

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Since coronavirus disease 2019 (COVID-19) was first described in December 2019 in China, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the virus responsible for COVID-19, has spread throughout the world. There have been numerous reports of COVID-19 in healthcare workers (HCWs) and hospitalized patients in several countries globally.123 Although it is probable that hospital-acquired infections are also key factors in COVID-19 transmission, the contribution of nosocomial transmission to the spread of COVID-19 is currently unclear.
At present, South Korea is experiencing its third wave of COVID-19, which began mid-November 2020. Recently, we experienced a COVID-19 outbreak at Chonnam National University Hospital (CNUH) in Gwangju, South Korea, following the diagnosis of a HCW with COVID-19 on 11/13/2021. In this study, we report our experience in managing the in hospital COVID-19 outbreak. As a result of our study, we have changed our infection control strategies for preventing nosocomial transmission to correspond with community prevalence.
METHODS
Hospital overview
CNUH is a major acute teaching hospital with over 1,000 beds and a 24 h accident and emergency service, serving over 3.5 million people in the Chonnam province and Gwangju metropolitan city. CNUH is composed of seven buildings (buildings 1, 2, 3, 5, 6, 7 and 8) (Supplementary Fig. 1A). Building 1 was constructed in 1979 and building 8 was constructed in 2001. Buildings 1 and 8 each have twelve floors. Building 7 is next to building 8, and the two buildings are connected on floors 1, 2 and 7. Buildings 1 and 7 are linked on floor 2 by a sky bridge. The general ward of building 1 comprises two wings (A and B), a communal toilet, and a communal bathroom. In addition, there is one single-patient room, five two-patient rooms, and five six-patient rooms in each wing (Supplementary Fig. 1B). There are toilet facilities in each single or two-patient room in the ward.
Hospital COVID-19 prevention measures before the healthcare-associated outbreak
All visitors and patients filled out a questionnaire regarding travel and contact history and underwent thermal scanning for fever before entry into the hospital premises was permitted. All patients with scheduled operations were only admitted following presentation of a negative SARS-CoV-2 reverse transcription-polymerase chain reaction (RT-PCR) test within 48 hours of admission.4 Each outpatient was only allowed 1−2 accompanying person(s) when attending the specialist outpatient clinic. Each inpatient was restricted to only one attending caregiver throughout the period of hospitalization, except near the time of death; however, caregivers could be changed without restrictions. Patients with fever (> 37.5°C) or respiratory symptoms were transferred to the triage room in the emergency area or outpatient clinic for SARS-CoV-2 RT-PCR testing. Medical staff in the triage room wore personal protective equipment (PPE) including gowns, gloves, N95 respirator and face shields or goggles. Everyone in the hospital was encouraged to wear masks and follow hand hygiene practices. Our administrative office recommended to avoid large events and gatherings, but it was not mandatory.
Test systems and contact tracing after the first confirmed COVID-19 HCW case in the hospital
The first confirmed COVID-19 case was a 30-year-old second-grade neurosurgery resident. On 11/13/2020, the patient visited the triage room presenting with cough and myalgia. The patient had no history of travel or close contact with confirmed COVID-19 cases. Following confirmation of COVID-19 infection on the evening of 13/11/2020, our infection control team announced the closure of the emergency room (ER) of the hospital; the ER and neurosurgical intensive care unit (NCU) were the main workplaces of the neurosurgery resident diagnosed with COVID-19. We then conducted contact tracing and tested HCWs, patients and caregivers in all areas served by neurosurgeons (ER, NCU, general neurosurgery wards [6A and 6B]) for COVID-19.
RT-PCR was performed using combined nasopharyngeal and oropharyngeal swabs in the CNUH laboratory, a diagnostic facility for COVID-19 authorized by the Korean Center for Disease Control and Prevention (KCDC). RNA was extracted using an automated nucleic acid extraction system (AdvanSure™ E3 System; LG Chem, Korea). Extracted RNA was amplified using a commercial kit (PowerChek™ 2019-nCoV Real-time PCR Kit; Kogenebiotech, Korea) and the envelope (E) and RNA-dependent RNA polymerase (RdRP) genes were detected (CFX96™ Real-time PCR detection system; Bio-Rad, USA). A positive RT-PCR result was defined as both E and RdRP genes had Ct values of 35 or less, whereas a Ct values over 40 was considered negative; a Ct values of 35−40 was considered indeterminate. In total, 439 respiratory samples from 344 HCWs, 47 patients and 48 caregivers were obtained between 11/13/2020 and 11/14/2020.
