

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Around 1830, Jean Cruveilhier, a French anatomist and pathologist, described necrosis of the femoral head as a late complication of hip trauma. He presumed vascular injury was the etiology of the necrosis.1 In early and middle 20th century, various non-traumatic factors were identified to induce the disease or to involve in its development.23 This disease entity had been called as avascular necrosis, ischemic necrosis or aseptic necrosis of the femoral head. In 1992, the Committee on Nomenclature and Staging of the Association Research Circulation Osseous (ARCO) agreed to use ‘osteonecrosis’ as a uniform terminology for necrotic lesions of the femoral head.
Non-traumatic osteonecrosis of the femoral head (ONFH) usually affects adults younger than 50 years. In the United States, more than 10,000 new patients are affected with the disease every year, and it accounts for up to 10% of total hip arthroplasties (THAs).4 In South Korea, the annual incidence of ONFH increased from 9,870 in 2002 to 18,691 in 2006.5 The annual incidence rate in Japan was 1.91/100,000 and the annual incidence was estimated to be more than 2,400 in the survey from 2010 to 2013.6 In China, the cumulative number of ONFH patients reached 8.12 million in 2013.7
In this review, we provide up-to-date knowledge on the etiology, pathogenesis, classification criteria, staging system, and treatment of non-traumatic ONFH.
Go to : 
ETIOLOGY
In 1913, osteonecrotic lesions were found in divers and this disease entity was known as “Caisson disease” and later as dysbaric osteonecrosis.8 Osteonecrosis in patients with sickle cell disease was recognized in the 1960s.9 As Chandler called the disease “coronary arterial disease of the hip”,10 embolism seemed to play the central role in the development of ONFH in patients with hemoglobinopathies and those with dysbaric osteonecrosis.
In 1962, the first case of ONFH after the use of corticosteroid was reported.11 By the 1970s, it was known that excessive-alcohol consumers had increased incidence of ONFH.12
During last three decades, thrombophilia, hypofibrinolysis, and hypoangiogenesis were found to involve in the pathogenesis of ONFH,1516 and familial ONFHs were reported.1516
The pathogenesis of non-traumatic ONFH is perplexing, and it remains to be investigated and scrutinized. Nevertheless, there are three general agreements. First, local ischemia due to compromised blood flow is the final common pathway in the pathogenesis of ONFHs other than radiation induced osteonecrosis. Second, alcohol- or steroid-associated ONFH is not an embolic infarction. It is a kind of intraosseous compartment syndrome. Third, the disease has a multifactorial etiology including genetic predispositions and exposure to risk factors. In most ONFH patients, both of genetic and non-genetic risk factors reciprocally interact and play roles together in the pathogenesis.171819 The genetic predisposition explains why only some of steroid users and alcohol abusers acquire the disease, while others do not.
Genetic factors are implicated in hypercoagulability/hypofibrinolysis and/or hypoangiogenesis. Protein C and protein S deficiencies,1620212223 mutations in the factor V Leiden or the prothrombin 20210A gene,20 polymorphisms of the plasminogen activator inhibitor-1 gene,212425 and presence of antiphospholipid antibodies2627 and decreased activity of 5,10-methylenetetrahydrofolate reductase25 have been known to be associated with hypercoagulability. Polymorphism of the endothelial nitric oxide synthase gene and vascular endothelial growth factor have been known to impair angiogenesis and to be associated with ONFH.28293031
Corticosteroid use and alcohol overuse are well known risk factors for ONFH. Besides, smoking, systemic lupus erythematosus, dysbaric disorders, pelvic radiation therapy, non-steroidal chemotherapeutic agents for leukemia and other myelogenous diseases, sickle cell disease, Gaucher's disease, human immunodeficiency virus infection, and pancreatitis have been known as risk factors or associated conditions of ONFH.323334353637383940414243444546474849
Even though corticosteroids and alcohol are leading causes of ONFH, there have been no unified criteria to classify corticosteroid-associated ONFH and alcohol-associated ONFH. In 2017, ARCO develop a classification scheme of corticosteroid-associated and alcohol-associated ONFH to standardize clinical studies on ONFH through Delphi surveys. The ARCO classification criteria of corticosteroid-associated ONFH included the following: 1) patients should have a history of corticosteroid use > 2 g of prednisolone or its equivalent within a 3-month period; 2) osteonecrosis should be diagnosed within 2 years after corticosteroid usage, and 3) patients should not have other risk factor(s) besides corticosteroids.50 The criteria of alcohol-associated ONFH included the following: 1) patients should have a history of alcohol intake > 400 mL/week (320 g/week, any type of alcoholic beverage) of pure ethanol for more than 6 months; 2) ONFH should be diagnosed within 1 year after alcohol intake of this dose; and 3) patients should not have other risk factor(s) than alcohol abuse.51
ARCO recommends using these criteria for studies about ONFH.
