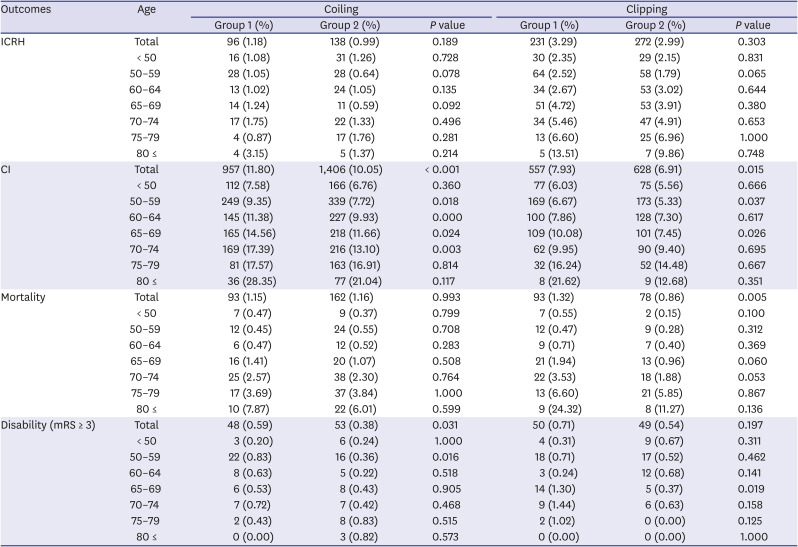
Table 3
The comparison of treatment outcomes for unruptured intracranial between group 1 and group 2
![]()
Postoperative CI
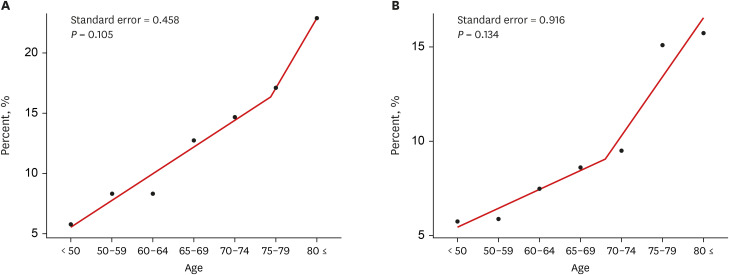
For patients in group 1, the incidence of CI during the post-treatment 3-month period was significantly higher among patients that underwent coiling (11.8%) than clipping (7.9%) (P < 0.01). In group 2, however, patients that underwent coiling (10.1%) experienced CI more frequently than those who underwent clipping (6.91%); however, the difference was not significant (P = 0.110). In group 2, the incidence of CI in those aged ≥ 65 years was 13.90% and 9.19% in the coiling group and clipping group, respectively. These values were higher than the 8.01% and 5.92% incidence rates determined for those aged < 65 years in the coiling group and clipping group, respectively. The incidence of CI in patients aged ≥ 75 years in group 2 of the coiling group and clipping group was 18.05% and 14.19%, respectively. In most patients that were less than 75 years of age, coiling was associated with an increased incidence of CI when compared with clipping. However, in patients aged ≥ 75 years, the incidence of CI in patients that underwent clipping increased and did not significantly differ from those that underwent coiling (Table 2). The EBP of the incidence of CI was 75 years of age (P = 0.105, SE 0.458) in patients who underwent coiling and 70 years of age (P = 0.134, SE 0.916) in those who underwent clipping. However, neither value was statistically significant (Fig. 2A and B). The incidence of CI after coiling in patients aged ≥ 75 years (P < 0.001, RR 1.96, 95% CI 1.72–2.23) and after clipping in patients aged ≥ 70 years (P < 0.001, RR 1.76, 95% CI 1.47–2.10) was significantly higher than that in younger patients. The incidence of CI after both coiling and clipping was significantly reduced in group 2 compared to group 1 (coiling, P < 0.001; clipping, P = 0.010). Moreover, the incidence of CI tended to be lower in group 2 compared to group 1 among patients of all ages (Table 3).