Close contacts of suspected/confirmed COVID-19 cases, as defined according to the World Health Organization guidelines,5 were tested for COVID-19. Close contacts with negative test results were obliged to self-quarantine for 14 days following their most recent contact with a confirmed COVID-19 patient, then retested at the end of the quarantine period. In cases of contact but not close contact, self-quarantine was not enforced, but active and passive monitoring were implemented. During active monitoring, the local public health authority assumed responsibility to establish regular communication with exposed people to assess for symptoms. Passive monitoring required exposed people to self-monitor by performing regular temperature checks.
RESULTS
Outbreak in the department of neurosurgery
Following confirmation of COVID-19 in the second-grade neurosurgery resident, we traced contacts made with the COVID-19 case from 11/09/2020 to 11/13/2020; we found a symptomatic third-grade neurosurgery resident and discovered that 13 neurosurgeons had attended a get-together (‘hoesik’ in Korean) for 6 hours with the first COVID-19−confirmed HCW on 11/12/2020. Fig. 1A shows the estimated transmission routes of 22 cases of COVID-19 in the neurosurgery outbreak. Through contact tracing and testing, we diagnosed COVID-19 in two other neurosurgery residents (Fig. 1A, Case numbers 2 and 3) and a nurse (Fig. 1A, Case number 4) of ward 6A of building 1 on 11/14/2020. We quarantined all neurosurgery doctors and nurses, healthcare assistants, and cleaners of NCU and neurosurgery wards (6A, 6B) from 11/14/2020 to 11/27/2020. The ER remained closed throughout this period because we were unable to respond to emergency neurosurgery calls due to the possibility of COVID-19 in HCWs. We recommended patients to be discharged from the hospital and quarantine at home for 14 days, and the remaining inpatients and caregivers were quarantined for 14 days within the hospital. We performed RT-PCR follow-up tests every 3 days for the remaining NCU patients, and semi-weekly RT-PCR follow-up tests for the remaining patients/caregivers in the general wards during the 14 days following last exposure. The patients and caregivers who were discharged from the neurosurgery areas between 11/09/2020 and 11/13/2020 were invited by call to undergo RT-PCR testing. From our surveillance, we found that three patients/caregivers discharged from ward 6A and two patients/caregivers discharged from ward 6B were infected with SARS-CoV-2. Of the follow-up RT-PCR tests, one patient in the NCU (Fig. 1A, Case number 10) was diagnosed with COVID-19 on 11/17/2020. Unexpectedly, a nurse based in the intervention room (Case number 11) who had performed several neurovascular interventions was diagnosed with symptomatic COVID-19 on 11/18/2020. During the quarantine period of the neurosurgery-based HCWs, three symptomatic and seven asymptomatic HCWs were diagnosed with COVID-19.