Go to :
PATHOGENESIS
Embolism plays the central role in vascular occlusion and consequent ONFH in hemoglobinopathies and dysbaric disorders.373846
However, alcohol- and corticosteroid-associated ONFHs are not embolic infarctions and have different mechanisms in the pathogenesis. In 2019, ARCO task force developed a plausible model to explain the pathogenetic of non-traumatic ONFH.52
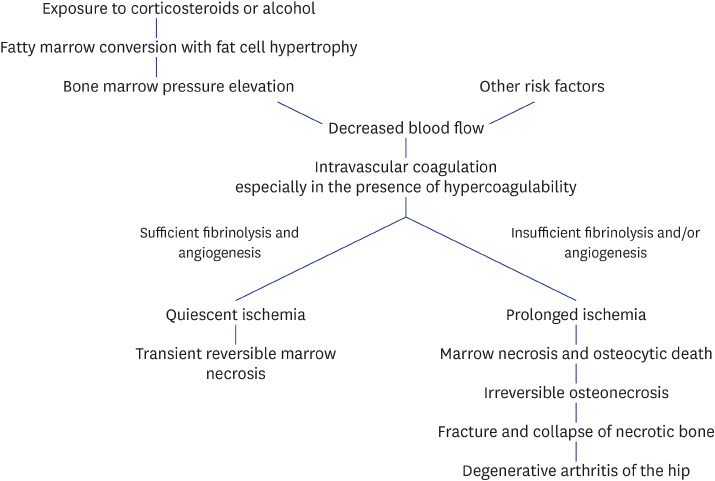
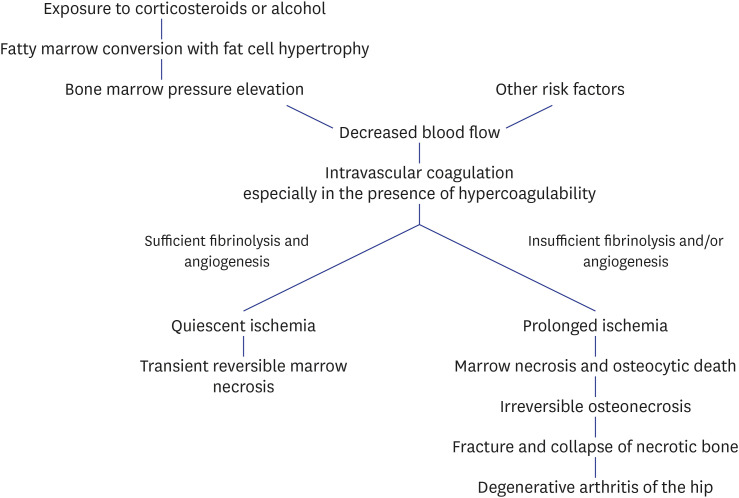
Corticosteroids and alcohol promote differentiation of mesenchymal stem cells to adipocytes. They also induce hypertrophy of the adipocyte through increasing intracellular lipid synthesis.535455565758 The increments of number and volume of marrow fat cell induce intra-osseous hypertension in the proximal femur. Venous sinusoids are compressed due to the intra-osseous hypertension, and intravascular coagulation occurs. Then, arterial blood flow is blocked, and an ischemia occurs in the femoral head.659606162
Corticosteroid- and alcohol-associated ONFHs are kinds of intra-osseous compartment syndrome inside the femoral head due to an ischemic cascade: 1) hyperplasia of marrow fat cell; 2) intra-osseous hypertension; 3) vascular compression and intravascular coagulation; 4) impaired blood flow; 5) marrow necrosis and osteocytic death; and 6) fibrovascular reparative process around the necrotic zone and saponification of necrotic marrow.176364
Once, this reparative zone is formed, the lesion is irreversible. Thus, the presence of encapsulating fibrovascular reparative tissue around the necrotic bone is the histologic criteria to make a definite diagnosis of ONFH.636465
The necrotic bone becomes saponified and mechanically weak. Thus, stress fracture occurs in the necrotic bone, followed by collapse of the femoral head and subsequent arthritis of the hip.506667
Ischemic lesions do not always progress to irreversible osteonecrosis. Whether the ischemic lesion progresses to osteonecrosis or not depends on the degree of restoration of vascular perfusion and the creeping substitution of dead bone by new bone.63676869 Genetic predispositions of hypercoagulability/hypo-fibrinolysis and/or hypo-angiogenesis play role in the restoration of vascular perfusion (Fig. 1).1620212223
Go to :
STAGING
The first ARCO staging system of ONFH was established in 1994. In 2019, ARCO revised the staging system. In the first version, marrow necrosis was defined as stage 0 (marrow necrosis without reparative process, no low-signal band on magnetic resonance imaging [MRI]). In the revised system, stage 0 (marrow necrosis without reparative process, no low-signal band on MRI) was deleted, stage III was divided into early (IIIA) and late stage (IIIB) according to the depth (2 mm) of head depression, and subclassification of location/size was not incorporated (Table 1).64

Table 1
The 2019 revised ARCO staging for osteonecrosis of the femoral head
ARCO = Association Research Circulation Osseous, MRI = magnetic resonance imaging, CT = computed tomography.
