

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cervical intraepithelial neoplasia (CIN) is known to progress to invasive cervical cancer in some cases.1 Patients with more progressive disease have the higher risk for malignant transformation. The overall prevalence of high-risk human papillomavirus (hrHPV) was calculated at 12% in normal cytology while hrHPV was positive in 89% of cervical cancer cases.2 In Korea, human papillomavirus (HPV) testing is currently recommended to triage women with abnormal cytology and the combined test of cervical cytology with HPV genotyping has reduced the incidence rate of cervical cancer.3
Colposcopy is the most common procedure performed in patients referred for cervical cytologic abnormalities. It facilitates detailed localization of the suspected cervical lesion, determines its severity, and eases biopsy.4 Colposcopic biopsy is primarily used to discriminate high-grade from low-grade lesions, in order to limit unnecessary surgical excision of the cervix.5 In addition, it differentiates CIN lesions from invasive cervical cancer and enables ablation treatment.6
A number of patients undergoing colposcopic biopsy after cervical cancer screening were diagnosed as low-grade intraepithelial lesions.7 Low-grade lesions (CIN1) were unlikely to progress to invasive carcinoma (CIN3).8 In fact, the risk of progression to a high-grade lesion was not significantly different in no CIN as well as CIN1 patients.
Inconsistencies between cervical cytology and colposcopic biopsy histology can lead to confusion in diagnosis and clinical management.9 Investigating this discrepancy and factors influencing it, are needed to avoid excessive unnecessary testing and underdiagnoses of high-grade cervical lesions. Therefore, we aimed at investigating the discrepancy between cytology and histology in cervical cancer screening.
METHODS
Study population
A multicenter retrospective analysis was performed in this study. Patients with both cervical cytology and HPV test followed by colposcopic biopsy of cervix between January and December 2018 were identified at thirteen certified tertiary hospitals (Supplementary Data 1). The inclusion criteria was for patients who underwent HPV test of HPV genotypes including HPV 16/18, so patients who did not have data for HPV genotypes such as Hybrid Capture II were excluded.
Data collection
Baseline characteristics including age, height, weight, and parity were obtained from patients. Cytological, histologic, and HPV-genotype results were recorded in database. Patients without data on cytology or HPV DNA tests were excluded from the analyses. All patients with abnormal cytology and/or positive for HPV were referred participating institutions.
To analyze the risk of discordance of cytology and histology, body mass index (BMI) over 25 is defined as overweight. In addition, the risk was analyzed before and after 45 years old, the age of generally entering perimenopause.10
The patients' group as HPV 16/18 was representative to not only positive for HPV 16 and/or 18, but also to co-infected with other hrHPV groups. HPV others included patients who were positive for hrHPV genotypes except for HPV 16 and 18.
Definition of correlation
Overcall was defined as the patients whose cervical smear result of atypical squamous cells cannot exclude high-grade squamous intraepithelial lesion (ASC-H)/high-grade squamous intraepithelial lesion (HSIL) or higher grade lesion followed by cervical biopsy showing negative or CIN1.11
Undercall was defined as the patients whose cervical smear result of negative for intraepithelial lesion or malignancy, atypical squamous cells of undetermined significance (ASCUS) followed by cervical biopsy showing CIN2 or higher lesion.
Statistical analysis
Baseline data are presented as mean ± standard deviation for continuous variables or frequency (%) for categorical variables. A logistic regression model was used to evaluate the odds ratio (OR) and 95% confidence intervals (CIs) to predict the results associated with epidemiological characteristics. All P values less than 0.05 were considered statistically significant. Data were analyzed using SPSS software (version 22.0; SPSS Inc., Chicago, IL, USA).
Ethics statement
The Institutional Review Board of the National Evidence-based Healthcare Collaborating Agency (NECA) in Korea approved the study (IRB No. NECAIRB19-015-2). The IRB of each institute approved the collection of data within a database of each institution. Information obtained from patients was coded for analysis, so the requirement for informed consent or parental permission was waived.
RESULTS
A total of 3,798 patients tested for hrHPV and cervical cytology, followed by colposcopic biopsy met the inclusion criteria. The baseline characteristics of the patients are displayed in Table 1. The mean age was 42.7 (19–88) years and mean BMI was 22.5 (16.9–34.1) kg/m2. Nine-hundred seventy (25.5%) patients were nulligravida and 1,109 (29.2%) were nulliparity. The most prevalent cytological abnormalities referred for colposcopic biopsy was ASCUS (1,390 patients, 36.6%). In addition, 495 patients (13.0%) were normal, 380 (10.0%) were ASC-H, 792 (20.9%) were low-grade squamous intraepithelial lesion (LSIL), and 593 (15.6%) were HSIL. HPV was positive for 3,008 (79.2%) and HPV 16/18 was found in 914 (24.1%) patients. Various types of HPV tests were used (Supplementary Table 1), of which Anyplex II HPV 28 (Seegene), the most common, was performed in 1,358 (35.8%) of all patients.