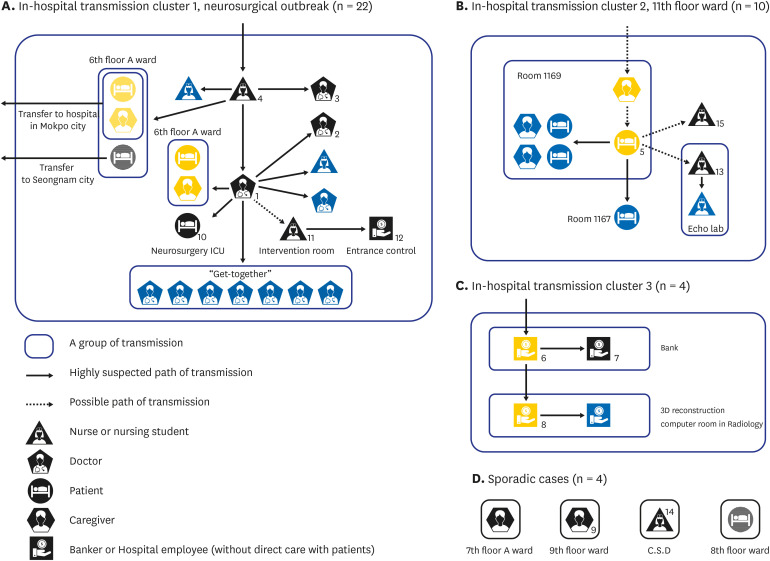
Fig. 1
Estimated transmission routes of COVID-19 cases who were diagnosed within CNUH or were epidemiologically associated with CNUH. (A) The in-hospital transmission during the neurosurgery (NS) department outbreak. Discharged patients and a caregiver from NS ward were transferred to other hospitals in Mokpo city and Seongnam city. (B) Intra-hospital transmission involving 10 COVID-19 patients. (C) Related COVID-19 cases in a private company (KJ bank). (D) Sporadic cases. The numbering of the COVID-19 case symbols represents the order in which the cases were diagnosed in the laboratory of CNUH during the complete enumeration survey. Blue coloring indicates COVID-19 cases that were diagnosed during the self-isolation period and yellow coloring indicates family members within a transmission group. Symbols with a grid pattern represent COVID-19 cases that caused community transmission after discharge.
C.S.D = central supply department, COVID-19 = coronavirus disease 2019, CNUH = Chonnam National University Hospital.
![]()
Epidemiological evaluation of Gwangju city revealed that the neurosurgery outbreak originated from the community outbreak spot of the Gwangju city.
First complete enumeration survey of all hospital employees and all patients/caregivers
COVID-19 was confirmed in a total of four HCWs (three neurosurgery residents and one nurse, Case numbers 1−4 of Fig. 1A) by 11/14/2020. Our rapid response team was gathered in the morning of 11/15/2020, and their roles were activated according to our hospital's public health crisis situations manual (Table 1). Following this, we expanded RT-PCR testing to all hospital employees, including outsourced agencies and all hospitalized patients and their caregivers, to find asymptomatic COVID-19 patients. The first complete enumeration test (CET) was conducted from 11/13/2020 to 11/17/2020, during which a total of 730 patients, 498 caregivers, and 3,346 hospital staffs, employees and business company employees had been subjected to COVID-19 testing by RT-PCR. Table 2 shows the number of SARS-CoV-2 RT-PCR tests performed according to the professions of HCWs.
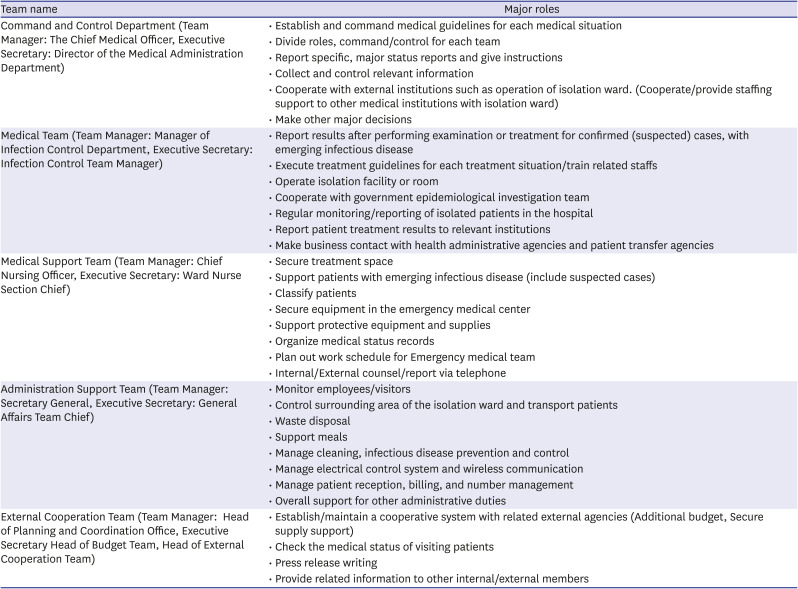

Table 1
Role of rapid response team for public health crisis situations
![]()
Table 2
The number of healthcare workers who underwent SARS-CoV-2 RT-PCR testing from 11/13/2020 to 12/04/2020 in Chonnam National University Hospital after the first confirmed case of COVID-19
A person may undergo multiple SARS-CoV-2 RT-PCR tests in one CET cycle if COVID-19 symptoms are present.