![]()
Go to :
SIZE/LOCATION OF NECROTIC PORTION AND NATURAL COURSE
The size/location of necrosis predicts further collapse of the femoral head and is the major determinant in the treatment of ONFH. Various classification systems have been developed to characterize the size/location of necrosis. Currently, three classification systems: Steinberg classification, Japanese Investigation Committee (JIC) classification and modified Kerboul classification, are widely used.
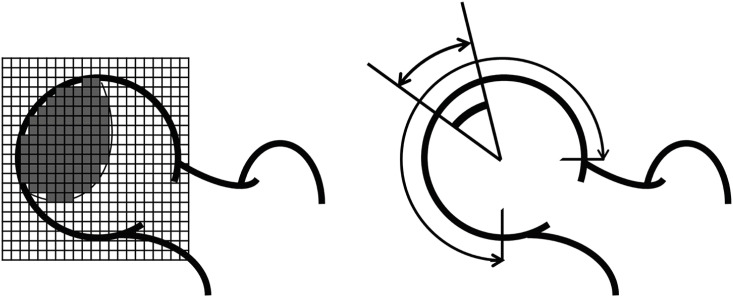
The Steinberg system categorized the extent of involvement into 3 subsets: mild (< 15% of articular surface or head affected), moderate (15–30%), and severe (> 30%) (Fig. 2).70
The JIC classification is based on the mid-coronal T1-weighted magnetic resonance (MR) image of the femoral head. In the JIC classification, necrotic lesions were classified into four types: type A lesion < medial 1/3 of the weight-bearing portion; type B lesion < medial 2/3 of the weight-bearing portion; type C1 lesion > medial 2/3 of the weight-bearing portion but not extending laterally to the acetabular edge; and type C2 lesion extending laterally to the acetabular edge. The prevalence of collapse was < 10% in type A, 40% in type B, 80% in type C1, and > 90% in type C2 (Fig. 3).7172
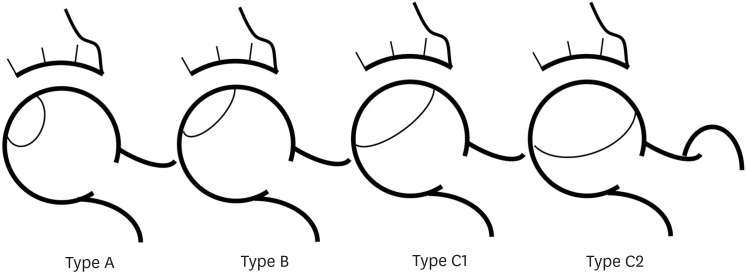 | Fig. 3Japanese Investigation Committee classification system of femoral head osteonecrosis. Four types: type A lesion < medial 1/3 of the weight-bearing portion; type B lesion < medial 2/3 of the weight-bearing portion; type C1 lesion > medial 2/3 of the weight-bearing portion but not extending laterally to the acetabular edge; and type C2 lesion extending laterally to the acetabular edge.
|
In 1974, Kerboul et al.73 developed a method to quantify the extent of necrosis by measuring the arc of the necrotic portion on anteroposterior and lateral radiographs and then calculating the sum of these two angles. In 2006, Ha et al.74 modified the method by measuring the necrotic arc on the midcoronal and midsagittal MR images (Fig. 4). The authors classified the necrotic lesions into 3 categories: small lesion (combined necrotic angle < 190°), medium-sized lesion (combined necrotic angle between 190° and 240°), and large lesion (combined necrotic angle > 240°). There was a strong correlation between the combined necrotic angle and the risk of femoral head collapse. None of small lesions collapsed, all large lesions collapsed, while 50% of medium-sized lesions collapsed within 3 years from the diagnosis of ONFH.74
 | Fig. 4Modified Kerboul classification system of femoral head osteonecrosis. A: necrotic angle in mid-coronal MR image. B: necrotic angle in mid-sagittal MR image. Combined necrotic angle: A + B. Three categories: small lesion (combined necrotic angle ≤ 190°), medium-sized lesion (combined necrotic angle between 190° and 240°), and large lesion (combined necrotic angle ≥ 240°).MR = magnetic resonance.
|
There is no agreement as to which method is most reliable and valid. Unified classification system of necrotic size/location should be developed.