Postoperative mortality and disability
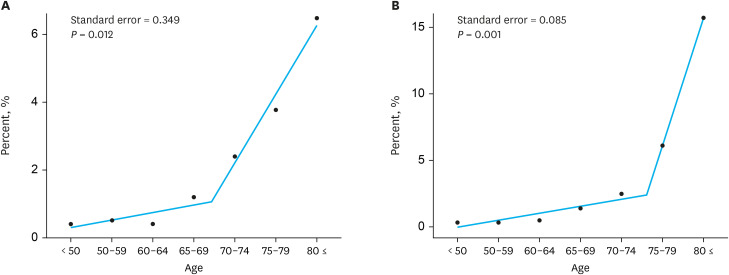
Mortality within the 1-year period that followed treatment in patients with perioperative ICRH or CI did not show a significant difference between the coiling group (1.15%) and clipping group (1.32%) in group 1. However, clipping (0.86%) was determined to be associated with significantly lower mortality than coiling (1.16%) in group 2. The mortality rates for coiling groups and clipping groups in patients aged ≥ 65 were 2.41% and 3.39%, respectively. Mortality rates in patients aged 75–79 years who underwent coiling and clipping were 3.84% and 5.85%, respectively (P = 0.151). For those aged ≥ 80, mortality rates associated with coiling and clipping were 6.01% and 11.27%, respectively (P = 0.123). Although not statistically significant, the mortality rates tended to be higher in patients aged < 75 years in the coiling group than those in the clipping group. In contrast, the mortality rates tended to be higher in patients aged ≥ 75 years in the clipping group than those in the coiling group (Table 2). No significant difference was observed in mortality among patients that underwent coiling between group 1 and group 2. However, mortality after clipping was significantly reduced (P = 0.010) (Table 3). EBP analysis revealed that mortality increased in patients that underwent coiling in patients aged ≥ 70 years (P = 0.012, SE 0.349) and in patients that underwent clipping aged 75 years (P < 0.01, SE 0.085) (Fig. 3A and B).
The rate of disability among patients with perioperative ICRH or CI at a level of mRS 3 or greater in group 2 was 0.38% for patients that underwent coiling and 0.54% for patients that underwent clipping, and no significant difference was observed between the two groups (P = 0.091). In patients aged ≥ 65 years, disability rates were 0.54% and 0.40% for the coiling group and the clipping group, respectively (Table 2). Additionally, when rates of disability in group 1 and group 2 were examined individually, the disability rate was significantly lower in group 2 for patients that underwent coiling (P = 0.031), while disability tended to decrease in patients that underwent clipping. However, the difference was not significant (P = 0.200) (Table 3).
Go to :
DISCUSSION
Several papers have reported outcomes of clipping and coiling in elderly patients with UIA.8910111213141516171824 However, the ages of elderly individuals in these studies have not been consistent, and large-scale studies assessing outcomes stratified by age are rare.81116 This study assessed treatment outcomes stratified according to population age, including the late elderly, and revealed trends associated with outcomes of UIA over time. Most importantly, EBP values were calculated to identify the appropriate age at which the risk of treatment for UIA rapidly increases.
Most studies to date have classified those individuals aged ≥ 65 years as elderly patients. In previous studies, the incidence of ICRH in patients aged ≥ 65 years was reported to be 0.3–3.9% among patients who underwent coiling and 0.2–5.1% among patients who underwent clipping.8121417 Although the incidence of ICRH was elevated in patients aged ≥ 65 years compared with patients aged < 65 years, the difference was not statistically significant.8 We identified 75 years of age in the coiling and clipping groups as the age at which ICRH incidence increased significantly. The incidence of ICRH was significantly higher than that noted in younger individuals above the age of 75.
Similar to the results of our study (coiling, 13.90%; clipping, 9.19%), a previous study determined that the incidence of CI in elderly patients aged ≥ 65 years was 2.9–8.9% among patients who underwent coiling and 2.2–10.3% among patients who underwent clipping. Differences between the incidence of CI in the two groups were conflicting.81213141718 However, it was reported that CI occurred significantly more frequently in older individuals (≥ 65) than those who were younger (< 65).81718 Despite the non-significant EBP in our study, the incidence of CI in patients whose age was above the EBP age (age ≥ 75 years in coiling group and age ≥ 70 years in clipping group) was significantly higher than that in patients in younger age groups. The relatively high incidence of CI observed in this study was likely because the study included both patients with major infarction and those with minor infarction that exhibited mild symptoms, as evident from the low mortality rate and disability (mRS ≥ 3) rate compared to the high incidence of CI.