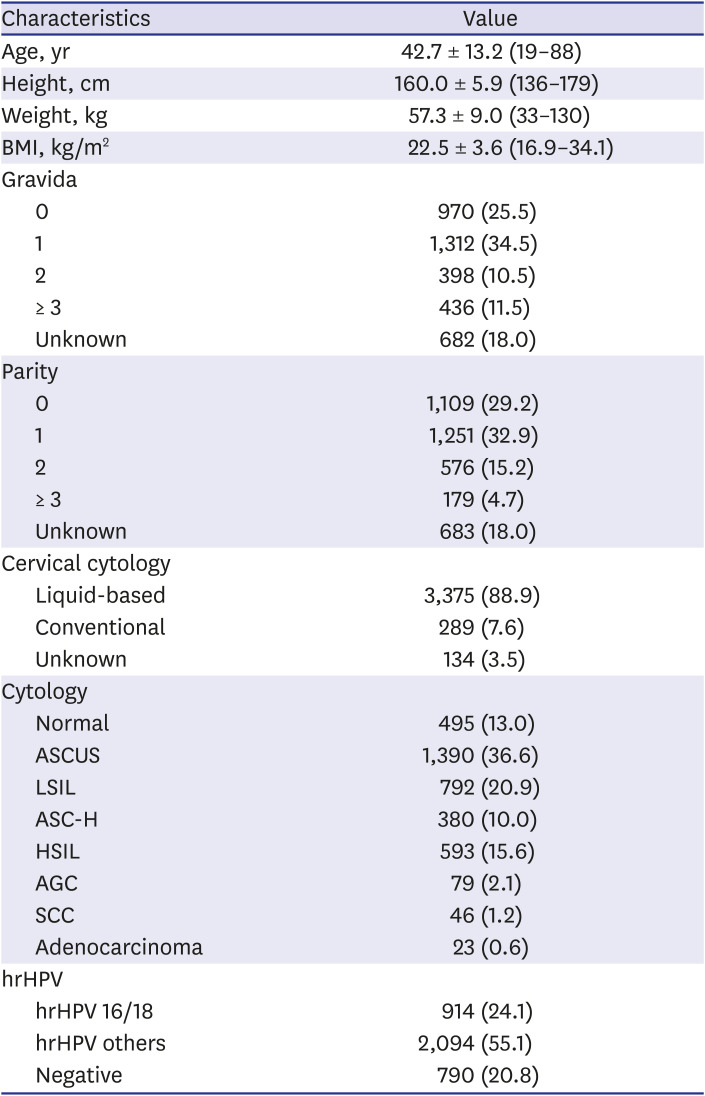
Table 1
Overview of patients' baseline characteristics (n = 3,798)
Values are presented as mean ± standard deviation (range) or number (%).
BMI = body mass index, ASCUS = atypical squamous cells of undetermined significance, LSIL = low-grade squamous intraepithelial lesion, ASC-H = atypical squamous cells cannot exclude high-grade squamous intraepithelial lesion, HSIL = high-grade squamous intraepithelial lesion, AGC = atypical glandular cells, SCC = squamous cell carcinoma, hrHPV = high-risk human papillomavirus.
![]()
Distribution of hrHPV positivity and cytologic findings in relation to histologic results were shown in Table 2. In patients with CIN, the positive rate of hrHPV was 64.9%, and HPV 16/18 was positive in 13.1%. On the other hand, in patients with CIN3, the positive rate of hrHPV was 95.6%, and the 69.5% of patients were positive for HPV 16/18. In particular of 128 patients with carcinoma on histologic finding, 10.9% of patients were negative for hrHPV. Among the patients with no CIN, ASCUS in the cytology result were most common (50.7%), followed by normal cytology (21.4%). The preceding cytology findings of patients with CIN1 were most common in the order of ASCUS (38.2%) and LSIL (36.1%), and in patients with CIN2, ASCUS (31.4%) and LSIL (26.6%) were the most common. In CIN3, HSIL was the most common with 43.4%, followed by ASC-H with 20.6%.