SARS-VoV-2 = severe acute respiratory syndrome coronavirus 2, RT-PCR = reverse transcription-polymerase chain reaction, COVID-19 = coronavirus disease 2019, CET = complete enumeration test.
![]()
During the first CET, we found five additional asymptomatic COVID-19 cases, including a patient (Fig. 1B, Case number 5) on Floor 11 of building 1; two bankers who worked in Kwangju bank (Case numbers 6 and 7 of Fig. 1C) on floor 1; a radiologist (Case number 8, husband of Case number 6) on floor 2 of Building 1; and a caregiver on floor 9 of building 1 (Case number 9 of Fig. 1D). The overall COVID-19 positivity rate of the first CET (100 × positive tests/total number of tests conducted, 9/4,496) was 0.2%. We were later informed by a community health center on 11/16/2020 about one asymptomatic COVID-19 case (caregiver of a patient from floor 7A who was discharged on 11/14/2020 after 3 days' admission), and one symptomatic COVID-19 case (patient from floor 8 discharged on 11/13/2020 after 4 days' admission). Fig. 2 shows a schematic diagram of COVID-19 occurrence sites in CNUH. The majority of COVID-19 cases were from within building 1, and the cases in building 8 were epidemiologically related to the COVID-19 cases of building 1.
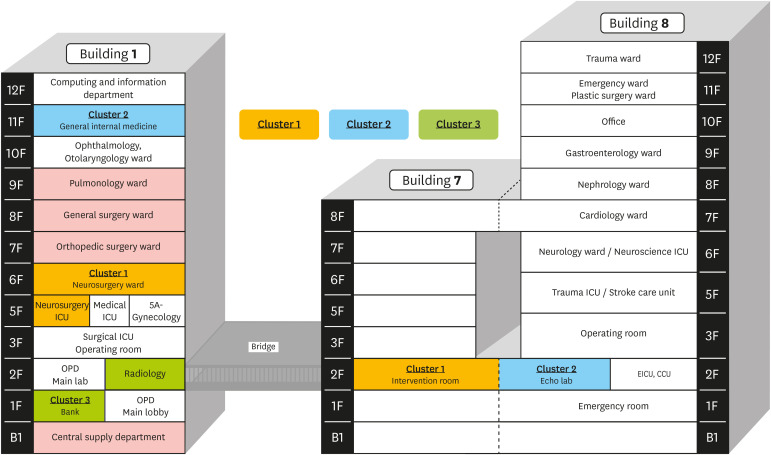
Fig. 2
Floor plan of Chonnam National University Hospital and the sites of coronavirus disease 2019 occurrences. The areas of each cluster of intra-hospital transmission are colored similarly. Green areas represent the predicted sites of sporadic cases originating from outside the hospital.
ICU = intensive care unit, EICU = emergency intensive care unit, CCU = coronary care unit, OPD = outpatient department.
![]()
Outbreak resolutions
Quarantine of floors 5−11 of building 1
We did not find any epidemiological relationship between the neurosurgery outbreak and the seven COVID-19 cases discovered during the first CET. Therefore, we decided to quarantine building 1 on 11/17/2020 to prevent a larger healthcare-associated outbreak and to investigate potential epidemiological linkages. We assessed the COVID-19 risk for each ward, and classified the wards as high-risk (NCU, 6F, 7F, 8F. 9F, 11F) and low-risk (5A, 10F). For floors 5−11 of building 1, inpatients who had not had contact with confirmed COVID-19 patients were discharged or transferred to other hospitals, while inpatients and caregivers who had contact history with confirmed COVID-19 patients were quarantined in single rooms, cohort rooms or at home for 14 days after discharge. A total of 107 patients and 60 caregivers were isolated in the hospital. All employees in cohort wards used gowns, gloves, medical masks, and eye protection when providing care to patients in building 1. Tables 3 and 4 show the cohort management guidelines of buildings 1 and 8, created by the CNUH infection control unit. Building 1 was closed to new admissions for 14 days. Outpatient clinics were also temporarily closed from 11/16/2020.