Go to :
TREATMENTS
The risk of collapse depends on the size/location of the necrotic portion. Small lesions seldom develop collapse even without any medical or surgical treatment, while most of large lesions are progressive.757677 The extent of necrotic portion is determined at the ischemic attack. Once ONFH develops, the lesion does not increase in size regardless of the disease progression in the stage.78 Thus, the size of necrotic portion should be evaluated prior to treating ONFH, and any treatment should not be done in small lesions. The efficacy of certain treatment should be determined cautiously considering the different natural courses according to the size of necrosis.
Medical treatments
To date, various pharmacological agents including enoxaparin, statins, bisphosphonates, iloprost and acetylsalicylic acid have been tried to retard or reverse the disease progression.7980818283848586878889909192939495
However, none of them have been proven to be effective by high level evidence, and most of them have adverse reactions.96
At this moment, no pharmacological prevention or treatment is recommendable.
Core decompression (CD) with bone marrow aspirate concentration (BMAC)
CD has been used in early-stage (pre-collapse) ONFH with the assumption that it prevents femoral head collapse and hopefully reverses the disease progression. However, the results of CD were not consistent, and the effectiveness of CD was questioned.97
Recently, injection of BMAC was combined to traditional CD to improve the results. While earlier studies have supported the effectiveness of additional cell therapy,9899100101102103 later studies reported no differences in outcomes between CD with BMAC and CD alone. Both of CD and BMAC therapy had high rates of progression in large lesions.104105106 Whether BMAC is effective or not is a controversial issue, which needs further investigation.
Osteotomies
Various osteotomies of the proximal femur were introduced to preserve osteonecrotic hips. These procedures move the necrotic portion from the weight-bearing dome to a non-weight-bearing region. Among them, transtrochanteric curved varus osteotomy (TCVO)107 and transtrochanteric rotational osteotomy (TRO)108 have been done mainly in Japan and South Korea.
In 2017, Lee et al.109 compared the results of 91 TROs and 65 TCVOs. In their comparison, TCVO was better than TRO in terms of operation time, the amount of blood, postoperative collapse, osteoarthritic change (20% vs. 37.4%), and THA conversion rate (10.8% vs. 16.5%). Thus, they recommended TCVO rather than TRO.
Vascularized bone grafts
Vascularized fibular grafting was first described by Judet et al.110 in 1980 and subsequently popularized by Urbaniak et al.111 and Yoo et al.112 Vascularized iliac bone grafting including a pedicle of the iliac circumflex artery has been favored because the iliac bone is in vicinity of the femoral head and the process needs no microsurgical anastomosis.113 However, vascularized bone grafts have been criticized for the technical difficulties and donor site morbidities. Currently, these procedures are only performed at several centers throughout the world.
Resurfacing arthroplasty
Hemi-resurfacing and total resurfacing arthroplasties were once considered as bone sparing alternatives to THA in young ONFH patients.114115 However, hemi-resurfacing has been abandoned and total resurfacing is rarely done due to complication related with the metal-on-metal bearing and risk of periprosthetic femoral neck fracture.116
THA using highly cross-linked polyethylene liners
Excessive wear rates and subsequent osteolysis associated with conventional polyethylene have prompted more durable bearings in young patients.117
Highly cross-linked polyethylene, which has enhanced wear-resistant properties, has rapidly replaced conventional polyethylene. Ionizing radiation during the manufacturing process increases the number of crosslinks and thereby reduces the polyethylene wear. Current cross-linking techniques use gamma-rays in place of electron beam irradiation and subsequent annealing or remelting of the polyethylene.118
Highly cross-linked polyethylene liners can be coupled with either cobalt chromium or ceramic femoral head. There are short-term follow-up studies to suggest that the clinical and radiological results of the highly cross-linked polyethylene liners are promising in patients with ONFH.119120 However, the long-term results remain unknown. There is a concern over the risk of fracture in these liners with time. To prevent fracture, a minimum liner thickness > 6 mm has been advocated.121
THA using ceramic-on-ceramic (CoC) bearings
Go to :
SUMMARY
ONFH has a multifactorial etiology including genetic predispositions and exposure to risk factors. The size/location of necrosis is the predictor for collapse of the femoral head and should be the major determinant in the treatment of ONFH patients. The extent of necrosis is determined at the initial ischemic attack, and the size of the lesion does not change with time. Small lesions do not progress even without any intervention and need no treatment. Any treatment, medical or surgical, should be done in medium-sized to large lesions with pain. To date, no pharmacological prevention or treatment has been proven to be effective and is not recommendable. CD combined with BMAC therapy does not work in large lesions and needs further investigations to verify its effectiveness. Osteotomy should be done cautiously in selected patients. Resurfacing arthroplasties are not recommendable in ONFH patients. THA using highly cross-linked polyethylene liners or CoC bearings showed excellent outcomes at early to medium term follow-up studies. However, the long-term follow-up results are unrevealed, yet.
Go to :
 XML Download
XML Download