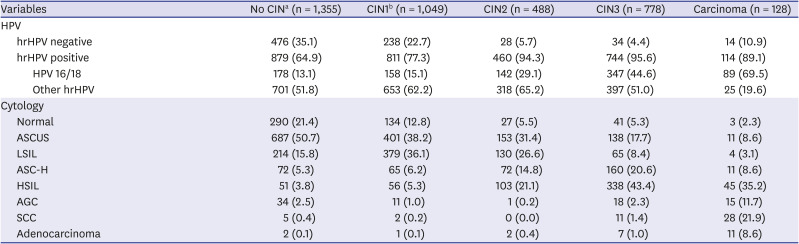
Table 2
Distribution of hrHPV types and cytologic findings in relation to histology lesions (n = 3,798)
Values are presented as number (%).
hrHPV = high-risk human papillomavirus, CIN = cervical intraepithelial neoplasia, HPV = human papillomavirus, ASCUS = atypical squamous cells of undetermined significance, LSIL = low-grade squamous intraepithelial lesion, ASC-H = atypical squamous cells cannot exclude high-grade squamous intraepithelial lesion, HSIL = high-grade squamous intraepithelial lesion, AGC = atypical glandular cells, SCC = squamous cell carcinoma.
aNo CIN included inflammatory changes as well as normal; bCIN1 included koilocytic changes.
![]()
We investigated the overcall defined as unexpected low-grade results as ≤ CIN1 from colposcopic biopsy from patients referred for abnormal cytology (≥ ASC-H). This amounted to 299 patients in the study. To investigate the associated factors, we performed a logistic regression analysis of variables. The OR of overcall was higher in age ≥ 45 (OR, 2.137; 95% CI, 1.475–3.096) as shown in Table 3. Multiparous women were a higher risk group at overcall compared to nulliparous women, but insignificant in multivariate analysis (OR, 1.090; 95% CI, 0.775–1.535). Overweight (BMI ≥ 25) infection was not associated with overcall while HPV 16/18 were at lower risk of overcall compared to other hrHPV or HPV negative (P < 0.05). Conversely, the findings of undercall defined as ≥ CIN2 following referral was ≤ ASCUS in 373 patients (Table 4). Patients aged over 45 years (OR, 0.530; 95% CI, 0.376–0.747) were at lower risk while HPV 16/18 positive cases were at higher risk for undercall compared to other hrHPV or HPV negative (P < 0.01). On the other hand, BMI or parity did not affect the results of colposcopy.
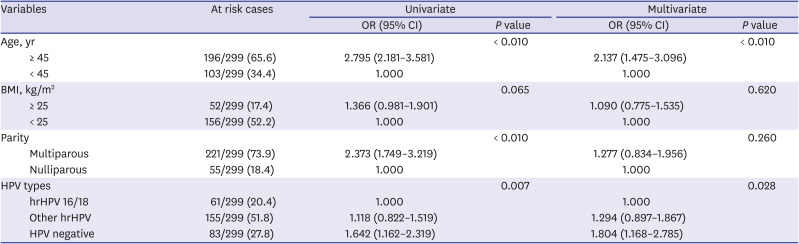
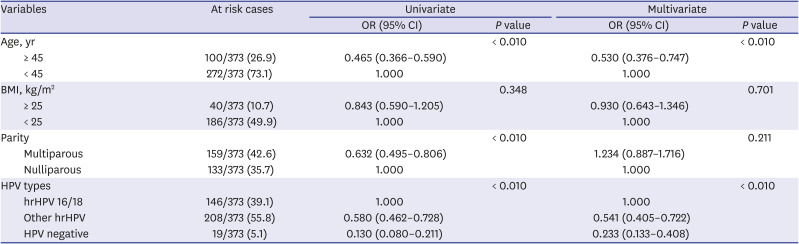
Table 3
Logistic regression results for predicting the ≤ CIN1 following ≥ ASC-H (overcall) (n = 299)
Values are presented as number (%).
CIN = cervical intraepithelial neoplasm, ASC-H = atypical squamous cells cannot exclude high-grade squamous intraepithelial lesion, OR = odds ratio, CI = confidence interval, BMI = body mass index, HPV = human papillomavirus, hrHPV = high-risk human papillomavirus.
![]()
Table 4
Logistic regression results for predicting the ≥ CIN2 following ≤ ASCUS (undercall) (n = 373)
Values are presented as number (%).
CIN = cervical intraepithelial neoplasm, ASCUS = atypical squamous cells of undetermined significance, OR = odds ratio, CI = confidence interval, BMI = body mass index, HPV = human papillomavirus, hrHPV: high-risk human papillomavirus.
![]()
DISCUSSION
This study investigated the current overall status of colposcopic biopsy and analyzed the associated factors for the discrepancy between cytology and colposcopic biopsy histology in Korea. The most common cytological finding referred for colposcopy was ASCUS, followed by LSIL, HSIL, and normal cytology. Age and HPV-genotypes affected the discrepancy between cytology and colposcopic biopsy histology. The unexpected colposcopic biopsy histology in negative or CIN1 findings following cytology of ASC-H or higher grade was found in 299 patients. Patients over 45 years and hrHPV others (compared to HPV 16/18) were at higher risk for initially overestimated before cervical biopsy. In contrast, patients under 45 years were at higher risk for underestimated before cervical biopsy. As expected, HPV 16/18 were at higher risk for high-grade lesions than hrHPV others. When targeting for colposcopic biopsy following cervical cancer screening, HPV genotypes, age, and cytology should be considered.