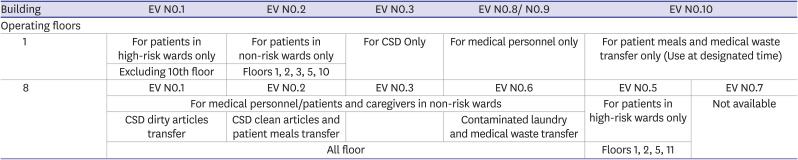
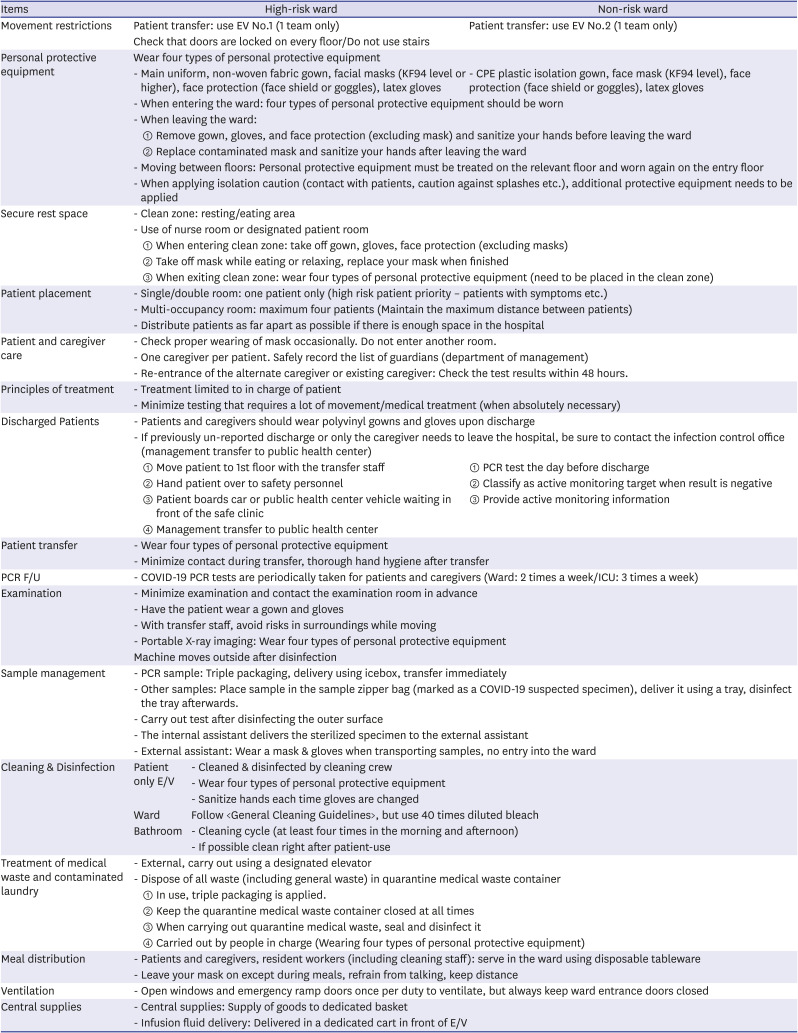
Table 3
Isolation (Building 1 Cohort) management guideline (1)
![]()
Table 4
Isolation (Building 1 Cohort) management guideline (2)
![]()
Surveillance of people with contact histories with confirmed COVID-19 patients
The CNUH infection control team reviewed electronic medical charts, closed circuit television, and personal movements with the goal of identifying individuals who had had contact with confirmed COVID-19 patients; this was performed for each positive SARS-CoV-2 RT-PCR test. We predefined the range of exposure and patient close contacts. Although we attempted to trace contacts thoroughly, full tracing was not possible.