Previous studies have shown that mortality rates within one year of treatment in patients aged ≥ 65 were 7.6–10% for those who underwent coiling and 5.9% for patients who underwent clipping.1013 Mortality rates within 30 days were reported to be 0–1.9% for patients who underwent coiling and 0.2–3.2% for patients who underwent clipping.8910121718 For those over 80, the mortality rates were 2.4% and 6.3–21.4% for coiling and clipping, respectively.815 There was no significant difference between prior and current findings. However, as a key finding of this study, mortality rates were found to increase dramatically and significantly after the age of 70 in patients who underwent coiling and after the age of 75 in patients who underwent clipping.
Post-treatment neurological deficits in elderly patients aged ≥ 65 years who underwent coiling were 3.0–5.6% and 2.8–17.3% in patients who underwent clipping. The values rose to 9.8% and 33.5% in patients aged ≥ 80 years who underwent coiling and clipping, respectively. When rates of deficit in older individuals were compared to individuals aged < 65 years, it was demonstrated that rates in patients of advanced age were significantly elevated.811131517 We analyzed the incidence rate of moderate to severe disability (mRS ≥ 3). However, it is likely that our statistical analysis was limited by the low number of treatments performed in very old aged individuals relative to incidence. Further, as evident from our study results, mortality is high compared to very low cases of disability at age ≥ 75 years. Accordingly, it is assumed that the disability rate at age ≥ 75 could have been underestimated because moderate to severe disability can lead to mortality when ICRH or CI occurs at age ≥ 75.
A nationwide study conducted during 2000–2010 in the United States of America found that the number of elderly patients aged 65–74 years who underwent coiling or clipping for UIA had increased by 47.4%.9 Furthermore, a comparison of a group that received treatment between 2001 and 2003 with the group that received treatment between 2008 and 2010 revealed that both 30-day mortality and complication rates decreased over time, with the same results also being observed in elderly patients.9 In our study, when comparing group 1 and group 2, the number of patients over 70 years of age who underwent coiling or clipping treatment for UIA had increased by 91.0% and 61.5%, respectively. Similar to the results from previous studies, ICRH, CI, and mortality rates appeared to decrease among patients in group 2 than those in group 1. Notably, the incidence of postoperative CI after coiling and clipping, the mortality rate after clipping, and disability rate after coiling were significantly decreased.
In summary, the likelihood of experiencing complications including ICRH, CI, mortality, and disability increases significantly with age. Furthermore, ICRH, CI, and mortality rates begin to increase rapidly at 70 or 75 years. Based on these findings, when deciding the treatment of elderly patients aged ≥ 70 years with UIA, the risk of treatment should be carefully compared with the spontaneous rupture rate. Moreover, because the risk of treatment shows a decreasing trend over time, which is likely due to advancements in the performance of endovascular techniques, general improvements in postprocedural care, and increased past-year clipping and coiling volumes, it is estimated that in the future, the age range eligible for UIA will have to be further increased.2526
A limitation of this study is that the NHIS data did not contain information regarding the location and size of UIA or the use of stent or antiplatelet drugs, which are associated with the incidence of ICRH and CI. Moreover, the nature of the NHIS data meant that if the underlying diseases were to be included as variables, the number of study subjects, especially the number of late elderly patients, would significantly decrease. Therefore, a population analysis was performed to sufficiently assess late elderly patients, for which variables other than age and sex were excluded. However, the data used in the study comprised 98% of the total population, and, therefore, it may be considered valuable in evaluating the treatment outcomes in practice. Another limitation was the lack of information regarding the accuracy of measurements such as mRS for neurological disorders that occurred during the long-term patient follow-up. Although moderate to severe sequelae (mRS ≥ 3) were identified with mortality and disability levels, no information regarding the occurrence of mild level neurologic deficit was available. In addition, although most patients with severe disabilities are enrolled in the disability registration system, there is a possibility that the incidence of disability is slightly underestimated because a small number of patients are occasionally omitted. Therefore, a large-scale multicenter prospective study will be necessary to analyze the natural course of UIA and treatment outcomes in elderly patients.
In conclusion, the risk of treatment in elderly patients diagnosed with UIA increases with age, and this also increases dramatically in patients aged ≥ 70 years. Therefore, the eligibility for treatment among patients aged ≥ 70 years should be determined carefully after considering the following factors: the natural course of UIA, the patient's general condition, preoperative comorbidities, and the patient's life expectancy. In addition, more attention and focus are required throughout the surgical processes, including administration of anesthesia and postoperative management.
Go to :
 XML Download
XML Download