Immature squamous metaplasia or air-drying artifacts have been known as factors influencing the discrepancy between cytology and histology.12 In addition, infectious cause such as bacteria or fungi will reduce the accuracy of cytology. Unlike our findings were patients' age was associated with the accuracy of cytology, previous studies have demonstrated the accuracy of Pap smear in diagnosing cervical intraepithelial lesions by comparing the characteristics of cervical dysplasia versus non-dysplasia.13 Age, smoking, number of abortions, age at first delivery, and number of sexual partners were not significantly different across both groups. HPV infection is the most important factor, though the genotypes were not investigated.
In our study, histology results tended to be of lower grade compared to those of combined cytology with HPV, in patients over 45 years. First, this can be explained by the fact that the squamous-columnar junction of menopausal women was deeper in the cervical canal than that of pre-menopausal women, thus rendering colposcopic examination unsatisfactory.14 Unfortunately, the results of cervical biopsy (loop electrosurgical excisional procedure [LEEP] or conization) were not included in our data, so further analysis was limited. Second, atrophic changes in postmenopausal women (caused by estrogen deficiency) could lead to confusion in the cytological diagnosis of Pap smear because they may simulate high-grade lesions.15 The cervical mucosa develops a morphological diversity with age, while dysplasia decreases with age.16
HPV has genotype-specific risk for high-grade lesions and cancer. HPV 16, 18, and 58 are associated with significant risk of CIN3 and invasive cancer.17 HPV testing was approved as a primary screening method by Food and Drug Administration (FDA) in April 2014. We found out that the ratio of HPV 16/18 to hrHPV others was higher in ≥ CIN3 lesions compared to ≤ CIN2 lesions. Colposcopy is recommended for HPV 16/18 infected patients, regardless of cytology findings in the Australian Society for Colposcopy and Cervical Pathology.18 Furthermore, HPV 16/18 infections can be prevented by vaccination fortunately.
Various assays for detecting and genotyping HPV have been introduced in Korea. Among them, the Hybrid Capture 2 HPV test was the first assay detecting 13 hrHPV, which has been approved by the U.S. FDA. Subsequently, various assays to detect hrHPV genotypes including HPV 16 or 18 by real-time polymerase chain reaction were introduced, and the Roche Cobas HPV assay was approved by the U.S. FDA in 2011. Various HPV genotype assays which were investigated in our study are currently used in Korea, and their usefulness has been proved in several literatures.192021222324
CIN1 is not considered a precursor of CIN3 or invasive carcinoma. CIN1 is not a target for screening and should not be managed but recommended for observation. However, the accuracy and reproducibility of cervical cytology are limited.13 Cytology diagnosis accuracy mainly depends on the pathologists' experience and the characteristics of patients.25 Recently, several studies show that a reduction in unnecessary colposcopy and induce objective cytology results. MicroRNAs (miRNAs) expression underlies the carcinogenesis.26 Cervical exfoliated cells can be used for miRNA detection in the diagnosis of cervical lesions. In fact, miRNAs expression as a cervical cancer screening tool, not only induces accurate cytology, but also detects high-grade lesions that would be missed in histology.27 Killeen et al.28 evaluated whether stain for p16 and Ki-67 improve the triage of abnormal Pap smears. Immunostaining was of value in selecting abnormal cytology and had diagnostic accuracy.
This study is the first multicenter analysis about patients who underwent colposcopic biopsy in Korea. Limitations encountered in the study include its multicenter retrospective design and the diverse indications of colposcopy across centers. In addition, final histology of cone or LEEP specimen could not be obtained. Nevertheless, the histologic results from colposcopic biopsy are critically enough to have a significant impact on the course of treatment. Although a large-scale study was conducted on patients with colposcopic biopsy, referred for abnormal cytology and/or positive hrHPV infection. A possible limitation is that our results are insufficient to investigate the sensitivity or specificity of Pap smear and/or HPV genotypes. This is due to different biopsy indications across centers and clinicians. This study includes not only cases which Pap smear and HPV test conducted at the same time, but also cases with abnormal cervical cytology followed by HPV testing. In addition, there was no central review of cervical biopsy histology specimens.
Most women underwent additional procedures such as repeated cytology or colposcopy unnecessarily. Therefore, establishing an accurate indication of colposcopy is important for the management of patients with abnormal cytology. Age and HPV 16/18 were responsible for the majority of discrepancies between cytology and histology results, and should be considered in cervical cancer screening. We recommend further research to assess efficient cervical cancer screening especially with abnormal cytology.
 XML Download
XML Download