Of the cohort, 322 HCWs were quarantined, 279 HCWs were placed under active monitoring, and 29 HCWs were placed under passive monitoring (Table 5). Following incomplete contact tracing, emergency alert messages were sent to citizens through the Cell Broadcast System, encouraging people who had been in the CNUH area between 11/09/2020 and 11/17/2020 to visit screening centers voluntarily for testing.
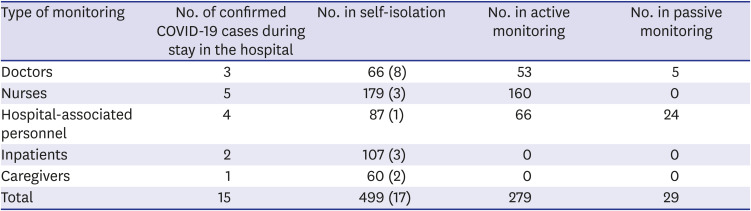
Table 5
Number of self-quarantine cases, active monitoring cases and confirmed cases from 11/13/2020 to 12/05/2020
The numbers in parentheses represents the number of people who were confirmed COVID-19 during self-isolation period. There were no confirmed cases during active or passive monitoring status.
COVID-19 = coronavirus disease 2019.
![]()
Five-day cycles of CET
Following the detection of COVID-19 in CNUH, the community onset of COVID-19 patients increased simultaneously. We performed periodic testing (every 5 days) for the entire HCW population. Fig. 3 shows a timeline of healthcare-associated COVID-19 infections and the number of SARS-CoV-2 RT-PCR tests performed. During the second CET, we detected one symptomatic (Case number 13 in Fig. 3) and one asymptomatic (Case number 14 in Fig. 3) COVID-19 case, each without obvious epidemiological ties with previously confirmed COVID-19 cases in the hospital. During the third CET, one symptomatic HCW was diagnosed with COVID-19 (Case number 15 in Fig. 3); the HCW was a nurse who had worked on floor 11 until 11/13/2020. COVID-19 case numbers 13 and 15 were not under active or passive monitoring at the time of diagnosis.
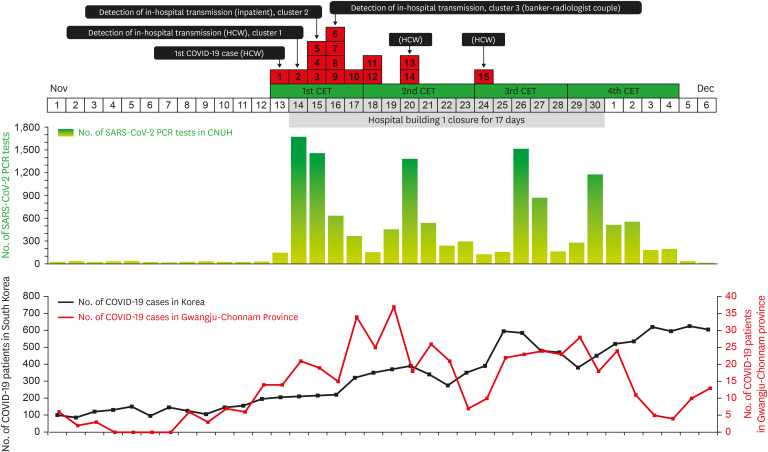
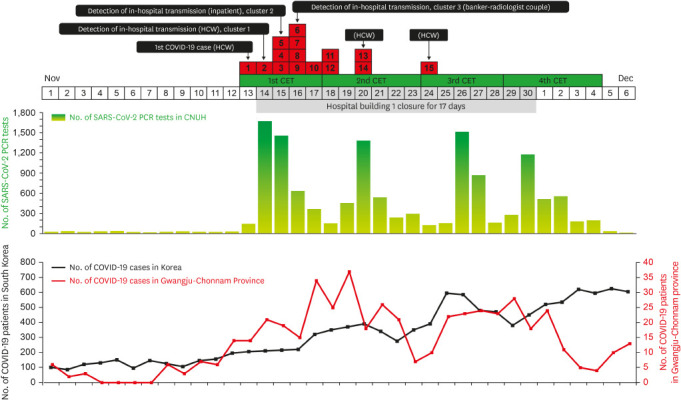
Fig. 3
Timeline of the COVID-19 outbreak in CNUH. The red boxes indicate each COVID-19 case diagnosed in the CNUH laboratory. Layered red boxes represent the number of COVID-19 patients diagnosed per day. Numbers in the red boxes represent the temporal order of diagnoses in CNUH and correspond to the numbered cases in Fig. 1. Green graph (top) represents the number of SARS-CoV-2 PCR tests performed per day. Red and black graphs (bottom) represent the number of COVID-19 cases in South Korea and the surrounding community.
CET = complete enumeration test, HCW = healthcare worker, COVID-19 = coronavirus disease 2019, CNUH = Chonnam National University Hospital, SARS-VoV-2 = severe acute respiratory syndrome coronavirus 2, PCR = polymerase chain reaction.
![]()
Outbreak analysis
After performing four CET cycles in CNUH, and testing people outside of CNUH following calls or emergency message alerts, we discovered a total of 40 COVID-19 cases with suspicious links to CNUH, including the 22 cases detected during the neurosurgery outbreak. The second large cluster (cluster 2) of COVID-19 cases was linked to a patient on floor 11 (Fig. 1B, Case number 5). The initial SARS-CoV-2 RT-PCR test for Case number 5 was performed in the ER on 11/05/2020 and the result was negative; however, the same patient tested positive on 11/14/2020. Case number 5 had a 2D-echocardiograph on 11/12/2020. There were ten COVID-19 cases in cluster 2. Cluster 3 included a banker and a radiologist who were a husband-and-wife couple; the parents and children of the wife (banker) had tested positive for SARS-CoV-2 following RT-PCR testing. Case number 9 from floor 9 cared for her mother for 3 months, but the mother tested negative for SARS-CoV-2. In four cases of sporadic COVID-19 (Fig. 1D), there was no evidence of secondary transmission in the hospital.
During the quarantine period, the hospital quality improvement team ensured mask wearing compliance by all visitors and HCWs. Following the CNUH quarantine, our infection control policy was amended. Universal screening of all inpatients and resident caregivers was mandatory upon admission. A negative SARS-CoV-2 RT-PCR test within 48 h of admission was required. Whenever a caregiver changes, a negative SARS-CoV-2 RT-PCR test result was required.
Outpatient clinics re-opened on 11/18/2020 and the ER re-opened on 11/27/2020. On 12/01/2020, building 1 re-opened after 17 days' quarantine. Total patients admitted were 922 on 11/12/2020 before the first confirmed COVID-19 cases. The lowest number of admitted patients was 248 on 11/28/2020, and the total number of patients admitted on 12/07/2020 after the quarantine was 540. The official total of COVID-19 cases associated with the CNUH, including n order transmission, was 67.
Change of infection control practices after outbreak
Universal screening of all inpatients and resident caregivers is now mandatory upon admission and on day 4 of hospitalization, and HCWs are tested monthly. For HCW and patients with potential exposure to patients with COVID-19, additional RT-PCR testing every 3 days for active monitoring and PCR every 5 days for passive monitoring are mandatory. Ventilation is an important factor in preventing the virus that causes COVID-19 from spreading. We identified areas that are not well ventilated and set split air conditioning units, fan coils or any system that runs with a recirculation mode not to recirculate. In cases where the recirculation of air is unavoidable, we increased outdoor air exchange by opening windows.
We recommended keeping windows in patient rooms open and opening emergency ramp doors once per duty, but always keeping the patient doors and the curtains between beds in the multi-occupancy room closed. An audit team including infection control team, quality improvement team, and nursing staff measured the performance rate of the guidelines (hand washing, mask, ventilation, etc.) regularly.
DISCUSSION
Throughout the current COVID-19 pandemic, preventing nosocomial COVID-19 outbreaks has been a major challenge for hospitals. In this study, we found that three classes of COVID-19 cases posed the greatest risk as sources of transmission in healthcare settings: SARS-CoV-2 positive HCWs who were not yet aware of their infection, SARS-CoV-2 positive caregivers before diagnosis and SARS-CoV-2 positive patients before diagnosis. Through epidemiologic evaluation, we found that during the neurosurgery COVID-19 outbreak (cluster 1), the initial source of COVID-19 was inflow from outside the hospital from a HCW, which consequently triggered intra- and inter-hospital COVID-19 spread. This highlights the important role of HCWs in the introduction of COVID-19 from the community into enclosed hospital settings. The number of asymptomatic cases of COVID-19 is high in young people.6 Young people, including acting nurses and residents, comprise the majority of the hospital workforce, and are more likely to work in multiple places throughout hospitals as well as to be socially active. Younger patients may not be screened and diagnosed with COVID-19 due to their lack of symptoms. Our experience highlights the need for repeated mass screening of all HCWs to help reduce HCW-associated transmission in acute-care teaching hospitals, although there are debates regarding mass testing for asymptomatic HCWs to reduce nosocomial transmission.789
By implementing the CET survey, we found an additional two infection clusters and four sporadic cases. In epidemiological investigation, we predicted that case number 14 might have been the last spreader in hospital transmission. Therefore, the CET period was decided to end two weeks after case number 14 was confirmed positive (Dec 04, 2020). We set CET interval as every 5 days because we conduct PCR every 5 days for passive monitoring. The early detection of COVID-19 cases in the hospital was likely to have reduced community spread. We found evidence for intra-hospital transmission in cluster 2, and that the caregivers played an important role in nosocomial COVID-19 transmission. Identifying the source of infection for HCWs and caregivers is more difficult, as they migrate between the hospital and the community on a daily basis. Therefore, universal screening upon admission of all inpatients and resident caregivers may be an effective strategy to prevent outbreaks in tertiary care hospitals with high influxes of patients, especially when the prevalence of COVID-19 is increasing within the community. Our results suggest that a testing strategy should be adapted based on the prevalence of the disease within the population as predicted by epidemiological surveillance, with testing for symptomatic individuals at times of low prevalence, then implementing rapid expansion of testing to include asymptomatic HCWs during new infection wave.
The infection control policy for COVID-19, which includes the use of masks and frequent use of alcohol-based hand sanitizers, is currently being implemented in all South Korean hospitals. Combining facial masks and social distancing is effective at controlling COVID-19.10 However, the extent of hand hygiene compliance among HCWs varies widely, ranging from 20% to 80%.1011 Mask wearing throughout the day in healthcare settings can be difficult. In CNUH, mask wearing compliance in patients/caregivers was not high (personal communication). A study of mask use in health care settings found that respiratory pathogens on the outer surface of used medical masks may result in self-contamination, and the risk increases with increasing time of mask use (> 6 h).12 It is important for health authorities to provide clear guidelines for face mask wearing to increase compliance. Furthermore, it is necessary to implement hand hygiene and mask use improvement interventions targeting patients/caregivers, as well as HCWs.
During the quarantine of building 1, we generated management guidelines for ward cohorts including movement routes, patient room distribution principles, RT-PCR intervals, and patient care. During health crises such as epidemics, HCWs must work harder and for longer periods of time, and often do so in a context where knowledge and understanding of the novel pathogen is still in its infancy. Unexpected outbreaks with nosocomial transmission bring fear and anxiety to HCWs, patients and caregivers. During the outbreak described in this study, it was important for HCWs to be supported, and to have clear management guidelines. Although our hospital already had manual about the public health crisis situations such as Table 1, in real practice, there were many miscommunications and difficulties. Actually, the infection control team was to act as a control tower and was burned out. By sharing our clinical experience, we hope that other hospitals facing COVID-19 outbreaks can enhance their preparedness and develop guidelines for caregivers, patients, and HCWs.
Our data reinforce the importance of multi-time point surveillance of asymptomatic HCWs, and of routine surveillance of patients and caregivers. Systems for the prevention of intra-hospital transmission should not be restricted to the hospital alone. Basic infection control policy (mask use, hand hygiene and social distancing) should also be implemented at the community level.
 XML Download
XML Download